 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
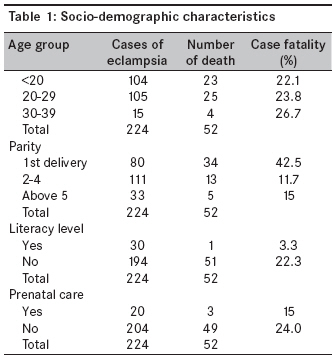
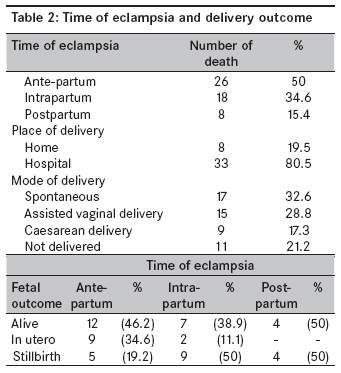
Annals of African Medicine, Vol. 8, No. 2, April-June, 2009, pp. 81-84 Original Article A 5-year review of maternal mortality associated with eclampsia in a tertiary institution in northern Nigeria Kullima AbubakarAli, Kawuwa MohammedBello, Audu BalaMohammed, Usman Hadiza, Geidam AdoDanazumi Department of Obstetrics and Gynaecology, Federal Medical Centre Nguru Code Number: am09019 PMID: 19805936 Abstract Objective : To determine the incidence of maternal mortality associated with eclampsia and to determine how socio-demographic and clinical characteristics of the women influence the deaths.Methodology : Records of 52 eclampsia-related mortalities from January 2003 to December 2007 were reviewed, retrospectively. Their social demography, mode and place of delivery, time of eclampsia, and fetal outcome were extracted for analysis. Results : Eclampsia accounted for 52 (46.4%) of the 112 total maternal deaths recorded within the 5-year period, with case fatality of 22.33%. Age group <20, 20-29 and above 30 all had similar case fatality rate of 22.1%, 23.8% and 26.7%, respectively. Those who were experiencing their first deliveries have the worst deaths recording 42.5% of the case fatality in that category. As expected, unbooked had higher case fatality of 24.0% compared to 15% among booked cases, while those with no formal education also had more death (22.3% case fatality) as compared to 3.3% among those who had some form of formal education. Antepartum eclampsia was the cause in 50% of the death, 11(21.2%) of the pregnancies were not delivered before their death, while 18 (34.6%) were stillbirth. Conclusion : Eclampsia still remains the major cause of maternal mortality in this region resulting from unsupervised pregnancies and deliveries. There is need to educate and encourage the general public for antenatal care and hospital delivery. Keywords: Eclampsia, maternal mortality, northern Nigeria Résumé Objectif: Pour déterminer l’incidence de la mortalité maternelle associés à éclampsie et pour déterminer comment
caractéristiques sociodémographiques et cliniques de l’infl uence de femmes le décès. Mots cles: éclampsie, la mortalité maternelle, Nord du Nigeria Introduction Eclampsia remains a complication of pregnancy and a leading contributor to maternal and perinatal morbidity and mortality. [1],[2] Worldwide [3] it accounts for 50,000 maternal deaths annually. In spite of the several global and regional interventions and initiatives from governments and other concerned agencies, maternal mortality continues to rise in sub-Saharan Africa with eclampsia as a major cause. [4],[5] Over the last decade it remained the leading cause of maternal and perinatal mortality in Nigeria, [6],[7],[8] This picture could even be worse especially in the north-eastern part of Nigeria with so far, the worst case fatality rate of 11.6% (11,600/100,000) as reported in Gombe. [9] This study was undertaken to determine the incidence of eclampsia-related death in the study population, the socio-demographic characteristic of the women and pregnancy outcome. Materials and Methods This is a retrospective study of maternal deaths from eclampsia recorded in Federal Medical Centre Nguru over a 5-year period, from January 1, 2003 to December 31, 2007. Out of the 112 total maternal deaths recorded over the study period, records of 52 patients who suffered from eclampsia-related deaths were retrieved from the medical records library, and information pertaining to their age, parity level of education and booking status was obtained. Information on the mode of delivery, time of eclampsia, fit controlled and gestational age at delivery, place of delivery, and fetal outcome were also obtained from the records for analysis using SPSS version 11. The Chi-square test was used for test of significance. Results During the period under review, a total of 3931 deliveries were recorded, 224 cases had eclampsia, giving a prevalence rate of 5.7% of the total deliveries. Diazepam is the sole anticonvulsant used for all the cases. Total deaths from eclampsia were 52 out of the 112 maternal death over the same period accounting for 46.4% of the total maternal death and a case fatality rate of 22.3% (22,300/100,000) and eclampsia-related maternal mortality ratio (MMR) of 1322/100,000 deliveries. As shown in [Table - 1], age group < 20, 20-29, and above 30 all had similar case fatality rate of 22.1%, 23.8%, and 26.7%, respectively. Those who were experiencing their first deliveries have the worst deaths recording 42.5% of the case fatality in that category. As expected, unbooked had higher case fatality of 24.0% compared to 15% among booked cases, while those with no formal education also had more death (22.3% case fatality) as compared to 3.3% among those who had some form of formal education. [Table - 2] illustrates the type of eclampsia and delivery outcome. About 50% of the victims had ante-partum eclampsia, while intrapartum and postpartum eclampsia were found among 34.6% and 15.4%, respectively. Surprisingly, 80.5% of the eclamptics delivered within the hospital environment, and 19.5% were cases of postpartum eclampsia and whose deliveries were conducted at home. Of those whose deliveries that were conducted in the hospital preterm and term deliveries were proportionally similar, but in majority the gestational age were estimated based on the fundal height at the time of presentation rather than by date or with the use of ultrasound scan. Spontaneous vaginal delivery, assisted vaginal delivery, and caesarean section were the modes of delivery of the pregnancies in 17 (32.6%), 15 (28.8%), and 9 (17.3%), respectively. Fit controlled was achieved in 47 (90.4%) of the cases, with diazepam as the anticonvulsant. Recurrence of fit was observed in three of the cases before their eventual death. Eleven of the mothers died undelivered giving a maternal mortality ratio of 279.8/100,000 deliveries, while the remaining 41 patients: 23 were live births, while 18 were stillbirths. The relationship between fetal outcome and time of eclampsia is also shown in same [Table - 2]; in those who experienced ante-partum eclampsia, 12 of the neonates were delivered alive, accounting for 46.2% of the live births, while intrapartum and post-partum 7 and 4 live births were found. Only 19.2 of stillbirths occurred in the ante-partum group compared to 50% in each of the intrapartum and postpartum eclamptics. Discussion During the 5-year study period, out of the 224 cases of eclampsia, 52 maternal deaths were recorded, giving case fatality rate of 22.3% which is significantly higher than reported in India (7.8%) [10] and other parts of Nigeria [Benin (10.7%), [11] Gombe (11.6%), [9] Ukpoma (15.4%) [6] and Jos (16.9%) [12] ]. The eclampsia-related maternal mortality ratio of 1322/100000 deliveries found was however lower than reported in Uyo (6800/100000). [13] There was no much significant difference in case fatality among the reported groups < 20, 20-29, and above 30 years with 22.1%, 23.8%, and 26.7%, respectively. Two-third of the death were of those experiencing their first deliveries which is not unexpected because the reported incidences of eclampsia is much higher in this group of patients. [9],[12],[14],[15],[16] Almost all the mothers not had any formal education that is not surprising, as there is apathy toward western education, particularly for girls′ and children education with subsequent early marriage. The poor/lack antenatal supervision in majority, who were only rushed to the hospital at terminal stages of the emergency, may account for more deaths. This was similar to findings in the Niger Delta region of Nigeria. [6]. Because of the peculiarity of these patients (unbooked and illiterates in majority), gestational age was either estimated in months or extrapolated from the fundal height measurement at the time of examination, this often lead to problem of decision making at mode of delivery when fetal survival is to be considered. Maternal death is higher among those who experienced antepartum eclampsia compared to those who had intrapartum or post-partum eclampsia. This could be partly explained by the relatively longer duration or possibly repeated episodes of convulsion from the onset of the first fit that often increased the risk of mortality. The observed maternal mortality ratio in this study of 279.8/100,000 deliveries was much higher than reported from Kaduna Nigeria of 141/100,000. [17] However, there is no much significant difference between live births and stillbirths, but the stillbirth rate of 34.6% is similar to findings in Jos of 31.7%. [12],[16],[18] Compared to those with other forms of eclampsia, neonatal outcome is relatively better among those with antepartum eclampsia; this might not be unconnected with the earlier recourse to caesarean section that might tend to minimiz further risks to both the mother and the fetus from repeated convulsions and its consequences. Conclusion Eclampsia no doubt contributes significantly to maternal mortality in Nigeria, more so in our geopolitical zone. Effort should be made by all concern to improve facilities and social infrastructures that will directly or otherwise minimize the occurrence of eclampsia. Skilled and prompt attendant of patient in emergency situations will help to curtail mortalities from preventable morbidities. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09019t1.jpg] [am09019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}