 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
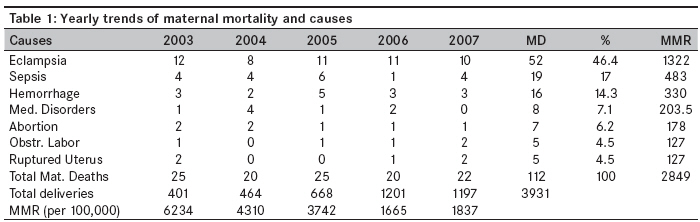
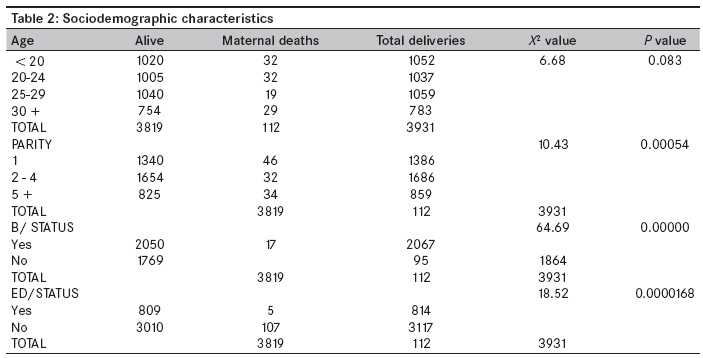
Annals of African Medicine, Vol. 8, No. 4, October-December, 2009, pp. 221-224 Original Article Trends in maternal mortality in a tertiary institution in Northern Nigeria Kullima AbubakarAli, Kawuwa MohammedBello, Audu BalaMohammed, Geidam AdoDanazumi, Mairiga AbdulkarimG Department of Obstetrics and Gynaecology, Federal Medical Centre, Nguru Code Number: am09048 PMID: 20139543 Abstract Objective: To look at the trends in maternal mortality in our institution over 5 years.Methods: Records of 112 maternal deaths were retrospectively reviewed to determine the trends and the likely direct cause of each death over the study period. Results: There were a total of 112 maternal deaths, while 3931 deliveries were conducted over the 5-year period. The maternal mortality ratio (MMR) was 2849/100,000 deliveries. The highest MMR of 6234/100,000 was observed in 2003, with remarkable decline to 1837/100,000 in 2007. Eclampsia consistently remained the leading cause, accounting for 46.4% of the maternal deaths, followed by sepsis and postpartum hemorrhage (PPH) contributing 17% and 14.3%, respectively. There were no statistically significant differences in the corresponding percentages of maternal deaths between various age groups (χ2=6.68; P =0.083). Grandmultiparas accounted for a significant proportion of maternal deaths as compared to low parity, with χ2=10.43; P =0.00054. Lack of seeking antenatal care (unbooked) and illiteracy were observed to be significant determinants of maternal mortality (χ2=64.69, P =0.00000; and χ2=18.52, P =0.0000168, respectively). Conclusion: In spite of decrease in the maternal mortality ratio over the years, it still remains high, with eclampsia persistently contributing most significantly. Community enlightenment on the need to avail of antenatal care and hospital delivery services, and improvement in the quality of skilled maternity care will, among other factors, drastically curtail these preventable causes of maternal death and reduce MMR. Keywords: Maternal mortality, Northern Nigeria, trends Introduction Since the inception of the Nairobi 1987 "safe motherhood" initiative, maternal mortality has evoked special interest among the global health and development agencies both at the regional and global level. Yet appreciable reduction in maternal mortality has not been achieved. [1] The difference between the developed and developing nations is unacceptably high, with risks of dying of 1 in 18 compared to 1 in 2228; and in terms of maternal mortality ratio (MMR), 740/100,000 compared to 20/100,000 live births in Africa and Europe, respectively. [2] A formal millennium summit in 2000 to address a reduction in maternal mortality was adopted as an international development goal by the Organization for Cooperation and Economic Development, World Bank, WHO, United Nations (UN) and the International Monetary Fund (IMF). [3],[4] This was endorsed by the149 heads of states present at the summit. The summit gave birth to the establishment of the Millennium Development Goals. MDG 5, the 5 th goal, is the reduction of maternal mortality by 75% by the end of 2015. [5] Though some degree of reduction in maternal death has been achieved in the developed countries, not much progress has been recorded in Africa and Asia. The latest global estimate, in 2005, showed maternal deaths of 535,900, with a maternal mortality ratio of 402/100,000 live births, and 95% of these deaths occurred in Africa and Asia, accounting for 50% (270,500) and 45% (240,600) of the deaths, respectively. [6] Nigeria was globally ranked 2 nd after India, with estimated number of maternal deaths being 58,500 in 2005. In Africa, Nigeria had the highest maternal mortality ratio, viz., well over 1000/100,000 deliveries. In Nigeria, the effort to reduce the high number of maternal deaths has received government priority, which informed the launching of the National Programme for the Prevention of Maternal Mortality (NPPMM) in 1986 with a view to expand and strengthen efforts towards advocating safe motherhood. [7] The northern part of the country is the worst, with an estimated maternal mortality ratio of 2151/100,000, [8] 2337/100,000 [9] and 2420/100,000 [10] deliveries in Sokoto, Makurdi and Kano, respectively, as reported in the institutional and population-based studies. From another institutional study in Jos, though the MMR was lower than highlighted above for the northern region, there was a significant increasing trend over just 4 years (though not during the same period), rising from 450/100,000 in 1990 to 1,060/100,000 deliveries in 1994. [11] Maternal mortality has been reported as a measure of standard of health care provided by the health care systems of a given society. [12],[13],[14] Nowhere can this reflection be better applied than in northern Nigeria, particularly the northeast, which is characterized by poor and sparsely distributed health facilities, coupled with inadequate and unskilled antenatal care staff and services. This study was undertaken to review the trend in maternal mortality in our institution with a view to determine the major causes of deaths and to ascertain if there are any significant deviations from other reports. Materials and Methods The study was a retrospective study of 112 maternal deaths recorded at the Federal Medical Centre, Nguru, over a 5-year period, from 1 st January 2003 to 31 st December 2007. The case notes of all pregnant women who died at the center were retrieved from the central medical library, and information pertaining to age, parity, booking status, level of education and probable cause of death was extracted for analysis. Chi-square was used to determine level of significance using epi info version 6. Results A total of 112 maternal deaths were recorded during the 5-year study period, and 3931 deliveries were conducted over the same period, giving a maternal mortality ratio of 2849/100,000 deliveries. The worst yearly MMR, viz., 6234/100,000, was observed in 2003; while in 2004 and 2005, the MMRs were 4310/100,000 and 3742/100,000 deliveries, respectively [Table - 1]. A remarkable decline to 1665/100,000 was observed in 2006, with a plateau in 2007. Eclampsia persistently remained the leading cause, accounting, overall, for 46.4% of the maternal deaths over the 5-year period, followed by sepsis and obstetric hemorrhage, accounting for 17% and 14.3% of maternal deaths, respectively. Medical disorders of pregnancy and abortion-related complications were the cause in 7.1% and 6.2%, respectively, while ruptured uterus and obstructed labor each were the cause in 4.5% of the deaths. There were no statistically significant differences in the corresponding percentages of maternal deaths between various age groups (χ2 = 6.68; P = 0.083). Grandmultiparas accounted for a significant proportion of maternal deaths compared to those of low parity, with χ2 = 10.43; P = 0.00054. Lack of seeking antenatal care (unbooked) and lack of formal education (illiteracy) were observed to be significant determinants of maternal mortality, with c2 = 64.69, P = 0.00000; and χ2 = 18.52, P = 0.0000168, respectively, as observed in [Table - 2]. Discussion The maternal mortality ratio of 2849/100,000 observed over the study period was the highest in the northern part of the country, which has the greatest burden of maternal mortality reported earlier in Sokoto, [8] Makurdi [9] and Kano. [10] There was a dramatic drop in the yearly trend, from as high as 6234/100,000 deliveries in 2003 to 1665/100,000 deliveries in 2006; this may be as a result of the substantial increase in the number of women who resorted to hospital deliveries at that time. Though may not be significant, the slight increase in the MMR seen in 2007 was equally as a result of the observed drop in the total deliveries recorded over the period. This finding however differs significantly from the observed trend in Jos earlier reported by Ujah (though 14 years earlier), which shows an increase over a 4-year period, from 450/100,000 in 1990 to 1060/100,000 deliveries in 1994. [11] Eclampsia was consistently observed to be the leading cause of maternal mortality throughout the study period and, overall, accounts for 46.4% of the total number of maternal deaths over the 5-year study period. This corroborates findings from other studies in Nigeria, which show that eclampsia was the leading cause of maternal mortality. [10],[15],[16] Abortion-related maternal deaths, which were currently observed to constitute 11% to 40% of the total maternal mortality in some reports in Nigeria, [17],[18],[19],[20] were however the least in this study, which might not be unrelated to low prevalence or under-reporting of induced abortion, which is seriously frowned at due to the cultural and religious orientation of the community of this area. Nearly 60% of the deaths were observed in those below 25 years of age, which might not be surprising as early age at first marriage and high fertility of this group are factors that contribute to increased susceptibility to pregnancy complications and mortality. As observed in other studies, [10],[21],[22],[23] illiteracy and non-utilization of antenatal care services were observed to be significant determinants of maternal mortality in this study also. Conclusion In spite of the decrease in the maternal mortality ratio over the years, it still remains high, with eclampsia persistently contributing significantly. Grandmultiparas, illiteracy and lack of prompt antenatal care (ANC) services were found to be significant contributors to maternal deaths in our study. Community enlightenment to inspire women to avail of ANC and hospital delivery services; improvement in skilled maternity care, especially for preeclampsia, toxemia and sepsis; and prevention of PPH will, among other factors, drastically curtail these preventable causes of maternal death and reduce MMR. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09048t1.jpg] [am09048t2.jpg] |
| |||||||||

{kind=link}
{kind=link}