 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 8, No. 2, April-June, 2009, pp. 100-104 Original Article Treatment outcomes among pulmonary tuberculosis patients at treatment centers in Ibadan, Nigeria Fatiregun AkinolaA, Ojo AbimbolaS, Bamgboye AfolabiE Department of Epidemiology, Medical Statistics and Environmental Health, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan Code Number: am09023 PMID: 19805940 Abstract Objective : To assess treatment outcomes and determinants of outcome among tuberculosis patients.
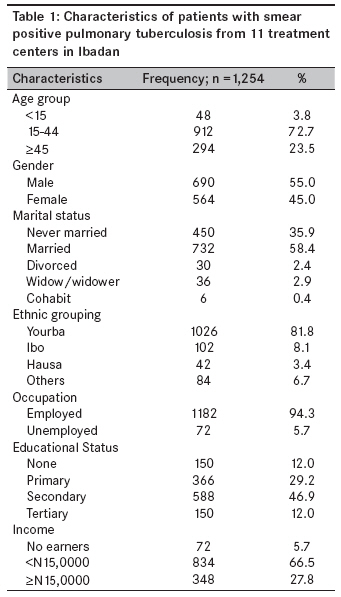
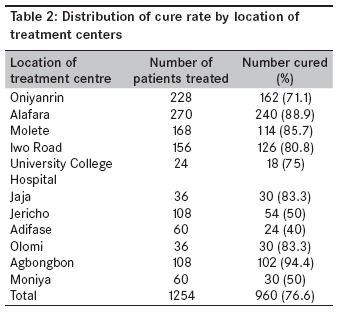
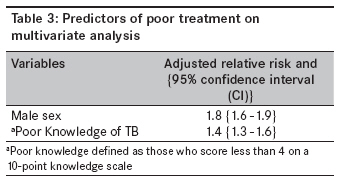
Keywords: Pulmonary tuberculosis; treatment centers; treatment outcome Résumé Paramètre: Centres de traitement de la tuberculose en Ibadan, Nigeria Introduction Effective tuberculosis (TB) treatment has been shown to have a significant effect on the control of TB. Completion of treatment of active cases is therefore the most important priority of TB control programs. [1] Guidelines suggest a target treatment completion rate of 85% for infectious cases. [2] In 1994, the World Health Organization (WHO) estimated the rate of treatment success to vary from 77% in areas instituting WHO TB control strategies, which include the use of directly observed therapy, to 41% in areas without such strategies. [2] In Nigeria, the treatment success rate was 79% in 2002; this increased to 85% in 2003. The default rate remained as high as 11% in the 2-year period, while the death rate was 6.7%. [3] In Ilorin, a northcentral town, a 43.7% cure rate and a 44.2% default rate were found in a 9-year review of records of TB cases. [4] A similar study in Ife, a southwest town, showed that 73% of patients completed treatment, while 27% defaulted at some point. [5] The treatment success rate has not been published for Ibadan, the largest city in Nigeria. Moreover, Nigeria has the highest estimated number of new TB cases among the African countries (200,000 annually). [6] The treatment of TB in Ibadan, like any other part of the country, is organized to follow the National Tuberculosis and Leprosy Control Programme (NTBLCP) guidelines. Although, completion of treatment is monitored primarily by the Public Health Unit, information on treatment outcomes is rarely reported. Poor treatment outcome has serious consequences, including ongoing infectivity and development of drug-resistant Mycobacterium tuberculosis. No reliable way exists to predict which patient will complete TB treatment; however, failure to complete treatment has been associated with alcohol abuse, drug abuse, and homelessness. [7],[8] Also, patients with AIDS have been found to be more likely than those without AIDS to complete treatment. [7] The extent to which other factors, including program quality, influence the outcome of treatment has not been explored. The objective of this study, therefore, was to assess treatment outcomes and its determinants among smear-positive pulmonary TB patients attending treatment clinics in Ibadan, Nigeria. Materials and Methods The study was carried out in Ibadan, the capital of Oyo, one of the 36 states of the Federal Republic of Nigeria. Oyo is located in the southwest geopolitical zone of the country. The city covers an estimated 150 sq km and a population of over three million in the year 2000. [9] The Oyo State Leprosy and Tuberculosis Control Unit, which has been in existence since the colonial era, was reactivated in 1991 during the formal launching of the NTBLCP. It is supported technically and financially by the Damien Foundation of Belgium. The treatment of TB is decentralized in Ibadan to increase accessibility, like in other parts of the state. There are 11 TB treatment centers throughout the city. All the centers are located within primary health care centers, except those affiliated with Jericho Chest Hospital and the University College Hospital (UCH), which are specialist health facilities. Treatment regimens and procedures, including laboratory diagnosis, are guided by the National Policy on TB and Leprosy Control. [6] A longitudinal study design was utilized. All patients who were sputum smear-positive at the initiation of treatment at all of the 11 treatment centers were followed up until the completion of treatment in the eighth month. The instruments used for the collection of data included a data collection format and a structured interviewer-administered questionnaire. The data collection format was used to extract data from the patient`s record, while the structured questionnaire obtained data regarding the patients` knowledge of TB, drug treatment, and other factors likely to affect treatment outcome, such as compliance with clinic appointments, family support, and the duration of illness. Follow-up information was obtained on a monthly basis. The main variable analyzed was the treatment outcome. Treatment outcome definitions, adapted from an international standard classification, [10] were as follows: (1) cured (a smear-positive patient based on the medical record, who had a negative sputum smear during the eighth month of treatment and on at least one previous occasion); (2) died (a patient who died during treatment irrespective of cause); (3) failed (a smear-positive patient who remained smear-positive at the fifth month of treatment); (4) defaulted (a patient who did not come back to complete chemotherapy and there was no evidence of cure through the sputum result during the fifth month of therapy), (5) treatment interruption (a patient who did not collect medications for 2 months or more at a particular time or at interval, but still come back for treatment and in the 8 th month of treatment, the sputum result was positive), and (6) transferred out (a patient who was transferred to another treatment center and for whom treatment results are not known). A Chi-square test was used to evaluate differences in categorical variables. The Fisher′s exact test was used when cell sizes were < 5. The Student t-test was used to compare continuous variables, and logistic regression analysis was performed to identify predictors of poor treatment outcome. Poor treatment outcome was defined as those patients with treatment failure, treatment default, treatment interruption, patients who transferred out or patients who died while receiving treatment. The knowledge score was computed from 10 items on knowledge about the disease, prevention, and treatment. Poor knowledge was defined as a score < 4. A multivariate model was constructed using factors that were found to be significant (a P value < 0.05) on univariate analysis. Data analysis was carried out with SPSS, version 11. Informed consent was obtained from study participants and ethical approval was obtained from the University of Ibadan and the UCH (UI/UCH) Institutional Review Committee before embarking on the study. Results A total of 1,254 patients were enrolled in the study. The mean age was 35.0±3.3 years. The patients were predominantly of Yoruba descent (82%). The majority of the patients was males (55.0%) and married (58.4%). Although a high proportion of the patients (94.3%) were employed, the majority (66.6%) earned less than N15, 000 per month [Table - 1]. The percentages of patients with treatment outcomes assessed in the study were as follows: cured (76.6%), failed (8.1%), defaulted (6.6%), treatment interruption (2%), transferred out (4.8%), and died (1.9%). Treatment outcomes varied significantly between health centers, with the Adifase Treatment Centre having the lowest cure rate (40%) and the Agbongbon Treatment Centre having the highest cure rate (94.4%). The treatment centers located in the specialist hospitals at Jericho and the UCH had 50 and 75% cure rates, respectively [Table - 2]. The mean age of the cured patients (31.2±3.1 years) was significantly lower than the mean age of those with a poor treatment outcome (36.7±3.5 years; P< 0.05). On multivariate logistic regression, factors that were found to predict poor treatment outcomes included male gender (adjusted RR 1.8; 95% CI: 1.62-1.94) and poor knowledge of TB (adjusted RR 1.35; 95% CI: 1.25-1.62; [Table - 3]). Discussion Any treatment outcome in which a cure is not established, i.e. sputum conversion to negative among active TB cases, will pose a danger to the community; hence, prevention of such occurrences is necessary to maximize the efficiency of TB control programs. The finding herein that TB primarily affects the young age group was consistent with previous reports in developing countries. [5],[11],[12] However, TB has been reported to be two-to-four times more prevalent among the elderly age group in developed countries. [13] Also, the observation that a greater percentage (55%) of the patients in this cohort was males is consistent with other reports. [4],[14] TB is closely associated with poor living conditions, poverty, and low socioeconomic status. Although the majority of the patients in this study were employed (94.3%) and had a post-primary education (58.9%), most (72.2%) were earning < N15, 000.00 a month. This is consistent with the report from Ife [5] in which low socioeconomic status, overcrowding, and poor living conditions were identified as major risk factors in the development of pulmonary TB. The cure rate of 76.6% found in this study is below the recommended target of 85% by the WHO. [3] Even if those who were transferred out were cured, the cure rate may not have been better than was estimated. The HIV status of the patients was not known because HIV screening tests were not routinely carried out; hence, our estimate could not be attributed to the prevalence of the infection among the study population. However, the estimated cure rate is close to the cure rate of 73% among pulmonary TB patients in the Obafemi Awolowo University Teaching Hospital (OAUTH) in Ile Ife. [5] The cure rate varied significantly between the treatment centers. The treatment centers with the lowest and highest cure rates were manned by primary health care workers. Cure rates of 50 and 75% were found for treatment centers located within the specialist hospitals at Jericho and the UCH, respectively. Although the care patients received in these centers may not necessarily represent TB management in the community, it is thought to be superior given that these are tertiary health centers. There is thus a need to study health centre-specific challenges to a high cure rate in our environment. In Montreal, [1] for example, it was found that university-affiliated centers adhered to recommended standard treatments only some of the time (in 25% of cases the initial treatment was a regimen not considered standard by current guidelines). The data revealed that males are at an increased risk of a poor treatment outcome compared to females. This is consistent with other published reports. [15],[16] Lienhardt et al, in 1998, reported that females were more likely to achieve a cure than their male counterparts. [15] Similarly, Diel et al, attributed poor treatment outcomes, such as default, failure, and death, to males. [16] Also, the risk of a poor treatment outcome was higher among those with poor knowledge. This is consistent with the report by Jaramillo that non-compliance and other treatment outcomes are associated with poor education of patients on TB therapy. [17] It is also consistent with the findings of Khan et al, that low knowledge of TB and therapy is a predictive factor of adverse treatment outcome among TB patients. [18] In conclusion, the findings provide a useful insight in understanding challenges to treatment outcomes. The cure rate among smear-positive pulmonary TB patients, though moderate, is less desirable, hence the need for stakeholders in TB control to intensify efforts in identifying and developing solutions. The poor knowledge identified in this study, as a barrier to higher cure rates among patients, could be modified by health education intervention. Variation in health centre treatment outcomes underscore the need for further research to identify centre-specific factors associated with poor treatment outcome. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09023t2.jpg] [am09023t1.jpg] [am09023t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}