 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 8, No. 3, July-September, 2009, pp. 163-167 Original Article Pediatric day case surgery: Experience from a tertiary health institution in Nigeria Abdur-Rahman LO, Kolawole IK, Adeniran JO, Nasir AA, Taiwo JO, Odi T Department of Surgery, Paediatric Surgery Unit, Ilorin Code Number: am09034 PMID: 19884692 Abstract Background : The general observation that children achieve better convalescence in the home environment supports the need for adoption of day case surgery, which is gaining considerable acceptance in developing countries. Pediatric surgical service is in great demand in developing countries, and in-patient beds and surgical supplies are insufficient. Method : A prospective collection of data on all pediatric day surgeries (PDSs) by the pediatric surgical unit University of Ilorin Teaching Hospital (UITH, Ilorin, was done. Parents had pre-operative outpatient briefing and postoperative interviews on the second and ninth days for consultation regarding post-operative complications and events at home. Study period was between April 2005 and September 2007 (2½ years). Keywords: Day case surgery, developing country, pediatric Résumé
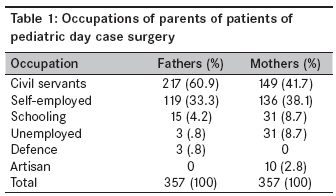
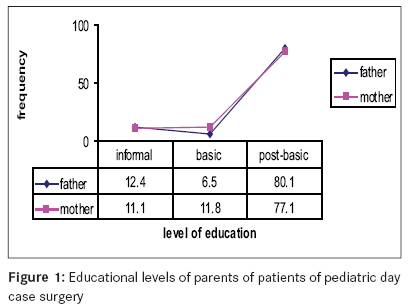
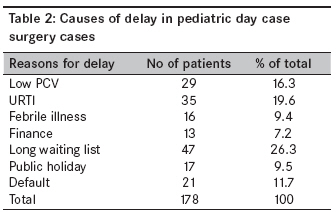
Arrière-plan: Le observation générale que les enfants atteindre convalescence mieux à la maison environnement Mots cles: jour cas de Chirurgie pédiatrique, les pays en développement Introduction Day case surgery (DCS) is a modern, effective and economical way to treat patients while maintaining the same level of quality of patient care. DCS has been reported to be safe and effective for a large proportion of infants and children requiring operation in many pediatric hospitals. [1],[2],[3] It is gaining considerable acceptance in developing countries because it is cost effective [4] and maintains confidentiality due to decrease in the number of visits to the sick in the hospital by neighbors and relations for social and cultural reasons. Many parents have expressed satisfaction with this approach. [5],[6] Ameh [7] and Bickler [8] have advocated increase in the number of pediatric surgical specialists in developing countries to take care of the rising number of pediatric surgical cases in a setting of insufficient surgical supplies. DCS has assisted in reducing waiting time and hospital stay, usually caused by inefficient utilization of operating theaters, which makes urgent and emergency cases to fill the available beds and operation lists. The general observation has been that children achieve better convalescence and outcome in the home environment because of lack of separation trauma and sudden change of environment. 9 Even where DCS is practiced, avoiding unpleasant experiences like the ones children have at health centers and introduction of play area could perhaps help children cope with a short-duration hospital experience. [9],[10] The practice of day surgery, especially among children, in a new unit needs the adaptation of set guidelines [11] to meet the peculiarity of the environment. This study was carried out to determine the pattern of pediatric day surgery and factors that affect the practice in our environment. Methods A prospective study of pediatric day surgery was carried out over a period of 2½ years (April 2005 to September 2007). Prior to this period, minor and intermediate elective surgeries in children usually involved short stays or full in-patient admission. Preoperative evaluation and selection of patients were based on clinical and laboratory parameters, and the patients who were clinically fit and had packed cell volume (PCV) of ≥28% and hemoglobin genotype AA, AC and AS were included. Those with low PCV (≤27%), genotype SS and compromising congenital anomalies; and preterm neonates were excluded. Anesthesiologists conducted pre-operation evaluation in the ward on the morning of surgery because there is no facility of a pre-anesthesia evaluation clinic (PEC). Parents had pre-operation outpatient briefing about the diagnosis, surgical treatment and offer of a discharge home on the day of surgery, after which signed consent was obtained. They were also given document indicating time to report to the ward and commencement of the period of "nil by mouth," which was 4 hours for infants on clear fluids and the entire night before meals for older children. Patients were also observed in the recovery room and reviewed in the ward prior to discharge by the unit doctors who instructed and reminded them about postoperative care and what to expect at home. Post-operative interviews on the second and ninth days for consultation regarding postoperative complications and events at home were done at the outpatient clinic. General and local anesthesia, including intraoperative analgesia, were used in the patients as deemed necessary. Postoperative analgesia was mainly pentazocine 1 mg/kg intramuscular administered in the recovering room and oral paracetamol 15-20 mg/kg every 4-6 hours. Results A total of 660 elective operations were done, of which 449 (68.03%) cases were day cases. Eighty cases of circumcision and 12 cases of ankyloglossia release were excluded from the study. The remaining 357 children comprised 334 (93.6%) males and 23 (6.4%) females, with age ranging from 20 days to 15 years and a mean of 37.6 months ± 34.4 months of standard deviation (SD). There were 254 (71.2%) cases of patent processus vaginalis with hernia and hydrocele; 46 (12.9%), superficial lumps and masses; 31 (8.9%), undescended testis; 17 (4.8%), umbilical hernia; and 9 (2.5%), thyroglossal duct cyst. Sixty-one (17.1%) patients had had previous operation when they were admitted for herniotomy (54, 88.5%) and lump excision (7, 11.5%). They all expressed excellent and satisfactory experience of this day case approach compared to the in-patient service they had experienced, particularly with regard to the disruption of their routine daily schedules and stress on the family and social system requiring relations and neighbors to be informed about the surgery and the children′s condition. Almost all parents (98.9%) of the patients resided within 20 km radius of the hospital. (Some of the parents residing outside the city came to stay with relatives in town.) About 91.5% of them could reach the hospital within 1 hour by using their private cars (39.3%), motorbike (1.4%), public/ neighbors′ vehicles (57.9%) or by walking to the hospital (1.4%). The distance from the hospital did not affect the practice of day case practice in this study. Regarding parents′/ caregivers′ occupation, 60.9% of fathers and 41.7% of mothers were civil servants [Table - 1]. With regard to education of parents, 80.1% of fathers and 77.1% of mothers had post-basic education [Figure - 1]. The mean interval between the first outpatient visit and surgery was about 4.53 weeks, with a range of 2-9 weeks. Reasons for delay are shown in [Table - 2]. The mean duration of surgery was 24 minutes ± SD of 13.8 minutes. Postoperative hemorrhage was witnessed in 7 (1.6%) patients but was controlled before discharge. Fourteen (3.2%) children were irritable at home because of pain, while the remaining 95.2% had no complications. Eleven (78.6%) of the mothers of patients who had postoperative pain at home had had post-basic education (P = 0.799). Four (1.1%) parents preferred admission of their wards because of the fear of the unknown; and of these, 3 would not recommend day case surgery to others. The estimated average cost per patient was eleven thousand two hundred naira only [(N 11,200) (USD99)], which covered operation packs, anesthesia and consumable items. Discussion Pediatric day surgery (PDS) has a long history [12] and has become widely accepted and practiced in the developed and developing countries, using the Royal College of Surgeons guidelines. [13] It is an established practice in Ile-ife and Lagos. [2],[14],[15] This was not the case in our unit prior to this study, when most operations except circumcision were done requiring short hospital stay (2-5 days) or full in-patient admission. This was probably because pediatric surgical unit was new, with a trained consultant pediatric surgeon, inadequate in-house complementary staff -and no dedicated day surgery unit in the hospital. Also the community being served lacked the necessary services with regard to communication, home doctoring and nursing. On the basis of this study, it can be said that PDSs constituted 68% of all elective procedures done by the unit during the study period, and these are still on the increase. This is comparable with what is obtainable in the USA [16] and locally in the sub-region [2] but certainly above figures for UK. [13],[17] The elective operation time allotted to pediatric surgery unit is less than 6 hours per week in a unit with two consultant pediatric surgeons, currently. The selection criteria adopted ensured that medically fit children were included in the study, which is a novel practice in pediatric surgical service at our hospital. Modified studies on other diagnoses or clinical conditions and environmental parameters may be needed in future. Using Brenan′s selection criteria, [18] term neonates were included in the study, and the coauthor′s skill in pediatric anesthesia also facilitated the conduct of the study. Cases of umbilical hernia repair and thyroglossal duct cyst excision (Sistrunk operation) were included in the last 9 months of the study, when confidence was gained in the practice of PDS in our unit; and evidently, it was found to be generally safe, a fact which is supported by the works of Yawe, [3] Agbakwuru, [4] Jiburum [19] from the sub-region, but care must be taken to avoid excessive dissection and mobilization of the gut or trachea, which can precipitate an ileus and laryngeal spasm or tracheomalacia. Parents expressed satisfaction because of the short stay in hospital environment; minimal disruption of routine family, official and social functions; and, of course, their wards′ comfort offered by the PDS setting. The satisfaction with day case surgery expressed by the parents of children who have had previous in-patient surgical service was encouraging. PDS as practiced in Europe and North America requires, in many cases, follow-up by their family physicians or general practitioners in the community or through the use of telephones. [20] The area of domicile of majority of our patients showed that there was easy access to the health facility in case of any complaint, and early visitation for outpatient follow-up allowed early assessment and attention to complaints. Not many patients had problems, and it may not be necessary to have day cases reviewed by hospital visit early after surgery. Parents and guardians in this study had adequate education to comply with instructions for the preparation of their wards for surgery and postoperative care. The educational level of these parents also assisted them in understanding the explanation about the diagnosis and acceptance of PDS, though initially with some difficulty, as many parents preferred medications to surgery on their wards; worse still, on a day-care basis. Out of the 14 patients who had postoperative pain, 11 of the mothers had post-basic education; however, this did not have statistical significance in relation to the outcome. This study also showed that there was minimal disruption of parents′ occupational activities because they were able to attend their duties on the days outside the operation day; there was also little change in the children′s environment because they were nursed at home. The delays experienced can be curtailed if a dedicated day case theater can be allocated for the Paediatric surgery unit (PSU) to reduce competition of day cases with the cases in the in-patient elective list. The newly introduced National Health Insurance Scheme (NHIS), the current beneficiaries of which are civil servants, would also assist in the provision of prompt funds for the care of these patients. The cost benefit is because patients do not pay admission fee; no cost is incurred for transportation by family members to and from hospital during visits; there is no cost of inpatient catering services, telephone calls; and expenses by visitors are eliminated. The risk of contracting nosocomial infections is also eliminated. Proper patient selection has been shown to eliminate unplanned admission, [17],[21] and our study has confirmed this since we did not record any mortality and no patient had an unplanned admission. The few cases of morbidities were due to poor pain control, which may be due to noncompliance with the 4-6 hourly prescribed dosing per kg body weight of acetaminophen by the parents who were used to three times daily dosage. In conclusion, pediatric day surgery is feasible for well-selected and monitored cases in our environment, and it has huge benefits. Children of all age groups, including neonates, who have well-informed parents are suitable for pediatric day case surgery. There is a need for a dedicated day case center in our hospital to reduce waiting list. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09034t1.jpg] [am09034f1.jpg] [am09034t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}