 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 8, No. 3, July-September, 2009, pp. 156-162 Original Article Blood pressure control and left ventricular hypertrophy in hypertensive Nigerians Salako BabatundeL, Ogah OkechukwuS, Adebiyi AdewoleA, Oladapo OlulolaO, Aje Akinyemi, Adebayo AdedejiK, Ojji DikeB, Ipadeola Arinola, Nwafor ChibuikeE Department of Medicine, Federal Medical Centre, PMB 3031 Sapon, Abeokuta, Ogun State Code Number: am09033 PMID: 19884691 Abstract Background : Hypertension is a disease characterized by end-organ complications, leading to high morbidity and mortality in many cases. People with untreated or uncontrolled hypertension often run the risk of developing complications directly associated with the disease. Left ventricular hypertrophy (LVH) has been shown to be a significant risk factor for adverse outcomes both in patients with hypertension and in the general population. We investigated the prevalence and pattern of LVH in a treated hypertensive population at the University College Hospital, Ibadan, Nigeria, using non-hypertensive subjects as control.Design and Setting : A prospective observational study performed at the University College Hospital, Ibadan, Nigeria. Methods : Patients had 6 visits, when at least one blood pressure measurement was recorded for each hypertensive subject and average calculated for systolic blood pressure (SBP) and diastolic blood pressure (DBP) separately. The values obtained were used for stratification of the subjects into controlled and uncontrolled hypertension. Subjects also had echocardiograms to determine their left ventricular mass. Results : LVH was found in 14 (18.2%) of the normotensive group, 40 (20.8%) of the uncontrolled hypertensive group and 14 (24.1%) of the controlled hypertensive group when left ventricular mass (LVM) was indexed to body surface area (BSA). When LVM was indexed to height, left ventricular hypertrophy was found in none of the subjects of the normotensive group, while it was found present in 43 (22.4%) and 14 (24.1%) subjects of the uncontrolled and controlled hypertensive groups, respectively. Significant difference in the prevalence of LVH was detected only when LVM was indexed to height alone. Conclusion : Clinic blood pressure is an ineffective way of assessing BP control. Thus in apparently controlled hypertensive subjects, based on office blood pressure, cardiac structural changes do remain despite antihypertensive therapy. This population is still at risk of cardiovascular events. Keywords: Blood pressure control, hypertension, left ventricular hypertrophy Résumé arrière-plan: l’hypertension est une maladie caractérisée par l’orgue de fi n complications menant à élevé de morbidité
et mortalité dans de nombreux cas. Personnes avec l’hypertension non traitée ou non contrôlée souvent risquent de
développer complications directement associées à la maladie. Laissé ventriculaire hypertrophie (LVH) a été démontré
un facteur de risque signifi catif pour les effets négatifs résultats tant chez les patients atteints de l’hypertension et
de la population générale. Nous avons a enquêté sur la prévalence et le modèle de LVH dans un traité hypertendues
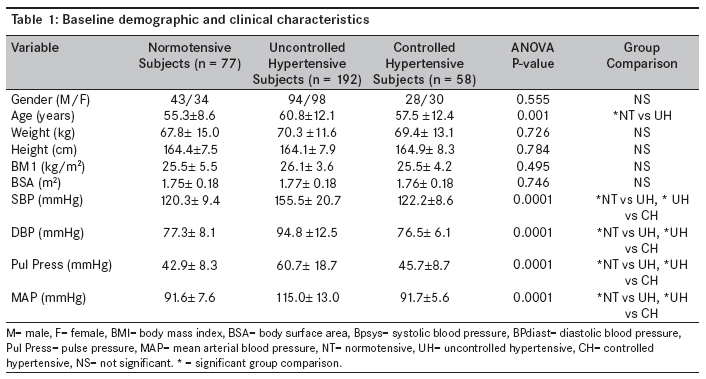
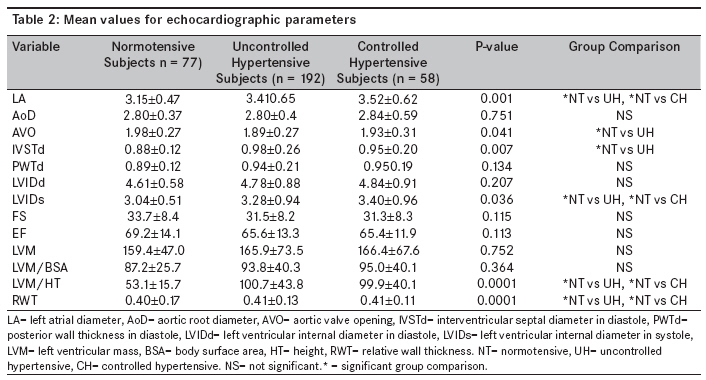
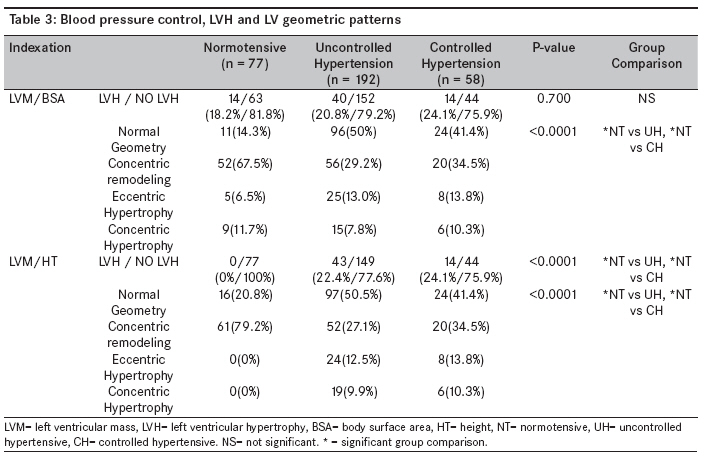
population au University College Hospital, à l’aide Ibadan, Nigeria non-hypertendues des sujets comme contrôle. Mots cles: contrôle de la pression sanguine, LVH, l’hypertension Introduction Hypertension is a disease characterized by end-organ complications, leading to high morbidity/ disability and mortality in many cases. [1] People with untreated and uncontrolled hypertension often run the risk of developing complications such as left ventricular hypertrophy (LVH), cardiomegaly, congestive cardiac failure, retinopathy, cerebrovascular disease and renal insufficiency. LVH alone has been identified to have adverse effect on survival of hypertensive patients. [2],[3] It has been shown to be an important predictor of cardiovascular morbidity and mortality in hypertensive patients and even in the general population. [4],[5] It is an adaptive response to increased left ventricular wall stress, which is reversible by treatment. Studies performed in Nigeria to evaluate blood pressure control in Nigerian hypertensive patients have shown that blood pressure control is poor, since only a few of them achieve a clinic blood pressure that can be described as optimal. [6],[7],[8] This study sets out to investigate the prevalence and pattern of LVH in both controlled and uncontrolled hypertensive population using apparently normal subjects as control in an attempt to observe the effects of treatment on LVH in the groups. Methods Normotensive healthy individuals and patients diagnosed with primary hypertension being followed- up in the medical clinic of the University College Hospital, Ibadan, were recruited into the study. Informed consent was obtained from the subjects, and their blood pressures were measured according to standard guidelines. [9] Recruitment into the study was spread over a period of 2 years. Blood pressure was measured in patients and controls after 5 minutes of rest and the average of two measurements taken each time. Six consecutive clinic BP values at an interval of 6 weeks were recorded for each hypertensive subject, and average was calculated for SBP and DBP separately. The average systolic and diastolic blood pressures were used in stratifying controlled and uncontrolled hypertensive subjects. A standard mercury sphygmomanometer (Accosson, London) was used, and systolic blood pressure (SBP) and diastolic blood pressure (DBP) were taken as Korotkoff sound phases I and V, respectively. A cuff of appropriate size was applied to the exposed right upper arm and was rapidly inflated to 30 mm Hg above the level at which the pulse disappeared and then deflated gradually. Blood pressure was considered to be well controlled if it was less than 140/90 mm Hg and uncontrolled if higher than 140/90 mm Hg. [10],[11] Weight was measured to the nearest 0.5 kg with subjects in light clothing and without shoes on a beam balance scale calibrated with standard weights. Height was measured to the nearest centimeter using anthropometric plane with subjects not putting on shoes or headgear. Body-mass index (BMI) was calculated using the formula BMI = Weight (kg)/ [Height (m)]2 , and body surface area (BSA) was measured by the formula of Dubois. Subjects with heart failure, cerebrovascular disease, ischemic heart disease, diabetes mellitus and renal failure were excluded from the study. Echocardiography Two-dimensional guided M-mode echocardiography with the use of commercially available echo-machine (ALOKA SSD-1, 700) and a 3.5-MHz linear array transducer was performed on each subject in the left lateral decubitus position. All measurements were made according to the leading edge-to-leading edge criteria of the American Society of Echocardiography. [12] Left Ventricular (LV) measurement was obtained at end diastole and end systole. The LV measurements taken include interventricular septal thickness at end-diastole (IVSTd), the posterior wall thickness at end-diastole (PWTd) and the LV internal dimensions at end-systole (LVIDs) and end-diastole (LVIDd). Measurements were taken in 3 cardiac cycles, and average of the 3 values was calculated. Two experienced echocardiographers performed all the echocardiographic examinations. In our laboratory, the intra-observer concordance correlation coefficient ranged from 0.76 to 0.98, while that of the inter-observer concordance ranged from 0.82 to 0.96. [13] Calculation of derived variables and LV hypertrophy Left ventricular mass (LVM) was calculated using the following formula, which has been shown to yield values closely related to necropsy LV weight and also has good inter-study reproducibility (r= 0.90) [14] : . LVM = LVM = 1.04 Χ [(LVID + IVS + LVPW) 3- (LVID) 3 )-13.6] Relative wall thickness was calculated as 2-x posterior wall thickness/LV internal dimension in diastole. [15] LV hypertrophy was considered present when LVM indexed to body surface area exceeded 116 g/m 2 in men and 104 g/m 2 in women, [16] or LVM indexed to height exceeded 126 g/m in men and 105 g/m in women. [17] Increased relative wall thickness was present when RWT was greater than 0.43, which represents the 97.5 th percentile in normal subjects. [18] LV geometry was defined using LV mass index and relative wall thickness. Normal geometry was present when indexed LVM (LVMI) and RWT were normal, whereas normal LVMI and increased RWT identified concentric remodeling. Increased LVMI but normal RWT identified eccentric LV hypertrophy, and increases of both variables identified concentric hypertrophy. [19] LV systolic performance (fractional shortening and ejection fraction) was calculated using the Teichholz′s formula. [20] Data analysis SPSS software version 12.0 (SPSS, Inc., Chicago, Illinois) was used for statistical analysis. Continuous variables were expressed as mean ± SD (standard deviation); and categorical variables, as percentages. Differences in categorical variables were assessed by chi-square analysis. Multiple comparisons were performed by analysis of variance (ANOVA). The Bonferroni post hoc test was used for comparison between groups. A 2-tailed P value < .05 was considered to be significant. Results Patient characteristics [Table - 1] shows the baseline demographic and clinical characteristics of the subjects. Two hundred fifty (250) hypertensive subjects and 77 normotensive subjects (NT) were recruited into the study. Of the 250 hypertensive subjects, 122 (48.8%) were men and 128 (51.2%) were women . As many as 192 (76.8%) hypertensive subjects had uncontrolled blood pressure (UH), while 58 (23.2%) had controlled blood pressure (CH). Of the 77 normotensive subjects, 43 were males while 34 were females. Subjects with uncontrolled blood pressure were significantly older than the normotensive subjects (60.8 ± 12.1 vs. 55.3 ±, P = 0.001). Otherwise, weight, height, BMI and BSA were similar in the 3 groups. As expected, blood pressure measurements were significantly higher in the group with uncontrolled BP when compared with the controlled BP and normotensive subjects. Echocardiographic measurements [Table - 2] depicts the mean values of echocardiographic parameters of the 3 groups. Left atrial diameter was significantly higher in the hypertensive subjects compared with the normotensive subjects (UH, 3.41 ± 0.65 vs. CH, 3.57 ± 0.62; as against NT, 3.15 ± 0.47, P= 0.001). The aortic valve opening (AVO) and the interventricular septal wall thickness in diastole (IVSTd) were significantly higher in the subjects with uncontrolled BP when compared with normal subjects but not when compared with the subjects of controlled BP group. The LVIDs and the LVM/BSA were also significantly larger in the hypertensive subjects (UH and CH) when compared with normotensive subjects (NT). Relative wall thickness was significantly higher in normal subjects (NT, 0.57 ± 0.17; UH, 0.41 ± 0.13; CH, 0.41 ± 0.11, P= 0.0001). The LV posterior wall thickness, LV internal dimensions in diastole, LVM and LVM/BSA were similar in the 3 groups. Prevalence of LVH and LV geometric patterns [Table - 3] shows the prevalence of the LVH and the LV geometric patterns in the 3 groups. When LVM was indexed to body surface area, LVH was found in 14 (18.2%) subjects of the NT group, 40 (20.8%) of the UH group and in 14 (24.1%) of the CH group. Forty-three (22.4%), 14 (24.1%) and none of the subjects in the UH, CH and NT groups, respectively, had LVH when LVM was indexed to height. This was statistically significant (P= 0.0001). With respect to LV geometry, 52 (67.5%), 56 (29.2%) and 20 (34.5%) subjects of the NT, UH and CH groups, respectively, had concentric remodeling when LVM was indexed to BSA. The corresponding numbers when LVM was indexed to height were 61 (79.2%), 52 (27.1%) and 20 (34.5%) for NT, UH and CH groups, respectively. Eccentric hypertrophy was found in 5 (6.5%), 25 (13.0%) and 8 (13.8%) subjects of the NT, UH and CH groups, respectively. The corresponding numbers when LVM was indexed to height were 0 (0.0%), 24 (12.5%) and 8 (13.8%) for NT, UH and CH groups, respectively. There were 9 subjects in the NT group with concentric LVH; 15, in the UH group; and 6, in the CH group when LVM was indexed to body surface area. Nine (11.7%), 15 (7.8%) and 6 (10.3%) subjects in the NT, UH and CH groups, respectively, had concentric LVH when LVM was indexed to height. Discussion Left ventricular hypertrophy is a common adaptive process that is induced by certain physiological and pathological stimuli that are naturally put in place to normalize the increase in left ventricular wall stress caused by hypertension. The findings from this study are that (1) absolute LVM, indexed LVM and LV wall thickness appear similar in controlled and uncontrolled subjects and even higher in the group with controlled BP and that (2) left ventricular internal dimensions appear similar in the controlled and uncontrolled BP groups and, in some cases, higher in the controlled BP group. Also, the findings may not be due to age difference since the mean age of the subjects was higher in the uncontrolled BP group. More so, the findings remained same after adjusting for age. Thus in hypertensive subjects, changes in left ventricular geometry can be found both in controlled and uncontrolled hypertension. These changes may not be completely reversed by blood pressure control. Since LVH is associated with adverse cardiovascular events, hypertensive subjects with apparent BP control may still be at risk of events. Our finding of persistence of LVH in subsets of treated hypertensive subjects is similar to the findings of some workers, especially those who based their blood pressure control on clinic or office blood pressure alone. [21] Gamble and co-workers studied the prevalence of LVH and carotid plaques in 500 hypertensive subjects and in 506 apparently normal subjects. They found no difference between the frequency of LVH in controlled and uncontrolled hypertensive subjects. On the other hand, those who used ambulatory blood pressure monitoring (ABPM) in stratifying subjects have observed more severe LV structural changes in the group with uncontrolled BP. [22],[23] Evidences abound that ABPM is a better method of monitoring blood pressure control than office BP. Many studies that used ABPM as an index of blood pressure control have demonstrated that LVM is more closely associated with ambulatory BP than office BP. [24],[25],[26],[27],[28] In this study, we observed that that the prevalence of LVH in hypertensive subjects was similar to the values observed in normotensive subjects when LVM was indexed to BSA but not so when it was normalized by height. This confirms the limitation of indexing LVM using BSA. Workers have shown that indexation to height is better than that to BSA, as shown by our finding, especially in obese subjects [17] . Another possibility is the concept of "apparent normotension," which may be present in some subjects of the control group. This study has shown that in patients with primary hypertension on treatment, prevalence of LVH ranges from 20.8%- to 24.5% in uncontrolled hypertensive subjects and from 24.1%- to 27.6% in controlled hypertensive subjects, using three different calculations. In a recent study in controlled hypertensive subjects, prevalence of 6% was found. The present study recorded a higher figure when compared to this, whereas our figure is comparable to 19% and 35% found in another study among controlled and uncontrolled hypertensive subjects, respectively. In this cohort of patients, LVH prevalence was about the same in both controlled and uncontrolled hypertensive subjects. However, the prevalence of LVH was surprisingly slightly higher among the controlled hypertensive subjects when compared with subjects of the uncontrolled group, although this did not reach statistical significance. We do not have adequate information about the duration of treatment in many of the subjects; therefore, the time factor and perhaps the small number of controlled hypertensive subjects may explain the above picture. The pre-treatment echocardiographic parameters of the subjects were also not available for comparison, and this made it difficult to assess the prevalence of LVH before the beginning of therapy. In another study relating hypertension, antihypertensive treatment and LVH together, left ventricular hypertrophy was twice as prevalent in hypertensive subjects compared to normotensive controls but was not different between treated and untreated hypertensive subjects, which is in agreement with our findings. Our finding of higher frequency of eccentric hypertrophy when compared with concentric LVH in this study is similar to the findings of other workers. [23] Overall, eccentric cardiac hypertrophy was mostly found with a ratio of about 1.2:1. This is in agreement with a previous observation. [16] The clinical and prognostic significance of eccentric hypertrophy is less adverse compared to that of concentric hypertrophy, and this has been explained to be a protective effect of chronic hypertension treatment. [4] The present study agrees in certain areas with others that have documented that cardiac structural damage can be frequently found in the presence or absence of antihypertensive treatment. This assertion probably indicates that even in the face of effective treatment, total or complete reversal of cardiac structural damage does not occur. However, the findings in our study that showed that prevalence of LVH in normotensive subjects was not different from that in the subjects of the hypertensive group call for reappraisal of the three calculations used to determine LVH in this study since one of the methods did not detect LVH in normal people but the other two did. There is also a need to determine normal values for echocardiographic parameters for our environment since the values used in this study were based on studies in Caucasians. Limitations The limitations of the study are as follows: 1. There was inability on our part to measure BP controls using ABPM; 2. since our study was cross-sectional, we could not take into account the pre-treatment blood pressure and the pre-treatment LVM; 3. we could not also conduct renal evaluation in our subjects, which is a very strong determinant of LVM; and 4. finally the duration of treatment and the classes of anti-hypertensive therapy were not taken into consideration in this study. Conclusion The conclusion that can be drawn from this study is that office blood pressure is an ineffective way of measuring BP control. Also, because this study was an observational (cross-sectional) one, it was difficult to take into consideration confounding variables such as pre-treatment blood pressure and LVM. Nevertheless, our study has shown that in apparently controlled hypertensive subjects, using office BP as a criterion, cardiac structural changes do remain despite antihypertensive therapy and that this population is still at risk of cardiovascular events. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09033t2.jpg] [am09033t1.jpg] [am09033t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}