 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 8, No. 3, July-September, 2009, pp. 147-155 Review Article A clinical and epidemiologic update on the interaction between tuberculosis and human immunodeficiency virus infection in adults Habib Abdulrazaq G Department of Medicine, Infectious and Tropical Diseases Unit, Bayero University Kano, Aminu Kano Teaching Hospital, PMB 3452, Kan Code Number: am09032 PMID: 19884690 Abstract Background : Tuberculosis (TB) is an important cause of mortality and morbidity in human immunodeficiency virus (HIV) infection in Africa. The interaction between TB and HIV infections is reviewed.Methods : Literature on TB, HIV and their co-infection, especially in sub-Saharan Africa, including Nigeria, is reviewed. Results : Burden of TB is fueled by the HIV epidemic, and clinical presentation of TB may be atypical with co-infection. Recommendations on drugs and timing of antiretroviral therapy (ART) initiation are discussed. Use of cotrimoxazole prophylaxis (CPT) in co-infected patients reduces morbidity and mortality, while the principles of TB prevention in HIV infection can be summarized with the three I's: intensive TB case finding and surveillance, isoniazid preventive therapy (IPT) and infection-control measures; to these can be added a fourth 'I,' viz., instituting ART. Clinical complications like drug resistance, toxicity and drug interactions; and immune reconstitution inflammatory syndrome (IRIS) with CPT, IPT and ART are highlighted. Emergence of drug-resistant- and nosocomial- TB in HIV infection poses serious challenges and potential consequences in Africa, and appropriate measures are recommended. Conclusions : Many barriers exist for optimizing the care of the two diseases, but the aim should be strengthening capacities, collaborations, linkages and eventually integrating the services. Interventions for TB prevention in HIV infection should be widely implemented. Keywords: Antiretroviral Therapy, Drug Resistance, Human Immunodeficiency Virus, Nosocomial, Preventive therapy, Tuberculosis Résumé arrière-plan: La tuberculose (TB) est une cause importante de mortalité et morbidité en homme Infection de virus
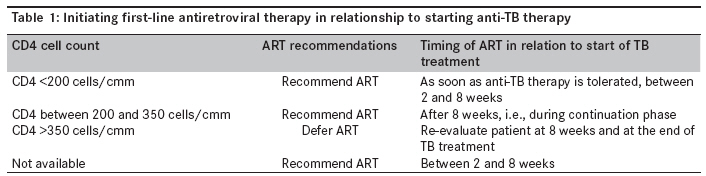
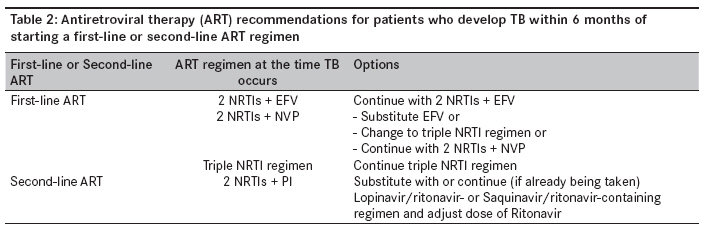
(VIH) de l’immunodéfi cience humaine en Afrique. L’interaction entre TB et l’infection à VIH est examinée. Mots cles: Antirétroviral thérapie, drug résistance, nosocomiale, la tuberculose, thérapie preventive, Virus d’immunodéfi cience humaines "We can not fight AIDS unless we do much more to fight TB as well." Introduction In sub-Saharan Africa, the resurgence of tuberculosis (TB) is fueled by the human immunodeficiency virus (HIV) infection. [1] Nigeria has the third highest burden of HIV, with sero-prevalence of 4.5%; and the fifth highest burden of TB globally. [1],[2] Rapid expansion of anti-retroviral therapy (ART) programs is happening in Nigeria and Africa in general, but TB control has yet to adapt to the new climate of ART availability. Many barriers exist in the management of HIV-TB co-infection, and they include deficiencies in knowledge of health care workers, drug interactions and traditional differences in the way TB and HIV services are provided. Failure to successfully integrate the two services will threaten the viability of both programs in a continent already besieged by the two diseases. Here, clinical and epidemiologic aspects of the interaction between TB and HIV in adults are reviewed with the aim of enlightening practitioners and health policy makers on the nature of the interaction and the best management and prevention strategies. Clinical and epidemiologic aspects of TB-HIV interaction One third of the world is infected with TB but 9.2 million people developed active TB, out of which 1.7 million died in 2006. [1] The resurgence of TB is fueled largely by HIV infection. The lifetime risk of developing active TB in HIV-negative individuals is approximately 10%; but the annual risk among HIV-infected patients is ~10%, while the lifetime risk approaches 50% among them. [1],[3] When HIV was emerging in the early 1990s in Nigeria, 2% of TB patients were HIV infected, but the co-infection rate rose to 21%-29%. [1],[4],[5] Clinically, in early HIV infection with minimal or no immune-suppression, pulmonary TB (PTB) presents typically, as in immune-competent individuals, with apical fibrosis and cavitations. In advanced HIV infection, however, apical predilection and fibro-cavitary disease become uncommon; chest radiographs show alveolar reticulo-interstitial infiltrates in lower and mid zones of the lung. The proportion of extra-pulmonary tuberculosis (EPTB) is higher in HIV infection, especially with advanced immune-suppression. [1],[5],[6] Common EPTB forms include adenitis, pleurisy, TB abdomen, meningitis and disseminated disease. Infectiousness and transmission are less in TB-HIV co-infected patients compared to HIV-negative patients, especially in EPTB or disseminated disease; the sputum smear yield and duration of smear positivity are much lower. [6] Among HIV-infected patients not on ART, TB was the commonest cause of adult hospitalization, accounting for 29% of HIV admissions in Zaria, Nigeria, [5] as HIV patients are much more vulnerable to infection and reactivation. Similarly, it is the commonest cause of death in hospitalized HIV-infected adults in sub-Saharan Africa (Kano-Nigeria, Cote d′Ivore, Zaire), accounting for 33%-41% of mortalities without ART. [7],[8],[9] Morbidity and mortality risks of TB significantly decrease with ART but remain higher in the first 6 months of initiation than during the subsequent time on therapy. [10] It was the second most frequent cause of morbidity (38%) in West Africa, [8] and its incidence remains high in TB-high-burden countries even with ART use. Also, it was the third major cause of in-program deaths in South Africa; although in rural Malawi, it was not found to be a risk factor for high early mortality in patients on ART. [11],[12] Optimum time to initiate antiretroviral therapy in co-infected patients Antiretroviral therapy (ART), which uses highly active combinations of drugs, improves survival in human immunodeficiency virus (HIV)-infected persons. [10] HIV-infected persons in Nigeria and across Africa now have access to ART, but physicians often do not prescribe it to HIV-infected tuberculosis (TB) patients because of concerns about drug-drug interactions, overlapping toxicities, immune reconstitution inflammatory syndrome (IRIS), and suboptimal adherence resulting from higher pill burden. But the overriding factors that guide optimal timing decisions include the excess mortality risk resulting from delayed ART versus the excess mortality risk from IRIS, which is associated more with early ART. [13] Thus the actual ART commencement time during TB treatment remains poorly defined although expert groups and the Word Health Organization (WHO) recommend that public health programs make treatment of TB the first priority and ideally begin ART after anti-TB treatment (ATT) is tolerated and CD4 cell count is measured [Table - 1]. [10] To date there have been no randomized clinical trials to address the issue. But some observational studies have now documented that ART reduces the likelihood of death during ATT of HIV-infected TB patients; though many of the studies relied on retrospective data collection, occurred outside routine public health programs, or involved Asian or resource-rich countries without large TB or HIV epidemic. [14],[15],[16] In South Africa, a study on mortality among TB patients (n= 73) in the Gugulethu clinic from the time of enrollment until 4 months of ART with a median interval between TB diagnosis and initiation of ART of 42 days, found that of the 14 deaths, 10 (71%) were among patients waiting to start ART and only 4 (29%) occurred during ART. [14] Similarly, in Thailand, mortality occurred in 5/71 (7%) patients among those who received ART compared to 94/219 (43%) among those who did not; 80% reduction in the odds of death was found with ART commencement even after adjusting for CD4 cell counts, smear status, co-trimoxazole use and treatment facility. [15] A decision analysis using hypothetical cohort of 1000 HIV-infected adults with TB and CD4 counts less than 200/cmm has been developed to guide optimum timing of ART initiation, but unfortunately input data was not representative of sub-Saharan Africa realities. [17] North American data from Tuberculosis Trial Consortium Study 23 was used, where the overall mortality risk among patients with HIV-associated TB was just 2%-3% after 12 months, and the mortality risk associated with delayed ART was thus small. [16] What ART regimen to start? The recommended first-line ART regimen comprises 2 nucleoside reverse transcriptase inhibitors (NRTIs) plus 1 non-nucleoside reverse transcriptase inhibitor (NNRTI). There are few drug interactions between TB drugs and the 2 NRTIs, and no specific changes are recommended. The situation is more complex with the NNRTI class because NNRTI levels are reduced in the presence of rifampicin. [18],[19],[20] However, accumulating data support the use of first-line NNRTIs-containing ARV regimens in patients receiving rifampicin-containing treatment for TB. Here EFV is the preferred option, because the interactions with rifampicin are easier to manage; EFV blood levels are decreased in the presence of rifampicin, but this can be overcome by a dose increase from 600 to 800 mg daily; although in Thai patients, the two doses were found to lead to similar plasma levels, as well as immunologic and virological successes. [21] A second alternative is to use a triple NRTI regimen in patients undergoing TB treatment. Two triple NRTI regimens (zidovudine + lamivudine + abacavir and zidovudine + lamivudine + tenofovir) can be used safely with rifampicin. A third less favored option is the use of two NRTIs with nevirapine (NVP), though its level is decreased in the presence of rifampicin. However, given the high therapeutic index of NVP and the recent studies in South Africa and Thailand showing good short-term outcomes in antiviral activity and few adverse events in patients receiving the drug, standard NVP dosing is recommended. [10] As nevirapine toxicities are commoner with relatively high CD4 counts, regimens containing it should be avoided among such patients. Hepatotoxicity is a significant complication of both ART and ATT, and liver function should be monitored. Severe hepatotoxicity was found in 7.7 per 100 person-years in an African cohort; although in TB-HIV co-infected patients, ATT increased its risk by 8.5-fold. [22] Similarly, EFV should not be used during the first trimester of pregnancy or in women of childbearing potential unless effective contraceptive is ensured; otherwise, the latter two alternatives should be used for them. TB in patients already receiving ART There are two issues to consider in patients who are diagnosed with TB while on ART. The first concerns the modifications of ART, if any, which should be recommended for patients developing active TB within 6 months of initiating first-line or second-line ART. The recommendations made by WHO are summarized in [Table - 2]. [10] The second issue is whether the presentation of active TB on ART constitutes ART failure. In cohort studies, ART has been found to decrease the incidence of TB in treated patients by approximately 80%; in South Africa, the TB incidence rate was 3.5/100 person-years in the first year and significantly reduced with a trend during follow-up, reaching 1.01/100 person-years in the fifth year of HAART. [23] Rates of TB among treated patients nevertheless remain persistently higher than among HIV-negative individuals. [23] Furthermore, an episode of TB can occur across a wide range of CD4 cell counts and does not necessarily herald ART failure and the need to switch to second-line regimens. In addition, sub-clinical or undiagnosed TB often presents within the first 6 months after initiation of ART, frequently as part of IRIS. WHO therefore recommends that the following principles be applied when determining whether the development of TB on ART constitutes treatment failure. If an episode of TB occurs during the first 6 months following initiation of ART, this should not be considered a treatment failure event and the ART regimen should be adjusted for co-administration with rifampicin-containing regimens. If an episode of TB develops more than 6 months after ART initiation and data on the CD4 cell count and viral load are available, the decision about whether TB diagnosis represents ART failure is based on the CD4 cell counts and, if available, the viral load. Generally, extra-pulmonary tuberculosis (EPTB) should be considered indicative of ART failure, although simple lymph node TB or uncomplicated pleural disease may be less significant than disseminated TB. If there is good response to anti-TB therapy, the decision to switch to a second-line regimen can be delayed until short-course TB therapy has been completed. [6],[10] Co-trimoxazole prophylaxis for all TB-HIV-infected patients regardless of CD4 counts In a randomized controlled trial in Cote d′Ivoire, fewer deaths and hospital admissions were noted in the co-trimoxazole group compared to the placebo group, with decrease in mortality risk of 46% (95% confidence interval [CI], 23%-62%) and decrease in hospitalization of 43% (95% CI, 10%-64%) with significantly fewer admissions for septicemia and enteritis in the co-trimoxazole group compared to the placebo group. [24] This beneficial effect has been replicated elsewhere in Africa. [25] Despite provisional recommendations from the World Health Organization and UNAIDS that cotrimoxazole (CTX) prophylaxis be offered to all individuals living with AIDS, including HIV-positive patients with TB, [6] its routine use in developing countries, particularly Africa, has been minimal. Concerns were expressed regarding its effectiveness in areas of high bacterial resistance, that its widespread use might substantially increase bacterial cross-resistance in the community and that this intervention might promote resistance of malaria parasites to sulphadoxine-pyrimethamine. The benefits of co-trimoxazole justify its use, and it has rightly been recommended in the Nigerian National TB-HIV Strategic Guidelines. Co-infected patients should be given co-trimoxazole 960 mg daily or thrice weekly while anti-tuberculosis therapy (ATT) is administered. Immune reconstitution inflammatory syndrome in patients with TB who start ART The IRIS may present as a worsening of clinical disease after initial improvement. It results from restored ability to mount an inflammatory response associated with immune recovery. It can present with the signs and symptoms of a previously sub-clinical and unrecognized opportunistic infection, as a paradoxical worsening of treatment response several weeks into ART. [6],[26] In this sense, it is similar to, but more frequent than, the paradoxical reactions seen in immunocompetent patients on anti-TB therapy. [26] It may occur in up to a third of persons with TB who initiate ART and is associated with rises in CD4 cell counts . [27] IRIS typically presents within 3 months of the initiation of ART but can occur as early as 5 days. [6],[26],[27] TB-associated IRIS most commonly presents with fever and a worsening of pre-existing lymphadenopathy (in size or numerically), respiratory disease (acute respiratory distress or pleural effusion) or central nervous system disease (meningitis or increase and/ or expansion of lesions [tuberculomas]). In resource-constrained settings where diagnostic capacity is limited, a definition of IRIS is suggested based on 3 criteria: [26]
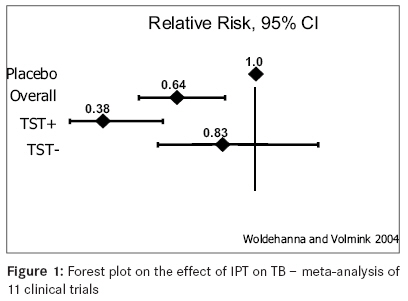
IRIS is probably more common if ART is started early in the course of TB treatment and in patients with low CD4 counts. [10],[13],[14] Most cases resolve without any intervention, and ART can be safely continued. Serious reactions such as tracheal compression, caused by massive adenopathy; or respiratory difficulty may occur. Therapy may require the use of corticosteroids. Drug-resistant TB-HIV co-infection - is it the perfect storm? HIV infection might potentially fuel multi-drug-resistant (MDR) TB, and the co-epidemic would have disastrous consequences. It is hypothesized that nosocomial transmission, malabsorption, acquired rifamycin resistance, poor treatment response, increasing TB incidence and deteriorating TB program performance in public health systems due to the HIV epidemic might potentially fuel MDR TB epidemic. [28],[29],[30] Although observations have not confirmed direct association between the organisms, reports of what came to be called extensively drug-resistant (XDR) TB in HIV have been most alarming. XDR TB is caused by Mycobacterium tuberculosis resistant to isoniazid and rifampicin (which defines MDR TB) in addition to a fluroquinolone and at least one of the following 3 injectable drugs: capreomycin, kanamycin and amikacin. In early 2005, physicians at a rural hospital in KwaZulu-Natal, South Africa, observed 53 patients with XDR TB; of these, 55% had primary infection with XDR strain of M. tuberculosis, two thirds had recently been hospitalized and all 44 who underwent testing were HIV positive. All but one (52/53 [98%]) died of TB, with a median survival period of only 16 days from the time the first sputum specimen was collected. [28] Limited studies in Nigeria failed to establish an association between drug-resistant TB and HIV infection but surveillance should be continued. [31],[32] The management of MDR TB is more costly, uses scarcely available medications, takes a longer time , is done with more drugs and higher pill burden, and entails use of more toxic agents; clearly, it can compound management of HIV infection and overwhelm care of both diseases. Typically, it entails use of 5 drugs (kanamycin, cycloserine, prothionamide, ofloxacin, pyrazinamide) for a 6-month intensive phase followed by an 18-month continuation phase with 4 drugs (cycloserine, prothionamide, ofloxacin, pyrazinamide). Nosocomial transmission of TB in HIV settings and its prevention Mycobacterium tuberculosis is transmitted via droplet nuclei through airborne inhalation. In open smear-positive patients, it has a basic reproductive number (the number of new secondary cases generated by an index patient), R 0, of 20-30, and about 10% will develop active disease. [3],[6],[33] Given this high reproductive number; the high background prevalence of TB and HIV infection; limited resources; poor state of health systems and facilities, which are already inundated, nosocomial transmissions of TB have occurred and can reach alarming levels in Africa. [28] For example, high prevalence of latent TB infection (57%) was found among health care workers in Kampala, Uganda, and delays in diagnosis and treatment of smear-positive TB heightened its incidence in hospital nurses working in medical wards in Blantyre, Malawi. [34],[35] But typically, nosocomial transmission is ignored or poorly recognized, although it should be addressed in these areas because of the potential serious consequences, particularly with drug-resistant TB and the specter of its association with HIV. Several outbreaks in the United States demonstrated the role that hospitals can play as focal points of MDR TB transmission, [36] a phenomenon also seen in Europe, South Africa and South America. [28],[29],[37] These outbreaks can be explosive and associated with high death rates because hospitalized patients are often HIV infected and/ or immunocompromised, as exemplified in KwaZulu-Natal. Recognizing nosocomial TB outbreaks can be daunting in Africa because of the high prevalence of background active and latent infections, thereby limiting use of skin test in assessments to determine new or old infections; difficulty in differentiating old infection, re-infection or relapse; poor laboratory diagnostic capacity; lack of relevant molecular epidemiologic tools; and the highly variable TB epidemiologic parameters, i.e., incubation period and serial interval, often used in classic infectious disease outbreak investigations. [3] However, clustering of cases in time, place and person is an important pointer to an outbreak. A hierarchy of control measures, including administrative (rapid diagnosis, quality smear microscopy, effective treatment, infectious patient movement restriction and isolation until smear negative), engineering and environmental controls (adequate ventilation, "negative pressure rooms," etc.), and personal protection measures has been recommended to reduce nosocomial TB risk. [38],[39] But the expenses for implementing the measures can be prohibitive for Africa. Therefore, WHO has proposed practical and low-cost modifications to reduce transmissions in resource-limited settings hinged upon early detection and effective treatment, less hospitalization and more ambulatory care, ventilation and avoidance of overcrowding, and standard infection control practices; [40] these should be widely implemented. Preventing active TB in HIV-infected patients Prevention of active TB is achieved with the use of isoniazid preventive therapy (IPT), which has been shown to confer protection in different settings and in both adults and children. In a meta-analysis [Figure - 1] comprising 11 clinical studies and trials with a total of 8,130 randomized participants, preventive therapy (any anti-TB drug) versus placebo was associated with a lower incidence of active tuberculosis (RR, 0.64; 95% CI, 0.51-0.81) [protection conferred was 36%]. [41] This benefit was more pronounced in individuals with a positive tuberculin skin test (RR, 0.38; 95% CI, 0.25-0.57) [protection of 62%] than in those who had a negative test (RR, 0.83; 95% CI, 0.58-1.18) [protection of 17%]. Efficacy was similar for all regimens (regardless of drug type, frequency or duration of treatment). However, compared to INH monotherapy, short-course multi-drug regimens were much more likely to require discontinuation of treatment due to adverse effects. Overall, there was no evidence that preventive therapy versus placebo reduced all-cause mortality (RR, 0.95; 95% CI, 0.85-1.06), although a favorable trend was found in people with a positive tuberculin test (RR, 0.80; 95% CI, 0.63-1.02). [41] Thus in adults, isoniazid (300 mg) daily for 6 months is favored after excluding active TB. Alternative regimens comprising rifampicin and/ or pyrazinamide for variable durations can be used as alternatives where factors such as adherence, adverse events, cost and drug resistance preclude the former. [41] It was shown in Cote d′Ivoire, West Africa, that a past history of TB at ART initiation was significantly associated with active TB while on ART, with incidence being 3.0 per 100 person-years in those with no history of prior TB compared to 11.3 per 100 person-years in those with a history of prior TB. [42],[43] Although such an association was not established among South African adults, [23] IPT was shown to reduce recurrent TB when used as secondary prevention, notably among miners. [44] Taken together, these findings [42],[43],[44] suggest that time-limited secondary prevention may be needed to prevent TB after initiation of ART in those with a prior history of TB. Although IPT has been increasingly promoted, concerns about the risk of development of isoniazid-resistant TB have been raised, especially in developing countries like Nigeria, where TB culture and drug susceptibility testing capacities are limited. In a meta-analysis to address the issue, all studies were combined from 1951, comprising 18,095 persons in the isoniazid group and 17,985 in the control group, and the summary relative risk for resistance was not statistically significant; 1.45 (95% confidence interval, 0.85-2.47). However, the point estimate and the upper boundary of the 95% CI are above unity, and findings do not also exclude an increased risk for isoniazid-resistant TB after IPT. [45] Therefore, continued surveillance for resistance is essential with IPT implementation. IPT has been well tolerated but a main concern is hepatotoxicity, which was reported in ~0.13%-0.83% of patients in Africa. [22],[44],[46],[47] Limited data suggest that the initial protective effect against tuberculosis with preventive therapy may decline over the short-to-medium term, although ART is as much a tool for HIV management as it is a prevention tool for TB [23] and can sustain the protection for the long term. Among patients in Rio de Janeiro [48] who received neither ART nor IPT, TB incidence was 4.01/100 person-years (py). Patients who received ART had an incidence of 1.90/100 py (95% CI, 1.66-2.17), and those treated with IPT had a rate of 1.27/100 py (95% CI, 0.41-2.95). The incidence among patients who received ART and IPT was 0.80/100 py (95% CI, 0.38-1.47). Multivariate cox-proportional hazards modeling revealed a 76% reduction in tuberculosis risk among patients receiving both ART and IPT (adjusted relative hazard, 0.24; P< .001) after adjusting for age, previous tuberculosis diagnosis, and CD4 cell counts at baseline. [48] The authors concluded that the use of both IPT and ART in HIV-infected patients is associated with significantly reduced tuberculosis incidence. In conjunction with expanded access to ART, the wider use of IPT in patients with HIV will improve tuberculosis control in high-burden areas. [48] In summary, the principles of TB prevention in HIV infection can be summarized with the three I′s: intensive TB case finding and surveillance, IPT and infection-control measures; to these can be added a fourth ′I,′ viz., instituting ART. Strengthening linkages between TB and HIV services There is need to strengthen linkages between TB and HIV services. Currently, only 10% of TB patients are tested for HIV in Nigeria; [1] all patients should be offered counseling and testing, preferably using the ′opt-out′ approach, where all are counseled and tested unless they indicate otherwise. Though "directly observed therapy short course" (DOTS) coverage has risen to 75% of the country population, provision of HIV services and referral linkages has remained sub-optimal. Elsewhere, it was shown that community DOTS centers can be used to provide step-down ART services for stable patients [49] and this should be the aim - to widen access to quality care. This facilitates integration of the services and wider access. Conversely, all HIV patients should also be screened for TB; the triad of fever, cough and weight loss for over 3 to 4 weeks should be elicited in all cases as it diagnoses TB in over 90% of cases. Access to improved qualitative smear microscopy and radiography should be made more widely available. Importantly, the phrase two diseases in one patient should be applied as there should be no parallel programs. That will lead to stronger collaborations, linkages and eventually integration of services. Conclusions HIV and TB continue to be linked in the pandemic in sub-Saharan Africa. Clinical presentation of TB is variable in HIV infection. In addition to the standard approaches to TB control, such as diagnosis and treatment of latent TB infection, recent studies have demonstrated that ART may also have a role in TB control. Despite major reductions with ART, however, the risk of TB remains high in Africa. As Nelson Mandela said, "We can not fight AIDS unless we do much more to fight TB as well"; thus, the standard principles of TB control will need to be followed and even expanded if we are to speed up the decline of TB. Also, much needs to be done to foster closer collaboration between, and integration of, TB clinics and ART services. Acknowledgments I would like to thank colleagues who have supported and facilitated my work over the years. They include colleagues at the Department of Medicine, AKTH, Kano; the CDC/ FMOH FELTP team, notably Drs Sani-Gwarzo, Obinna, Biya and Uwem; staff of the National TB and Leprosy Control Program; and fellow members of the National MDR TB Committee under the chairmanship of Dr Oni-Idigbe. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09032t2.jpg] [am09032f1.jpg] [am09032t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}