 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 8, No. 4, October-December, 2009, pp. 266-270 Short Report Circumcision mishaps in Nigerian children Osifo OD, Oriaifo IA Department of Surgery, Paediatric Surgery Unit, University of Benin Teaching Hospital, Benin City Code Number: am09056 PMID: 20139551 Abstract Background/Objective: Circumcision may be associated with complications which are usually minor but could be life threatening on certain occasions.
This study determined contributory factors, pattern of presentation, challenges of management and outcome of circumcision mishaps in Benin City, Nigeria.
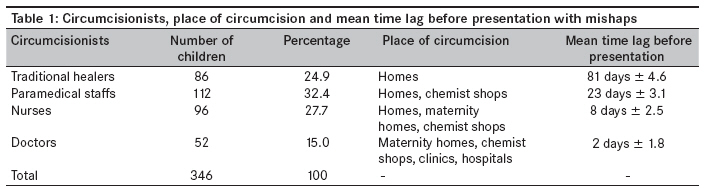
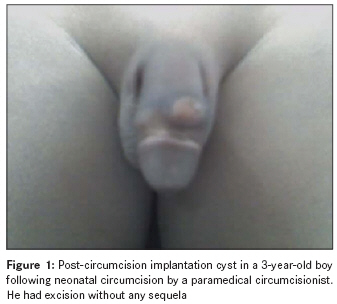
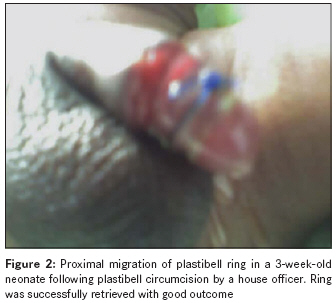
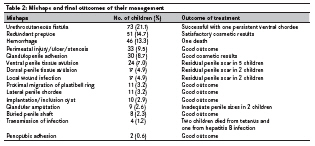
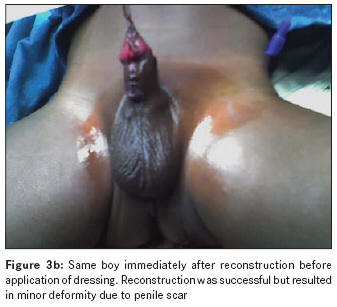
Keywords: Children, circumcision, foreskin, mishaps Introduction Circumcision is the most common surgical procedure, widely performed by both the orthodox and unorthodox health care providers, especially in Nigeria. [1] Many methods of circumcision have been described; but irrespective of the method employed, circumcision continues to be one of the oldest surgical procedures with the highest complication rates. [1],[2],[3],[4] In this subregion, minor complications such as redundant prepuce, penile scars and glandulopenile adhesion are accepted as normal because they do not interfere with sexual performance. Medical consultation is rarely sought for these complications. [1],[2] On the other hand, glandular amputation, urethrocutaneous fistula, transmission of infections and uncontrolled hemorrhage are unacceptable complications of circumcision. [5],[6],[7] In Sub-Saharan Africa, all male children are routinely circumcised. Majority of circumcisions are performed during the neonatal period, except on health grounds. [3],[4] Religion, custom and cultural rites which are sometimes part of initiation to manhood are the major indications in many communities. [1],[2],[ 3] Not being circumcised is regarded as taboo, uncultured and uncivilized and is treated with contempt in traditional African culture. [1],[4] Hence circumcision remained an accepted practice by the literate and illiterate before and even after the advent of western civilization. Many literatures [8],[9],[10],[11] reported complications following circumcision. These brought into question the rationale for circumcision, which resulted in a tilt towards "no circumcision" in many highly developed cultures. [5],[6],[7],[8],[9] Although circumcision is regarded as very common in this subregion, there are not many studies on the prevalence of, and factors influencing, circumcision mishaps in our setting. This retrospective study determined the pattern of presentation, challenges of treatment, outcome and various factors that contributed to circumcision mishaps in children in Benin City, Nigeria. Materials and Methods Male children who presented to the Pediatric Surgery Unit of the University of Benin Teaching Hospital between January 1998 and December 2007 with complications after circumcision were retrospectively studied. Their case files were retrieved from the medical records and analyzed for age at circumcision, the health personnel who circumcised, place of circumcision, complications recorded, contributory factors, time of presentation, treatment and its challenges and the final outcome. Five children who were discharged against medical advice on insistence of their parents were excluded from the study. Statistical analysis The data were analyzed using SPSS version 11 (SPSS, Chicago, 111) software package and presented as count, frequency and percentage. Categorical data were analyzed using Chi-square test, and where necessary, P values < 0.05 and> 0.05 were regarded as significant and nonsignificant, respectively. Results A total of 346 male children who were aged between 6 days and 12 years presented to the unit with complications; the time of presentation ranged between 1 hour and 12 years after circumcision. They accounted for 24% of the 1096 children treated for urological lesions over 10 years. Religion, custom and cultural practice were the reasons for circumcision in all the children. The majority (301, [87%]) of children had circumcision performed as routine neonatal procedure, while 45 (13%) were circumcised after neonatal period. As shown in [Table - 1], orthodox practitioners recorded 210 (75.1%) of the complications as against 86 (24.9%) recorded by traditional practitioners. Paramedical practitioners who had not received any form of training on circumcision recorded the highest number of circumcisions (112, [32.4%]). They were followed by nurses (96, [27.7%]) and doctors (52, [15.0%]). Of the 52 circumcisions performed by doctors, 46 (88.5%) were performed by house officers who were still undergoing training, while 6 (11.5%) were performed by general practitioners. Urethrocutaneous fistula (73, [21.1%]), redundant prepuce (51, [14.7%]), hemorrhage (46, [13.3%]), glandular injury (33, [9.5%]), glandulopenile adhesion (30, [8.7%]), implantation cyst (10, [2.9%]) [Figure - 1], proximal migration of plastibell ring (11, [3.2%]) [Figure - 2] and penile tissues avulsions (17, [4.9%]) [Figure - 3]a were more commonly seen than glandular amputations (9, [2.6%]), transmission of infection (4, [1.2%]), local wound infections and penopubic adhesion (2, [0.6%]). Those with hemorrhage presented much earlier than those with infections, glandular injuries, scars and adhesions. Also, those circumcised by doctors in maternity homes, clinics and hospitals presented with complications within an average of 2 days following circumcision. Other children presented with complications after a mean time lag of 81 days following circumcision by traditional practitioners, 23 days following circumcision by paramedical staff and 8 days following circumcision by nurses. Those who were not doctors performed circumcisions at homes, maternity homes and chemist shops with unsterilized instruments. Native concoctions, petroleum jelly and different topical agents were used for post-circumcision dressing. Challenging mishaps and late presentation were more common among children circumcised by those who were not doctors and by traditional practitioners ( P < 0.0001). The types, frequencies, treatments and final outcomes of the circumcision mishaps are as depicted in [Table - 2]. Treatment was easy in many patients, but closure of urethrocutaneous fistulae, penile reconstruction following penile tissues avulsion and glandular amputation were challenging. Closure of fistulae and penile reconstruction [Figure - 3]b were successful, but recurrent fistula formation was common. Pressure dressing controlled hemorrhage in many children, but 1 of the 4 with bleeding diathesis died due to irreversible shock as a result of late presentation. Three children developed tetanus, with a mortality rate of 66.7%, and 1 child who developed hepatitis B infection subsequently died; these children were in terminal stages of the diseases on arrival. Children who had transmission of infections, local wound infections, as well as the child who died from bleeding diathesis, were circumcised by traditional practitioners. Overall, successful treatment was achieved in 322 (93.1%) children, and penile sizes were grossly inadequate after reconstruction in 2 children with amputation. Poor cosmetic results, penile torsion and persistent chordee were recorded in 18 (5.2%) children, while a total of 4 (1.2%) deaths were recorded. Discussion The number of children treated for circumcision mishaps constitutes a large proportion of children treated for urological lesions in many referral centers in Sub-Saharan Africa. [12] Treatments for circumcision mishaps accounted for 24% of pediatric urological workload during the study period, which tallies with earlier observations in similar referral centers. [10],[11],[12],[13] Although religious and cultural circumcisions were performed in the neonatal period, many children with mishaps presented after the neonatal period. The time of presentation was influenced by the type of mishap, as well as by parental and circumcisionists′ awareness. Hence children with hemorrhage, although many were in shock on arrival, presented earlier than those with penile adhesions; and those circumcised by doctors presented earlier than those circumcised by persons who were not doctors, as also reported by previous authors. [10],[11] Although all circumcisionists recorded complications, the range of mishaps and time lag before presentation differ considerably. The level of training, place of circumcision and post-circumcision care were important factors in determining the type of injury, mode of presentation, challenges of treatment and final outcome. [10] Consequently, unacceptable complications and poor cosmetic outcomes increased as the level of training of the circumcisionists decreased, as also observed by other researchers. [5],[6],[10],[11],[12],[13],[14] Proximal migrations of plastibell rings were recorded by house officers and nurses only. This is perhaps because plastibell circumcision method may not have been mastered by the practitioners, which is in agreement with the reports by other authors. [12],[15],[16],[17] In view of this, previous reports [18],[19] have emphasized the importance of adequate training and supervision of circumcisionists, particularly those in rural areas. Many children were circumcised in unhygienic environments; with unsterilized instruments; or without local anesthesia (Xylocaine infiltration), analgesia and postoperative antibiotics. These resulted in regrettable and avoidable mishaps. Moreover, many among the paramedical staff, nurses and house officers did not have access to standard operation theater, adequate surgical instruments and did not have adequate training on circumcision. These factors led to many circumcisions being done at homes, maternity homes and chemist shops, resulting in many avoidable complications. The transmissions of hepatitis and neonatal tetanus were associated with big challenges and higher morbidity and mortality as the children were presented when they were in the terminal stages of the disease. [10],[11] These could have been prevented if postoperative antibiotics were given and the children presented early for treatment. Application of native concoctions by traditional circumcisionists compounded the problems and resulted in penile tissues fasciatis. The nonprovision of local anesthesia and analgesia for circumcision was unethical because neonates do perceive pain, as reported by earlier researchers. [20],[21] Although other authors reported [10] children who manifested features of, and were diagnosed with, HIV infection following circumcision, such incident was not recorded in this study despite the fact that the circumcisions were done under similar circumstances. The need for urinary diversion, special dressing, microsurgical instruments, fine sutures and expertise in fragile tissue handling made penile reconstruction very challenging in children who developed post-circumcision urethrocutaneous fistulae, penile tissues avulsion and glandular amputation. Consequently, repairs of these mishaps were complicated by recurrent fistula formation, scarred penis and inadequate penile sizes, unlike an excellent report [8] of repair that one can expect in a more sophisticated center. Conclusion Circumcision mishaps were common, the children presented late and the mishaps were challenging to manage in our setting, with resultant residual penile deformities and preventable mortalities. Inadequate training of circumcisionists; circumcision in unhygienic environment; circumcision with unsterilized instruments; circumcision without anesthesia, analgesia, antibiotics; and delayed referrals played significant and contributory roles in the development and final outcome of the mishaps. Public enlightenment on safe circumcision practice may help reduce post-circumcision morbidity and mortality. Early referral of children with post-circumcision mishaps should be encouraged and emphasis placed on hospital circumcision by experts. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09056f3b.jpg] [am09056f3a.jpg] [am09056t2.jpg] [am09056t1.jpg] [am09056f2.jpg] [am09056f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}