 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 8, No. 3, July-September, 2009, pp. 185-188 Case Report Portal biliopathy in a 13-year-old Asian girl: A case report and review of literature Ajayi AO, Chandrasekar T.S.C, Hammed AH Gastroenterology Unit, Department of Medicine, Federal Medical Centre, Ido-Ekiti Code Number: am09039 PMID: 19884697 Abstract Portal biliopathy (PB) is a term used to describe biliary ductal and gallbladder wall abnormalities seen in patients with portal hypertension. The pathogenesis of PB is not well known. It has been postulated that external pressure of portal cavernoma and/ or ischemia may play a role. We report a case of a patient with PB presenting with obstructive jaundice that involved endoscopic sphincterotomy and stenting.Keywords: Jaundice, portal biliopathy, sphincterotomy, stent Résumé Portail biliopathy (PB) est une terminologie utilisée pour décrire les biliaire ductal et anomalies de mur de la vésicule biliaire vu chez les patients atteints de portail hypertension. la pathogenèse de PB n’est pas bien connue. Il a été posé que pression extérieure du portail cavernoma et/ou ischaemie peut jouer un rôle. nous avons signalé un patient avec PB présentant jaunisse obstructive qui avait sphincterotomy endoscopique et stenting. Mots cles: portail biliopathy, la jaunisse, sphincterotomy, Stent Introduction Portal biliopathy (PB) is a term used to describe biliary ductal and gallbladder wall abnormalities seen in patients with portal hypertension. [1],[2],[3] These changes are predominantly seen in patients with extra-hepatic portal vein obstruction (EHPVO) and include abnormalities (stricture and dilatation) of both extra- and intra-hepatic bile ducts and varices of the gallbladder. [4] Occasionally, these changes become significant to give rise to overt obstructive jaundice and possibly contribute to the development of choledocholothiasis. [5] Biliary stasis is produced by pressure effects from engorged paracholedochal and epicholedochal collaterals on the bile ducts. Such collaterals are present in all patients with EHPVO, and the frequency and severity of PB are greater in these patients than in patients with liver disease. [5],[6] EHPVO is a common cause of portal hypertension in developing countries and constitutes up to 40% of all patients with portal hypertension. [7],[8] EHPVO is a common cause of major upper gastrointestinal bleeding among children. [8],[9],[10] Portal vein obstruction in EHPVO is transformed into a cavernoma, which is a bunch of multiple collateral veins around the obstructed portion of portal vein. [11] The reasons for EHPVO are obscure in approximately half of the patients. Omphalitis and intra-abdominal sepsis are the common causes in neonates and children. Adults develop EHPVO due to increased blood coagulability; local inflammation; intra-abdominal sepsis; myeloproliferative disorders; or underlying cirrhosis or tumors in the liver, bile ducts and pancreas. [12],[13],[14],[15] The frequency of PB in patients with EHPVO (81-100%) [6] is much greater than among patients with cirrhosis of the liver (0-33%) [4] or idiopathic portal hypertension (9-40%). [4] This is most probably related to longstanding portal hypertension that results in the development of large collaterals in the biliary region with the formation of typical portal cavernoma. We report a case of a patient with PB presenting with obstructive jaundice that involved endoscopic sphincterotomy and stenting. Case Report A 13-year-old girl presented at MedIndia Hospital, India, with a 4-month history of jaundice and yellow urine; and fever of 4 days′ duration. There was no history of pale stool or body itching. Jaundice had been deepening since onset, and fever was low grade without chill or rigors. She had noticed abdominal distension and heaviness in the left hypochondrium. There was no hematemesis or melena; however, she had developed hematemesis and melena in 1999 and was admitted to the Medical College Hospital, where she was investigated and found to have EHPVO. Sclerotherapy was done and the patient was kept on propanolol. Between 1999 and March 2007, she had had 15 sessions of sclerotherapy. Her delivery was reported to be normal, with no umbilical sepsis or jaundice in the neonatal period. Her developmental history was also reported to be normal until age 7 years, when she started having growth retardation. There was no family history of such a problem. On examination, we found a small-for-age girl, deeply jaundiced, febrile (T= 37.8°C), pale, with no pedal edema and no finger-clubbing of the toes or fingers. Abdominal examination revealed a slightly distended abdomen with right hypochondrium fullness, as well as moderate tenderness over the right hypochondrium. Liver was palpable 4 cm below the right costal margin and was 14 cm in total span; also, spleen was palpably enlarged by 4 cm below the left costal margin. Ascites was demonstrable by shifting dullness, and both kidneys were not palpable. Results of cardiovascular and chest examinations were essentially normal. A diagnosis of EHPVO with obstructive jaundice was made. She was admitted for further investigations. Meanwhile, she was kept on intravenous antibiotics. Following are the investigation results:
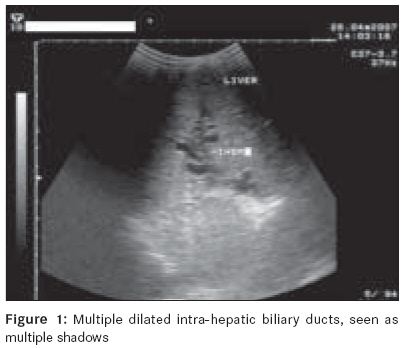
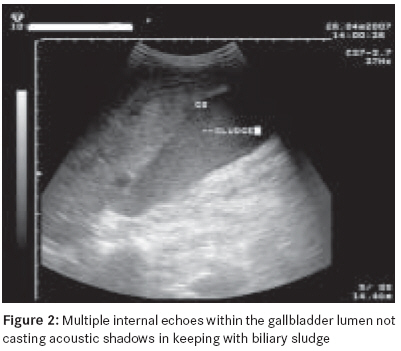
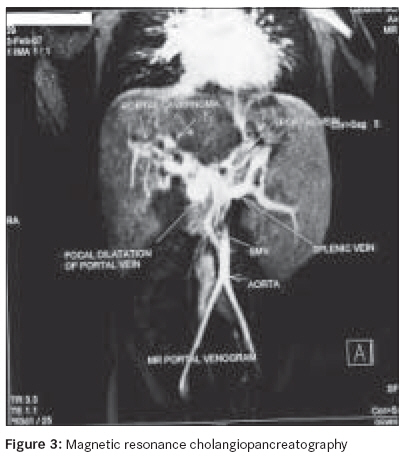
Her genotype was AA, and blood group was A +ve . Hepatitis B surface antigen (HBsAg) and antibody to hepatitis C (HCV) were negative. Abdominal ultrasound revealed hepatosplenomegaly, cavernous transformation of the portal vein, portal hypertension (extra-hepatic), gallbladder sludge, dilated intra-hepatic and common bile duct [Figure - 1] and [Figure - 2]. CT scan showed features highly suggestive of EHPVO with portal hypertension and terminal common bile duct stricture. Magnetic resonance cholangiopancreatography (MRCP) report showed features of cavernous malformation of the portal hepatic (old thrombosis recanalized); aneurismal dilatation and kink of the portal vein in hepatoduodenal ligament region, compressing the common bile duct; dilatation of biliary tree above the level of cystic duct insertion and left-sided portal hypertension with prominent coronary vein [Figure - 3] and splenomegaly . Upper gastrointestinal endoscopy was done, the results of which were essentially normal. A final diagnosis of PB was made. Endoscopic retrograde cholangiopancreatography (ERCP) was done, which showed proximal and mid-lower common bile duct strictures. Sphincterotomy with balloon dilatation was done, and a common bile duct stent was deployed with good drainage. She was discharged after 10 days of admission. In the last 6 months, she has had 3 stent replacements and she has remained stable. Discussion Gibson et al,[16] first reported the relationship between EHPVO and jaundice in 1965. Since then, several cases of obstructive jaundice due to CBD obstruction caused by cavernomatous transformation of portal vein (portal cavernoma) have been described. Williams et al,[17] were the first to report cholangiographic changes caused by choledochal varices, while Dhiman et al,[11] first described abnormalities on endoscopic retrograde cholangiography (ERC) in a prospective study. The pathogenesis of PB is not well known. It has been postulated that external pressure of portal cavernoma and/ or ischemia may play a role. [18],[19],[20] Histological and morphological studies have shown that cavernous transformation is not only dilatation of periportal collaterals but also neogenesis of vessels and formation of connective tissue occurring with increasing duration of thrombosis, which results in porous, tumor-like solid tissue that does not disappear after shunt surgery. [19],[20] Biliary strictures resulting in biliary obstruction may be caused by ischemia, or by encasement within a solid tumor-like cavernoma. [19],[20] The mechanism of ischemia resulting in bile duct damage in patients with EHPVO remains obscure. Although biliary abnormalities are seen in most patients with EHPVO, majority of them are asymptomatic and a few present with symptoms such as jaundice, pruritus, fever or pain in the abdomen. The patient under this report presented with deepening jaundice, low-grade fever and yellow urine, an indication of a progressive disease with cholangitis. There are 2 types of clinical features: (i) those related to chronic cholestasis, probably explained by strictures caused by either compression of the biliary lumen by enlarged collaterals or by ischemia as seen in this patient; and (ii) those related to biliary stones, which are probably responsible for biliary pain and cholangitis. [11] The diagnosis of PB is mostly made by ERCP. [4] The typical changes are irregularities in the CBD and hepatic ducts (smooth tapering strictures), and localized saccular dilatations and filling defects suggestive of CBD stones are possible. [4] A diagnosis of PB was made in this patient with both MRCP and ERCP, which showed the classical picture as highlighted under the case presentation described above. Abdominal ultrasound provides additional information regarding the presence of gallbladder varices (tortuous vessels in and around the gallbladder) and is helpful to provide the complete spectrum of PB. [21] Chandra et al,[22] graded the severity of biliopathy changes as follows:
On the basis of ERCP findings, our patient′s case fell into grade I, as graded by Chandra et al. It was interesting to note that upper GI endoscopy carried out on this patient was essentially normal; this was contrary to one′s expectations considering the several courses and years of injection sclerotherapy. Asymptomatic patients do not need any treatment, especially if the results of tests of liver function are normal. At present, strategies for the management of PB are selective and directed to symptomatic patients only. Treatment should be focused on the management of portal hypertension, and relief of obstructive jaundice due to the portal cavernoma can be managed endoscopically. [23],[24] Stenting with or without balloon dilatation of the CBD is recommended, and the stent needs to be replaced regularly. Portosystemic shunt surgery can be done in cases which cannot be managed endoscopically. The patient under discussion had balloon dilatation of the strictured CBD, and stent was deployed with good drainage. She has had 3 stent replacements in the last 6 months and has remained stable. It is the advice of the authors that patients presenting with features highly suggestive of EHPVO and PB should be adequately investigated and referred to centers where facilities are available for prompt interventions, as many lives have been saved through such interventions. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09039f1.jpg] [am09039f3.jpg] [am09039f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}