 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
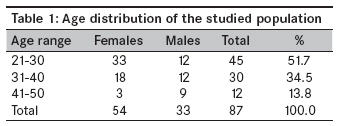
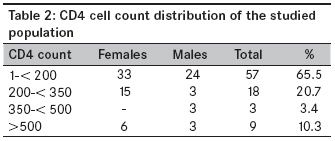
Annals of African Medicine, Vol. 8, No. 4, October-December, 2009, pp. 257-260 Short Report CD4+ T-Lymphocytes cell counts in adults with human immunodeficiency virus infection at the medical department of a tertiary health institution in Nigeria Ajayi AO, Ajayi EA, Fasakin KA Department of Medicine, Federal Medical Centre, PMB 201, Ido-Ekiti Code Number: am09054 PMID: 20139549 Abstract Objectives: To evaluate the CD4+ cell counts in adults with human immunodeficiency virus (HIV) infections presenting at the medical department of the Federal Medical Centre, Ido-Ekiti, Nigeria.Methods: This study was carried out at the medical department of the Federal Medical Centre (FMC), Ido-Ekiti, Nigeria, in the period July-December 2006. FMC, Ido, was recently upgraded to serve as the only center for HIV/AIDS referral, diagnosis and treatment in Ekiti State. The center offers free antiretroviral therapy. All patients with a diagnosis of HIV/AIDS, either diagnosed at the center or referred from other hospitals, admitted to the medical department within the study period had their blood sample taken for CD4 cell counts estimation at the first visit to the center, as part of the routine workup to assess their disease status and need for antiretroviral therapy. Results: A total of 87 patients comprising of 54 (62.1%) females and 33 (37.9%) males had their CD4+ T-Lymphocytes cell counts evaluated within their first week of presentation. The total mean age of the population studied was 33.17 ± 7.01 years. The mean age of the females was 31 ± 5.6 years, while that of the males was 36.5 ± 8.2 years. The difference between the mean ages of females and males was statistically significant (P = 0.0004). The female: male ratio was 1.6:1. Out of the 87 patients, 30 were referrals from other hospitals within the state. The total mean CD4+ cell count was 230.7 ± 311.9 cells/µL. The mean CD4 cell count of females was 212.17 ± 264.96 cells/µL, while that of males was 261.0 ± 389.19 cells/µL. This difference was not significant (P = 0.4876). Majority of the patients (75, [86.2%]), had CD4 cell count < 350 cells/µL, comprising of 48 females and 27 males. Of the 75 patients, 57 (76%) had a CD4 cell count < 200 cells/µL (33 females vs. 24 males). Conclusion: At the time of HIV diagnosis, majority of our patients had a CD4+ cell count < 200 cells/µL. This was consistent with a relatively advanced disease. More women than men in the population were found positive for HIV. More sustained and vigorous awareness campaigns need be embarked upon in the HIV propaganda in the Ekiti State on one hand and Nigeria on the other hand to bring down this Hydra-headed monster called HIV/AIDS. Keywords: CD4+ T-lymphocyte cell count, HIV/AIDS infections, Tertiary health institution Introduction CD4+T lymphocyte cell count is a major indicator of the stage of the disease in human immunodeficiency virus (HIV)-infected individuals. [1],[2] Depletion of CD4+ T cells is one of the hallmarks of progression of HIV infections. [3] The absolute CD4 cell count is used routinely in the evaluation and monitoring of HIV-infected persons. [4] CD4 cell counts have been found to have good correlation with development of various complications in HIV/AIDS. [5] In general, patients with low CD4+ T cell counts have been infected with HIV for longer periods of time than have patients with higher CD4+ T cell counts. [6] In this regard, it is clear that individuals who begin highly active antiretroviral therapy (HAART) when their CD4+ T cell counts are < 200 cells/µL have a significantly poorer response to therapy and a worse prognosis when compared with individuals who begin therapy when their CD4+ T cell counts are higher. [2],[7],[8],[9],[10] CD4+ T-lymphocyte cell count is a standard test to stage HIV disease and to make therapeutic decisions regarding antiretroviral therapy and prophylaxis for opportunistic pathogens. [11] It is also a relatively reliable indicator of prognosis, and it complements the viral load assay. These two assays independently predict clinical progression and survival. [1] We carried out this study to determine at what stage in the disease HIV-infected persons present to our treatment facility, and to have a comparison with what is obtained in other centers. Materials and Methods This study was carried out at the medical department of the Federal Medical Centre (FMC), Ido-Ekiti, Nigeria, in the period July-December 2006. FMC, Ido, was recently upgraded to serve as a center for HIV/AIDS referral, diagnosis and treatment in Ekiti State. The center offers free antiretroviral therapy. All patients with a diagnosis of HIV/AIDS, either diagnosed at the department or referred from other hospitals, admitted to the medical department within the study period had their blood sample taken for CD4 cell counts estimation at the first visit to the center, as part of the routine workup to assess their disease status and need for antiretroviral therapy. CD4 cell counts were determined using a freshly taken blood sample drawn into a 2-mL Ethylene Diamine Tetra-acetic Acid (EDTA) anticoagulant bottle and processed within 2 hours of venesection. The samples were prepared and run on the Coulter Epics XL flow cytometer (Bechman Coulter Inc., Fullerton, California, USA) according to the manufacturer′s instructions. The data generated were analyzed using the SPSS. Results A total of 87 patients comprising of 54 (62.1%) females and 33 (37.9%) males had their CD4+ cell counts evaluated within their first week of presentation. Of the 87 patients, 35 were referrals from other hospitals within the state. The overall mean age of the study population was 33.17 ± 7.01 years (range, 23-50 years). The mean age of the females in this study was 31 ± 5.6 years, while that of the males was 36.5 ± 8.2 years. The difference between the mean ages of females and males was statistically significant (P = 0.0004). Majority (51.7%) of the patients were in the age group 21-30 years. Females constituted a higher proportion in this age group (33 females as against 12 males); this difference was not statistically significant [Table - 1]. The mean CD4+ T-Lymphocytes cell count of the study population was 230.7 ± 311.9 cells/µL. The mean CD4 cell count of females was 212.17 ± 264.96 cells/ µL, while that of the males was 261 ± 389.19. Again, the difference here was not statistically significant (P = 0.4876). Majority (86.2%) of the patients had their CD4 cell count < 350 cells/ µL. Fifty-seven (65.5%) patients had their CD4 cell count < 200 cells/µL (33 females as against 24 males) (P = 0.3526). Only 9 patients had their CD4+ cell count> 500 cells/µL [Table - 2]. All patients with CD4+ cell count < 200 cells/µL were symptomatic at the time of presentation. In all, 13 patients were asymptomatic. It is interesting to know that 3 out of the 9 patients that had their CD4+ cell count> 500 cells/µL were symptomatic at the time of presentation. Majority (75.8%) of the patients had a hemogram of < 10 g%. Discussion Current treatment guidelines recommend that therapy should be initiated when CD4+ T-lymphocyte count is # 350 cells/µL. [12],[13] It had been reported that HIV-infected persons with lower CD4+ cell counts have been infected for longer periods of time as compared to those with higher CD4+ cell counts. [6] Studies have reported that patients with CD4+ cell counts < 200 cells/ µL have both a poorer response to HAART therapy and a worse prognosis than do individuals with higher CD4+ cell counts at the time of initiation of therapy. [2],[13],[14] The present study showed that 86.2% of our patients had relatively advanced disease as reflected by their CD4+ cell counts of < 350 cells/µL. Of particular interest is the fact that 65.5% of this studied population had a CD4+ cell count of < 200 cells/ µL at the time of initial diagnosis. The figures obtained in this study were similar to those obtained in the studies by Kilaru et al. [11] in Barbados and Guarner et al. [15] in Mexico. The results obtained in this study clearly showed that majority of the HIV-infected patients were diagnosed quite late in the course of HIV disease. The reasons for this observed delay are multifactorial. One is the level of denial among the individuals; the other factor may be the real or perceived social stigma toward HIV-infected persons and the fear of suffering discrimination in the society. Also, the hospital was recently upgraded as a referral center for diagnosis and treatment of HIV/AIDS; this may have encouraged patients with suspected infection to assess their disease status and seek treatment. Due to delayed presentation, most of our patients were in clinical categories B and C at the time of their presentation. The individuals in this study with CD4+ cell count of < 200 cells/µL are at the risk of rapid disease progression and worse prognosis despite initiation of HAART therapy, based on current knowledge on HIV disease. We also found that majority (51.7%) of the patients in this study were in the age group 21-30 years, with the number of females (33) being more than that of males (12). This is similar to the findings by Kilaru et al., [11] and in contrast to the Mexico findings. [15] We also found in this present study that males had a higher CD4+ cell counts (261 ± 389.19) than their female counterparts (212.17 ± 264.96). This difference was not statistically significant. Conclusion At the time of HIV diagnosis, majority of our patients had a CD4+ cell count < 200 cells/µL. This was consistent with a relatively advanced disease. More women than men in the study population were found positive for HIV. More sustained and vigorous awareness campaigns need to be undertaken in the HIV propaganda programs in the Ekiti State on one hand and Nigeria on the other hand to bring down this Hydra-headed monster called HIV/AIDS. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09054t1.jpg] [am09054t2.jpg] |
| |||||||||

{kind=link}
{kind=link}