 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 8, No. 2, April-June, 2009, pp. 95-99 Original Article Operative vaginal deliveries in Zaria, Nigeria Adaji SE, Shittu SO, Sule ST Department of Obstetrics and Gynaecology, Ahmadu Bello University Teaching Hospital Zaria Code Number: am09022 PMID: 19805939 Abstract Background : Operative vaginal deliveries are frequent features of obstetrics practice in tertiary levels of care even in developing countries. It is essential to review these practices in order to assess their benefits or otherwise to safe motherhood in resource limited settingsStudy design : Labor records on operative vaginal delivery cases and matched controls who had spontaneous vaginal deliveries between January 1997 and December 2001 at the Ahmadu Bello University Teaching Hospital, Zaria, Nigeria, were analyzed with respect to mode of delivery, indication for operative vaginal delivery, anesthesia use, fetal 5-min Apgar score, birth weight, fetal, and maternal complications. Results : Of 7,327 deliveries at the center in the study period, 262 (3.6%) were by operative vaginal deliveries. Forceps delivery was most frequently performed (55.7%), while vacuum delivery was found to be in increased use (38.2%). Embryotomy procedures were performed selectively (6.1%). Operative vaginal deliveries were more commonly employed on primigravida (78.6%) compared to multiparas and the most common indication was delayed second stage of labor. Forcep- and vacuum-assisted deliveries were both associated with maternal and newborn complications. There was no significant difference in the use of anesthesia between forceps and vacuum deliveries. Conclusion : Operative vaginal delivery rates in this center are comparable to other centers as are the possible complications. Making these procedures safer will improve safe motherhood in settings where there are performed. Keywords: Embryotomy; forceps and vacuum deliveries; symhyseotomy Résumé Arrière-plan: Dispositif livraisons vaginales sont fréquentes fonctionnalités d’obstétrique pratique en tertiaire niveaux de soins de même dans les pays en développement. Il est essentiel de revoir ces pratiques afi n d’évaluer leurs avantages ou autrement à sécuritaire maternité dans ressource limitée paramètre Plan d’étude: Du travail des enregistrements sur conscient cas de livraison vaginale et contrôles jumelés qui avait
spontanée vaginale livraisons entre janvier 1997 et décembre 2001 à l’Ahmadou Bello Université enseignant Hospital,
Zaria, Nigéria, ont été analysés quant aux mode de livraison, indication pour dispositif livraison vaginale, utilisation de
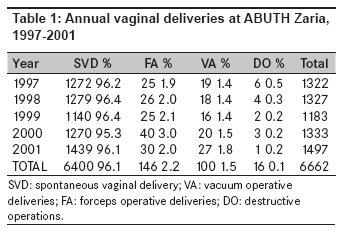
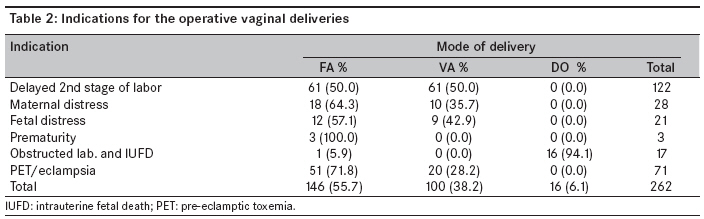
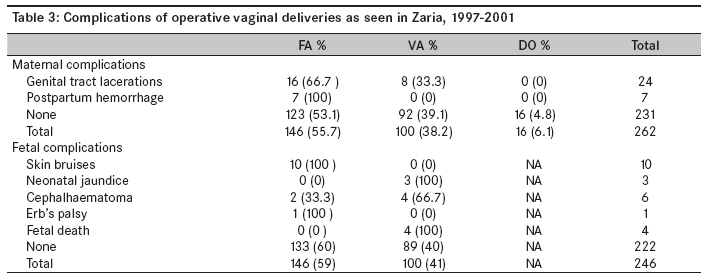
l’anesthésie, score d’Apgar de cinq minutes du foetus, poids de naissance, les complications du foetus et maternelles. Mots cles: forceps and vacuum livraisons; Symhyseotomy; Embryotomy Introduction Operative vaginal delivery, a vital component of basic emergency obstetric care worldwide remains an integral part of the obstetrician′s duties. It may take the form of instrumental deliveries, employing obstetric forceps and vacuum extractor to shorten the second stage of labor or operative procedures like symphysiotomy or destructive operations performed to achieve vaginal delivery in dystocias with or without a living fetus. [1],[2],[3] Although operative vaginal delivery may be performed, as infrequently as in 1.5% of deliveries in some countries, it may be as high as 15% in other countries. In the United Kingdom, the rates of instrumental vaginal delivery range between 10% and 15%; these rates have remained fairly constant, although there has been a change in preference of instrument. In the 1980s, most instrumental vaginal deliveries were by forceps, but by 2000 this had decreased to under a half. Much of the decline has been attributed to increasing preference for vacuum extraction or caesarean section when difficult vaginal delivery is anticipated. [2],[3],[4] Symphysiotomy and destructive operations are performed mainly in developing countries where obstetric care for many women is still rudimentary. [5] Among obstetricians in developing countries, including the center where this study was undertaken, outlet forceps delivery and vacuum extraction are used frequently to shorten the second stage of labor or address delays in second stage, for maternal and fetal indications. Destructive operations and symphysiotomy are also performed to relieve labor dystocias. The overall objective of these is to improve safe motherhood by reducing the contribution of second stage of labor complications to maternal mortality and morbidity. This study aims to review the experiences in operative vaginal deliveries in Zaria with a view to suggesting evidence-based practices that will help to achieve the goals of safe motherhood Materials and Methods This was a case-control study of operative vaginal deliveries performed at the Ahmadu Bello University Teaching Hospital Zaria over a 5-year period spanning January 1, 1997 to December 31, 2001. The operative vaginal deliveries reviewed were forceps delivery, vacuum delivery, symphysiotomy, and destructive operations (craniotomy, embryotomy, decapitation). The operative vaginal procedures were performed by resident doctors and consultants in the Department of Obstetrics and Gynecology. The obstetrics forceps used were the Wrigley′s forceps employed for outlet forceps delivery and Malstrom′s metal vacuum extractor with a manually operated suction pump was used for vacuum extraction. The subjects reviewed consisted of all parturients who underwent any of the above-mentioned procedures over the stated period at ABU Teaching Hospital, Zaria. The control subjects were randomly selected parturients who had spontaneous vaginal deliveries at the delivery suite of hospital over the same period of time. Cases and controls were matched for age, parity, gestational age at time of labor and delivery, and fetal birth weight with the study group. All deliveries during the study period were reviewed and the total operative delivery rates were calculated. The birth records of the parturients who underwent operative vaginal deliveries and an equal number of randomly selected parturients who had spontaneous vaginal deliveries and who meet the criteria for inclusion into the control group were retrieved. Information extracted included the mode of delivery (spontaneous vaginal, outlet forceps and vacuum deliveries, symphysiotomy and destructive operations), indications and complications of each procedure, gestational age at the time of delivery, infant 5-min Apgar score, and birth weight. The data obtained were analyzed using descriptive statistics and the Minitab statistical software package. Results Prevalence and types of operative vaginal delivery procedures A total of 7,327 deliveries were conducted between January 1997 and December 2001. Operative vaginal delivery techniques were employed in 262 cases giving the operative vaginal delivery rate of 3.58% over the study period. [Table - 1] shows the details. The operative vaginal delivery procedures performed were forceps deliveries, vacuum deliveries, and destructive operations (craniotomy, embryotomy and decapitation all on dead fetuses). No case of symphysiotomy was recorded. As shown in [Table - 1], forceps delivery was the most frequently performed procedure during the period with rates ranging from 1.9 to 3.0%. Vacuum delivery was shown to be gaining more popularity, while destructive operative rates were on the decline. Parity of clients The majority (78.6%) of the parturients who were delivered by an operative vaginal delivery procedure were primigravida. Most (68.7%) of the operative procedures were performed at term, while 31.3 % were preterm. Among preterm infants, 76.8% were delivered by forceps. Indications for operative vaginal deliveries The most common indications for instituting operative vaginal deliveries as shown in [Table - 2] were delayed second stages of labor and pre-eclampsia/eclampsia. Complications The maternal and fetal complications of operative vaginal delivery seen during the study period are as presented in [Table - 3]. Overall, operative vaginal delivery had a complication rate of 21.6% (11.8% maternal and 9.8% fetal) as compared to a complication rate of 12.7% found among parturients who had spontaneous vaginal delivery. In the case of forcep-assisted deliveries, 15.8% of mothers who had the procedure-developed complications, while for vacuum-assisted deliveries 8% of the mothers sustained a complication. On the other hand, 8.9% of newborns delivered by forceps had complications, while vacuum-assisted delivery was associated with complications in 11% of newborns. As shown in [Table - 3], skin bruises were commonly associated with forceps delivery and neonatal jaundice and cephalhaematoma were found to be commonly associated with vacuum deliveries. There were four fetal deaths following vacuum deliveries. The absence of postmortem reports, however, made it difficult to ascertain the exact complication that lead to the deaths. Severe asphyxia was observed only in one infant following spontaneous vaginal delivery. However, 38.2% infants delivered following forceps or vacuum delivery had depressed 5-min Apgar scores. Fetal birth weights The birth weights of infants ranged between 1.5 and 4.0 kg. Operative vaginal deliveries were mostly performed among infants weighing 2.52-3.99 kg. Forceps delivery was most frequently performed in low birth weight infants (59.6%). Anesthesia The various forms of anesthesia used included local anesthesia (perineal infiltration and vulval ring block) sedation with diazepam, combination of chlorpromazine, pethidine and promethazine as lytic cocktail, pentazocine, and spinal and general anesthesia. These were commonly employed in parturients that underwent operative vaginal deliveries and were required more commonly in clients who had forceps deliveries. There was, however, no significant difference in the use of anesthesia between forceps and vacuum deliveries (x2 = 0.711, DF = 3, P = 0.8706) Discussion The operative vaginal delivery rate of 3.6% found in this study is similar to rates found in other centers worldwide. Specifically, the prevalence rates of 1.9-3.0% for forceps delivery; 1.4-1.5% for vacuum delivery, and 0.1-0.5% for destructive operations agree with those from previous studies. [6],[7],[8],[9],[10],[11],[12],[13] The increasing frequency of use of vacuum delivery as revealed in this study conforms to a similar trend observed in other centers. [5],[6],[7] This trend may be attributable to its relative safety, lower risk of maternal trauma, less propensity to resort to caesarean sections, less peri- and postpartum blood loss, and less need for analgesia. [11],[12],[13],[14] The procedure is also easy to learn. Destructive operations are increasingly less utilized worldwide and the trend in this study also reflects this. This reducing popularity may be due to dearth of suitable cases for their application, more liberal use of caesarean deliveries, lack of skills, or negative attitude of obstetricians. [15],[16] The findings in this study could be a reflection of diminution in suitable cases for the procedure or reluctance in their application as the skills are available in this center. Most authors agree though that destructive operations still have a place in obstetric practice in developing countries. [17],[18],[19] With a mean age of 23.5 years, most of the parturients who had operative vaginal deliveries were adolescents and young adults. This study also revealed that operative vaginal deliveries were more frequently performed in primigravida, who constitutes 78.6% of parturients in this study. Similar observations were made by Kabiru et al and Adefuye et al, and may not be unconnected with the higher tendency to second stage delays in primigravida, [10],[20] which was the most common indication for operative vaginal delivery in this study. Tight, untested lower genital tracts, undue anxiety, and inexperience in labor among young aged primigravids no doubt accounted for the higher frequency of this diagnosis. The other indication for operative vaginal delivery procedures was maternal illness mainly due to pre-eclampsia and eclampsia. Similar indications have been reported from other centers in Nigeria where women have demographic and obstetrics characteristics similar to Zaria. [8],[20] The complication profile found in this study concurs with those found by most authors with higher risk of maternal complications associated with forceps deliveries and higher risk of fetal complication associated vacuum deliveries. However, a lot of workers report insignificant differences in fetal injuries sustained following either forceps or vacuum deliveries. [11],[12],[13] Depressed 5-min Apgar scores were observed more frequently in infants delivered by an operative vaginal delivery procedure. This compares to the findings of various studies and may not be truly attributable to the procedure as the asphyxia may be the outcome of the events of labor that indicated the intervention than from the operative vaginal procedure itself. The hypothesis advanced by Towner et al, supports this view. They found in their series that substantial fetal morbidity previously attributed to operative vaginal delivery was due to the process of labor. [21] This study like previous ones attests to the high effectiveness and safety of vacuum delivery in assisting vaginal delivery as compared to forceps delivery. The adoption of vacuum extraction as the first choice procedure for operative vaginal delivery should therefore be promoted. In settings with little or no experience with the use of vacuum extraction, training programs at residency and senior levels are recommendable in order to attain satisfactory skills. As much as possible, training programs should be based partially on simulated situations, and while achieving the minimum skills, the professionals in training should not use vacuum extraction in real patients. [22] Reducing operative vaginal delivery rates through preventing the indications for their use no doubt will also help to improve outcome for both mother and infant. Various techniques may help to achieve this; these include companionship in labor, active management of the second stage of labor with syntocinon, upright posture for the parturient with use of the birth cushion, or undertaking fetal scalp blood sampling rather than expedited delivery when fetal heart rate decelerations occur. When epidural analgesia is used, allowing time for the analgesic effect to wear off or having more liberal approach to the length of the second stage also reduces the need for operative delivery. [22] References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09022t3.jpg] [am09022t2.jpg] [am09022t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}