 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
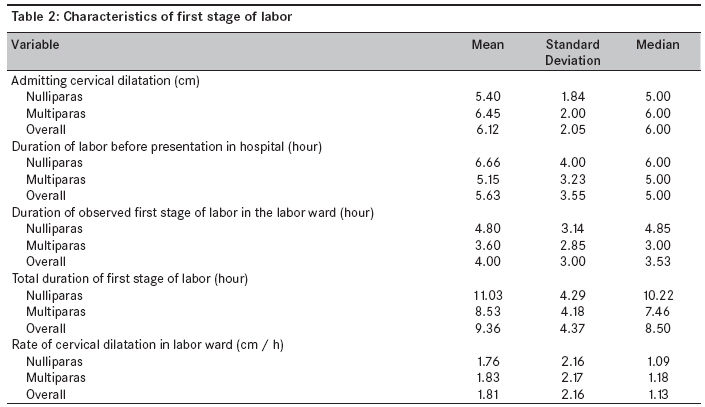
Annals of African Medicine, Vol. 8, No. 3, July-September, 2009, pp. 181-184 Short Report Pattern of cervical dilatation among parturients in Ilorin, Nigeria Ijaiya Munir'deenA, Aboyeji AbiodunP, Fakeye OlurotimiO, Balogun OlayinkaR, Nwachukwu DuumC, Abiodun MosesO Department of Obstetrics and Gynaecology, University of Ilorin Teaching Hospital, Maternity Hospital Wing, Ilorin Code Number: am09038 PMID: 19884696 Abstract Objective : To evaluate the pattern of cervical dilatation in live singleton pregnancies with spontaneous onset of labor and to compare any differences among nulliparas (P ara 0) and multiparas (Para ≥1). Keywords: Cervical Dilatation, First Stage, Spontaneous Labor Résumé Objectif: pour évaluer la motif de dilatation du col utérin dans les grossesses singleton live avec spontanée apparition
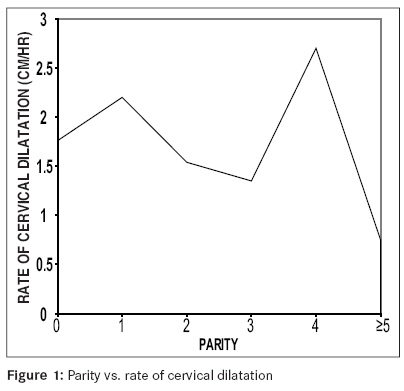
du travail et de comparer les différences entre les nulliparas (para 0) et multiparas (para ≥1). Mots cles: Irritable Syndrome de la communauté, africains Introduction Labor is the physiologic process by which regular painful uterine contractions result in progressive effacement, dilatation of the cervix and ultimately leads to the delivery of the fetus through the birth canal. Cervical dilatation is one of the major determinants of progress of labor and is dependent on the forces of labor. [1] Poor understanding and management of labor may lead to prolonged/ obstructed labor, which is one of the leading causes of maternal mortality in Nigeria. [2],[3] Prolonged/ obstructed labor accounts for one- tenth of maternal deaths in developing countries, where 99% of the maternal deaths worldwide occur. [4],[5] Hendricks, Friedman, Philpott and other researchers did an extensive work on management of labor, namely, gravicostatistical analysis of labor, which serves as a managerial tool. [6],[7] The aim of this study was to examine the pattern of cervical dilatation among parturients in Ilorin, Nigeria. The specific objectives of the study included the following: to determine and compare the admitting cervical dilation, duration of labor from onset of labor to full cervical dilatation, and rate of cervical dilatation among nulliparas and multiparas. To the best of the authors′ knowledge, having perused through available literature and internet, this appears to be the first original article on this topic from the West Africa subregion. Methods The study was conducted at the maternity hospital wing of the University of Ilorin Teaching Hospital, Ilorin, Nigeria, from May 2004 to June 2004. The inclusion criteria included labor with spontaneous onset, gestational age equal to or greater than 37 weeks, live singleton pregnancy, and vertex delivery. Patients that met these criteria and had augmentation of labor or rehydration were also included. A total of 238 consecutive labor cases that satisfied the inclusion criteria were prospectively studied. Patients that had pre-labor rupture of membrane, instrumental vaginal delivery or abdominal delivery and referred patients were excluded. All information obtained was recorded on a data-collected form designed for the study. Parity, age, gestational age and duration of labor as at presentation were recorded. Other information included cervical dilatation at presentation and duration of first stage of labor from time of arrival to full cervical dilatation. The hospital operates as both secondary and tertiary health care facility. Parturient is usually first attended to by an intern and then reviewed by registrar, senior registrar and consultant. Events of labor are documented in the partograph. Vaginal examination is performed at admission and subsequently every 3 to 4 hours and more frequently if need arises. For data analysis, Pearson correlation and t test were used (SPSS 11.0 software). Results A total of 238 cases were analyzed. The patients′ age ranged from 16 to 38 years with a mean of 28.34 years. Looking at the parities individually, nulliparas had the highest frequency (31.5%), while the mean parity and median parity were 1.38 and 1, respectively. Mean gestational age was 39.59 weeks (range, 37.00-45.71 weeks), as seen in [Table - 1]. Only 53 (22.3%) patients had augmentation of labor. The characteristics of first stage of labor are summarized in [Table - 2]. Mean cervical dilatation on presentation in labor ward and duration of labor before presentation in labor ward among nulliparas (Para 0) were 5.40 cm and 6.66 hours; and among multiparas (Para ≥1), 6.45 cm and 5.15 hours, respectively, the overall mean being 6.12 cm and 5.63 hours, respectively. The differences between nulliparas and multiparas were statistically significant (t test P< 0.05). Also, a significant positive correlation at 0.01 level existed between parity and cervical dilatation on presentation (.189), and a negative correlation existed between parity and duration of labor before presentation (.200). The average time spent to achieve full cervical dilatation from time of arrival in labor ward was longer in nulliparas (4.80 hours) than in multiparas (3.60 hours) (t test not significant; P> 0.05). Overall average total length of first stage of labor, i.e., from onset of labor to full cervical dilatation, in all the parturients was 9.36 hours; being 11.03 and 8.53 hours for nulliparas and multiparas, respectively (difference was significant; t test P< 0.05). There was significant negative correlation between parity and total length of first stage of labor (.238). Mean cervical dilatation rate, from the time of arrival in labor ward to full cervical dilatation, was more in multiparas (1.83 cm/h) than in nulliparas (1.76 cm/h), but the difference was not significant (t test P> 0.05). Para 4 and Para 1 had the highest rate of cervical dilatation, viz., 2.66 cm/h and 2.15 cm/h, respectively, which is illustrated by line graph in [Figure - 1]. There was no significant correlation between rate of cervical dilatation and the following variables: maternal age (.002), gestational age (.094) and birth weight (.042). Discussion Length of labor is important to the fetus, mother and obstetrician. Unduly prolonged labor is an unpleasant experience, which no pregnant woman ever wishes to undergo. It sometimes leads to personality problems like phobia for labor. Prolonged/ obstructed labor remains a major contributor to maternal and perinatal morbidity and mortality in developing countries. [3],[8],[9] In this study, the time patients started perceiving regular uterine contractions was taken as the onset of labor, although it is subjective. The mean admission cervical dilatation was more in multiparas than nulliparas (6.45 vs. 5.40 cm; P significant); this is in keeping with the finding of Chapel Hill, North Carolina, USA. [6] This result could simply be interpreted that multiparas parturient sought medical attention later than their nulliparous counterparts. But surprisingly, the interval between the onset of labor and presentation at the hospital was shorter in multiparas than nulliparas (5.63 vs. 6.66 hours; P significant). This could probably be explained by the postulation of Hendricks et al. that cervix starts dilating before onset of labor and mean cervical dilatation at the onset of labor is more in multiparas than in nulliparas. [6] Furthermore, cervical changes as observed by attending doctors were analyzed, which is a more accurate and objective assessment of cervical dilatation in first stage of labor. The mean total duration of first stage of labor was longer in nulliparas than in multiparas (11.02 vs. 8.53 hours; P significant). However, the differences in mean length of labor as observed in labor ward, i.e., from time of arrival to full cervical dilatation (Para 0 was 4.80 hours as against 3.60 hours for Para ≥1), and mean rate of cervical dilatation between the two groups (Para 0 was 1.76 cm/h, while Para ≥1 was 1.83 cm/h) were not statistically significant. This is consistent with the observation by Hendrick et al., that when labor is progressing at what appears to be an optimal rate, the mean rate of cervical dilatation for nulliparas is just as fast as that for multiparas. [6] Both mean rates of cervical dilatation were normal and above the World Health Organization-specified and Philpott′s lower limit of 1 cm/h in the active phase of labor, which represents the mean rate of progress of the slowest 10% of patients in the study population. [10],[11],[12] However, maternal age, gestational age and fetal size did not significantly affect the rate of cervical dilatation in this series. In conclusion, this study revealed that the higher the parity the shorter the length of first stage of labor; however, significant difference existed only in the first half of first stage of labor between nulliparas and multiparas. The mean rate of cervical dilatation was also greater than 1 cm/h in active phase of labor. Acknowledgment We are grateful to the other consultant staff of the department for allowing us to conduct this study on their patients and the resident doctors that participated in filling the data forms. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09038t1.jpg] [am09038t2.jpg] [am09038f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}