 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
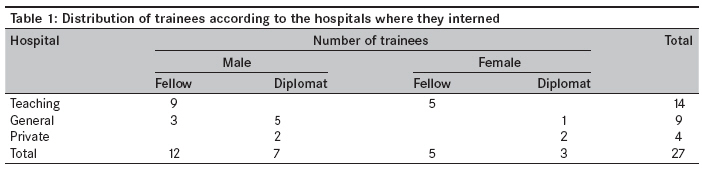
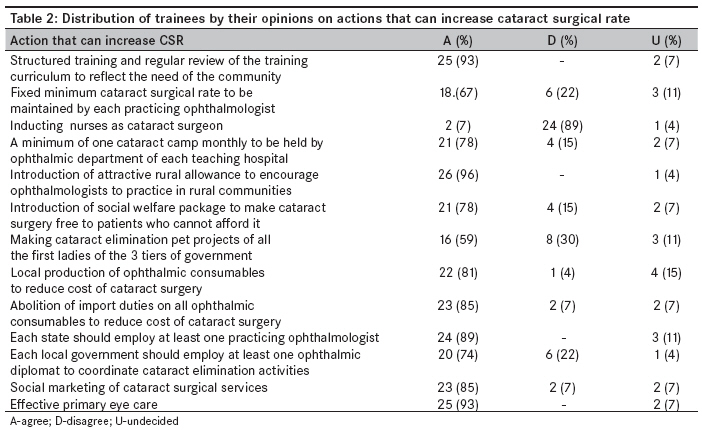
Annals of African Medicine, Vol. 8, No. 4, October-December, 2009, pp. 276-280 Short Report Trainee ophthalmologists' opinions on ways to improve cataract surgical rate Ayanniyi AbdulkabirAyansiji, Adepoju FeyiGrace, Owoeye JoshuaFoluso Department of Ophthalmology, University of Ilorin Teaching Hospital, Ilorin, Kwara State Code Number: am09058 PMID: 20139553 Abstract Objective: To know the opinions of trainee ophthalmologists on ways to improve cataract surgical rate (CSR) with a view to having insight into actions that should be of high priority for achieving this improvement.Methods: A survey of 27 trainee ophthalmologists using structured self-administered questionnaire. Results: Most trainees had a positive view about actions towards raising CSR: Structured ophthalmic training- 25 (92.6%), monthly cataract camps by eye departments in teaching hospitals- 21 (77.8%), rural allowance for ophthalmologists- 26 (96.3%) and welfare package for indigent cataract patients- 21 (77.8%). Other actions included local production of cataract consumables- 22 (81.5%), duty-free importation of ophthalmic materials- 23 (85.2%), employment of ophthalmologists in the services of the state governments- 24 (88.9%) and local governments- 20 (74.1%), effective primary eye care- 25 (92.6%) and marketing of cataract surgical services- 23 (85.2%). However, only 16 (59.3%) trainees wanted first ladies (wives of the president, governors and local government chairmen) to adopt cataract elimination as pet projects, and 24 (88.9%) opposed the introduction of cataract surgeons. Conclusion: Most trainees had positive perceptions about most actions that can raise CSR. However, top-priority actions to improve CSR were attractive rural allowance, structured training, resource availability, cost reduction and marketing of cataract surgical services. Multiple actions might be necessary to raise CSR. Keywords: Cataract surgical rate, opinion, priority actions, trainees Introduction The numbers of cataract surgeries done in Sub-Saharan Africa fall short of ′Vision 2020′ targets. [1] This is even worrisome in West Africa (WA), especially Nigeria, where cataract surgical rate (CSR) falls below 500, compared to India and affluent economies, where CSR is at least 3000. This is of concern to the stakeholders in the eye care industry in the subregion. [2],[3] Cataract is the leading cause of avoidable blindness the world over, more especially in income-limited economy such as WA. [4] Achieving the mission of ′Vision 2020′ by eliminating the avoidable causes of blindness, among which cataract is a major one, can largely be through increasing CSR in the income-limited economy such as WA. [5] CSR is a performance indicator and is the total number of cataract operations performed per million of the population over a period of 1 year in a given locality, usually a country. CSR can also serve as an indicator of the availability, accessibility and affordability of cataract surgical services. [6] A number of actions at the individual, group, organization and government levels can have positive influence on CSR if given the needed attention. Different ways to improve CSR are available across the globe. [5] However, in the face of competing demands for scarce resources, there is the need to prioritize actions so as to employ those ones that will produce optimal results. It is a fact that trainee ophthalmologists are aware of the current ophthalmic issues such as cataract, more especially of how to improve CSR. Furthermore, trainees are potential decision makers and implementers of eye care plans; thus trainee ophthalmologists′ opinions should be respected as these should positively affect the plan of action on CSR. To the authors′ best knowledge, this is the first work wherein trainees′ opinion was sought on how to improve CSR in Nigeria. The objective of the study was to know the opinions of trainee ophthalmologists on ways to improve CSR with a view to having an insight into actions that should be of high priority for achieving this improvement and in order to optimize available resources towards this end. Materials and Methods A self-administered structured questionnaire was distributed to 34 trainee ophthalmologists who attended the Community Eye Health (CEH) 2006 module; the questionnaire was given to every trainee at the end of the fifth week of the 6-week course held in the CEH 2006 module from 27 th February 2006 to 7 th April 2006. These were collected at the venue of the course at the end of the sixth week of the course. The trainees were from 23 different hospitals - 22 in Nigeria and 1 in Ghana. Included in the questionnaire were questions related to socio-demographic data of the trainees, such as age, sex, marital status, place of work, designation and duration in ophthalmic training. Other questions were related to information on actions that can increase CSR, such as structured ophthalmic training program/regular review; fixed minimum CSR to be achieved by ophthalmologists; induction of cataract surgeon and ophthalmic team in teaching hospitals; holding a minimum of one cataract outreach eye camp monthly; introduction of attractive rural allowance to encourage ophthalmologists to practice in rural areas; social welfare package making cataract surgery free for indigent cataract patients; first ladies (wives of the president, state governors and local government chairmen) adopting cataract elimination as pet projects; local production of ophthalmic consumables; removal of import duties on ophthalmic consumables/equipment; employment of at least one ophthalmologist by each state and each local government; social marketing of cataract surgical services; and effectiveness of cataract elimination in the primary eye care services. The trainees were to indicate ′agree,′ ′disagree′ or ′undecided′ for each of the actions to improve CSR. The opinions were collated, entered into SPSS 12.0.1., and a simple proportion analysis was carried out. Results Twenty-seven (75%) out of the 34 trainees from 23 different hospitals (22 in Nigeria and 1 in Ghana) who attended the CEH 2006 module in Kaduna, Nigeria, consented to participate in the study and filled and returned the questionnaires. They included 17 (63%) trainee ′fellows′ (14 [52%] senior registrars and 3 [11%] registrars) and 10 (37%) trainee ′diplomats.′ There were 19 (70%) men and 8 (30%) women, with a male-to-female ratio of 2.4:1 [Table - 1]. Their ages ranged from 31 to 50 years, with a mean of 37 years, standard deviation (SD) of 6 years and modal age of 32 years. Twenty-four (89%) trainees were married and 3 (11%) were single. The duration in ophthalmic training ranged between 1 and 6 years, with a mean of 3 years and SD of 2 years. [Table - 2] shows the distribution of trainees by their opinions on actions that can increase cataract surgical rate (CSR). Inducting nurses as cataract surgeon (C) to raise CSR was unpopular with the trainees as 89% of the trainees disagreed. Introduction of attractive rural allowance (10-20% of basic salary) to encourage ophthalmologists to practice in rural communities (E) was the most popular as 93% of the trainees agreed; and making cataract elimination pet projects of all the first ladies of the 3 tiers of government (G) was the least popular, with only 59% of the trainees agreeing and 30% disagreeing. Discussion These findings are representative of the opinions of trainee ophthalmologists as 75% of them participated in the study and also were from various training hospitals. Nearly all had positive attitude towards actions that could raise cataract surgical rate (CSR). Most trainees were found to be likely to support actions that would raise CSR. Although nearly all trainees were from hospitals in Nigeria, their views could be applicable elsewhere too, especially in the West Africa subregion, as most factors that are responsible for low CSR are common in all subregions. [2],[3] The observed male preponderance in this study may indicate a greater interest in ophthalmology among the males. [7] Expectedly, trainees preferred structured training and regular review of the training curriculum. The training curriculum should be structured to reflect societal needs. CSR can be raised if each ophthalmologist targets to perform a fixed minimum number of cataract operations yearly. This has been successfully implemented in India, where the norm is 700 operations per year. [8] It is a fact that ophthalmologists provide more than just cataract services; however, ophthalmologists in resource-limited economies across the globe, including West Africa (WA) and especially Nigeria, have to rise up to the challenge of result-oriented performance by the work force, which Faal observed in her faculty lecture to be a major issue in order to raise CSR in WA. [3] Though there are reports of good performance by cataract surgeons, [9],[10],[11] the induction of cataract surgeons was unpopular among trainees in this study. This may be related to the belief that cataract surgeons may extend their services beyond the job specification, resulting in abuse of ophthalmic practice and quackery, especially in Nigeria and Ghana. Additionally, the ophthalmic diplomat program in WA could be seen to have taken care of the role expected of cataract surgeons. There may also be satisfaction that ophthalmic diplomats are medical doctors who are qualified to carry out surgery, apart from additional 2 years of postgraduate structured training in ophthalmology, unlike cataract surgeons who are qualified ophthalmic nurses with additional 12-month on-the-job training in cataract surgery. [12] Inducting nurses as cataract surgeons were previously unacceptable to all Anglophone WA countries [12] and to date to Nigeria and Ghana [10] however, they have been successfully inducted in The Gambia and its neighboring nations. [11] It is a fact that there are more ophthalmologists in cities, while they are mostly beyond the reach of poor cataract patients in rural communities. [2] Attractive rural allowance most likely would encourage young ophthalmologists to practice in rural areas, while teaching hospitals holding monthly outreach cataract eye camps would assist in reaching the unreached in rural areas and most likely raise the CSR. Furthermore, by having functional primary eye care (PEC) services in place, the unreached/underserved communities can be served. It has been observed that the development of ′bridging strategies′ that create a strong link between hospitals providing clinical service and communities needing these services could increase CSR in Sub-Saharan Africa. [1] First ladies as implied by the study constitute wives of the president, the governors and the local government chairmen. In recent years, especially in Nigeria, it is a practice among first ladies to embark on ′pet projects′ (usually financed by funds raised using position of influence - ′office of first ladies′) that are expected to assist the public. First ladies adopting cataract surgical services (CSS) as pet projects and employing practicing ophthalmologists in government services are likely to encourage government funding of CSS and are most likely to raise CSR. However, almost 30% of the trainees were not enthusiastic about first ladies adopting CSS as a pet project. This might be out of fear of sustainability of such a project. Local production of ophthalmic consumables, as well as making consumables/equipment duty free, would most likely reduce the cost of CSS and raise CSS uptake and CSR. Social welfare package for indigent cataract patients who are unable to afford CSS would raise CSR. Most cataract patients are aged, visually incapacitated and usually unproductive and would need assistance to get CSS. Cost is a major barrier to uptake of CSS in resource-limited economies, including the WA subregion. [13],[14],[15],[16],[17] Social marketing of CSS most likely would boost uptake of CSS and raise CSR. This involves creating demand for CSS by getting cataract patients informed about where to get quality, accessible and affordable CSS. Outreach programs and patient counseling are powerful marketing techniques to generate demand for eye care. [18] Concluding, most trainees had positive perceptions about most of the actions that can raise CSR. However, top-priority actions were attractive rural allowance, structured training, resource availability, cost reduction and marketing of cataract surgical services. Multiple actions might be necessary to raise CSR. Acknowledgment The authors are highly grateful to the cohort of trainee ophthalmologists (CEH 2006 module) who participated in the study; and the Department of Community Eye Health, National Eye Centre, Kaduna, Nigeria. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09058t2.jpg] [am09058t1.jpg] |
| |||||||||

{kind=link}
{kind=link}