 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 9, No. 1, January-March, 2010, pp. 5-10 Original Article Depression among medical outpatients with diabetes: A cross-sectional study at Jos University Teaching Hospital, Jos, Nigeria Agbir TM, Audu MD, Adebowale TO, Goar SG Department of Psychiatry, Jos University Teaching Hospital, Jos Code Number: am10002 PMID: 20418642 DOI: 10.4103/1596-3519.62617 Abstract Background: Clinical depression is a common problem among patients who seek medical care, and diabetic patients with comorbid depression tend to have higher health care cost. A dearth of literature exists on depression among diabetics in Nigeria. The objectives of the study were to determine the prevalence of depression among diabetic patients and to determine the sociodemographic correlates of depression among diabetics.Methods: A cross-sectional descriptive study was conducted between December 2005 and April 2006 among patients who attend the diabetes clinic of Jos University Teaching Hospital (JUTH) with a laboratory and clinical evidence of diabetes mellitus. A semi-structured questionnaire was used to record the sociodemographic data of each consecutive patient followed by an interview by psychiatrists using the depression module of the Structured Clinical Interview for DSM-I V axis I disorder (SCID). Subsequently, the Hamilton Rating Scale for Depression (HDRS) was used to determine the severity of symptoms among subjects diagnosed with depression according to DSM-I V criteria. Results: Thirty-one of the 160 subjects fulfilled the DSM-IV criteria for the diagnosis of a major depressive episode giving a 1-year prevalence rate of 19.4%. Depression was significantly correlated with sex (P=0.001) with a female-to-male ratio of 3:1 and was also significantly associated with unmarried diabetics (P=0.002) and those who had a poor relationship with their partners (P=0.04). No significant association was found between depression and the respondents' age (P=0.216), educational qualifications (P=0.268), employment status (P=0.84), place of residence (P=0.80), household composition (P=0.77), and monthly income (P=0.110). Conclusion: Depression is a common psychiatric disorder among diabetic subjects in this environment. It was suggested that diabetic patients be screened for depression to allow for early detection and treatment. Keywords: Depression, diabetes, sociodemographic correlates Introduction Diabetes mellitus (DM) is present in all parts of the world, with varying prevalence rates from one region to another and between rural and urban population. [1],[2] The World Health Organization (WHO) estimates that there are about 100 million person with DM worldwide. [2],[3] In Nigeria, findings from a community-based study in Lagos metropolis in 1969 by Johnson [4] yielded a prevalence of 0.55%. In 1992, the national expert committee on noncommunicable diseases [5] quoted the crude prevalence of DM in Nigeria as 2.73%. Depression, a mood disorder, [6] is known to occur at higher rates in patients who seek general medical care [7] and nearly 70% of all antidepressant prescriptions are written by primary care physicians. [8] Patients who suffer from both depression and diabetes also tend to have higher health care cost in primary care. [9] A review of the prevalence of depression in adults with diabetes in meta-analytic study revealed depression to be commoner among diabetic than nondiabetic group with the odds of depression in the diabetic group to be twice that of the nondiabetic comparison group. [10] Similarly, the prevalence of comorbid depression was significantly higher in diabetic women (28%) than in diabetic men (18%). [10] In another study of prevalence of major depression and other psychiatric disorders in patients with long-standing type 1 diabetes mellitus in Minnesota, Popkin et al. [11] found the lifetime prevalence of major depression among these patients to be 22.9% for males and 25.9% for females; both rates were significantly higher than in the general population. In a study of specific psychiatric disorders and cognitive impairment among diabetics attending an out-patient clinic, 31% of the patients had psychiatric symptoms among which 4% were reported with mild depressive disorder. [12] But in the study of the psychological conditions of a cohort of Nigerian diabetic subjects at the University College Hospital, Ibadan, Nigeria, [13] the prevalence rate of depression for the entire cohort was reported to be 25.3% - a finding which shows that depression is a common feature of chronic debilitating illness. Depression among diabetics is associated with poor glycemic control, which is the principal cause of diabetic complications. [14] It is also found to be commoner among patients with less education, with lower social status [15] and successful treatment of depression among diabetes is associated with improvement in glycemic control. [16],[17],[18] The objectives of the study were:
Materials and Methods Site of study The study is part of a larger study conducted at the Medical Out Patient Department (MOPD) of the Jos University Teaching Hospital (JUTH) Jos. JUTH is a tertiary institution which takes care of patients with medical conditions including those with the diagnosis of DM. The out-patient department offers both secondary and tertiary health care services for patients referred from the General Out Patient Department, Surgical Out Patient Department, or other hospitals. Records from the MOPD of JUTH showed that there were about 350 registered patients with DM at the time of this study. Population The study commenced after receiving approval from the ethical committee of the hospital, and a sample size of 160 was obtained using the formula for sample size estimation by Araoye. [19] The study population consisted of patients who attended the diabetes clinic of JUTH between December 2005 and April 2006 with clinical evidence of DM, which was corroborated with the laboratory evidence as indicated by the fasting plasma glucose (FPG) concentration of th > 7.0 mmol/L or a casual glucose concentration of th > 11.1 mmol/L or a 2-hour postprandial glucose of th > 11.1 mmol/L after a 75 g glucose load. [19] Instruments The instruments consisted of the following:
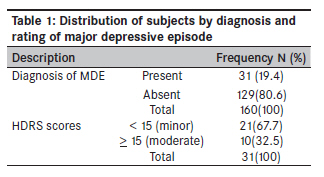
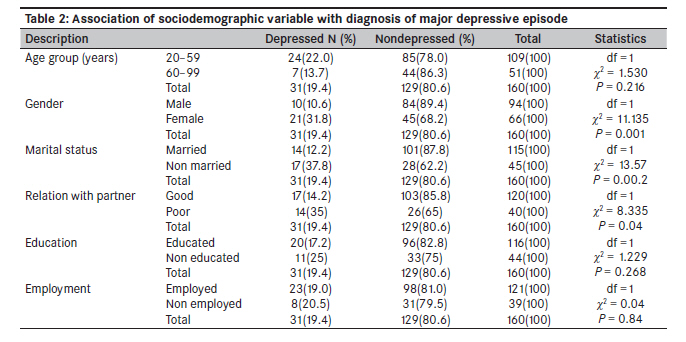
Procedure With the informed consent of each consecutive subject, the proforma for sociodemographic data was administered by the authors. Then psychiatrists trained in the administration of SCID conducted a structured interview on each subject. Those who met the diagnostic criteria of DSM--IV for a major depressive episode were subsequently interviewed with the Hamilton Depression Rating Scale to determine the severity of the depression at the time of the interview. This was done on every clinic day until the desired sample size of 160 patients was obtained. Subjects with alcohol and drug abuse, bipolar affective disorder, and those who had other comorbid medical conditions like pulmonary tuberculosis, HIV infection and hypertension were excluded. Data analysis The data were analyzed using the SPSS version 11.0 statistical package for windows. Mean and standard deviation were used to describe continuous variables and proportion for categorical data. The comparison of group means was done using student t-test, while the significance of observed difference in qualitative variables was determined by Chi-square tests. A P-value of < 0.05 was considered statistically significant. Results A total of 31 of the 160 diabetic subjects were identified as depressed using DSM-IV criteria giving a 1-year prevalence rate of 19.4%. Twenty-one (67.7%) of the 31 depressed subjects were rated as having minor depression and 10 (32.5%) as moderate to severe depression using HDRS. The mean age for the population studied was 53.49 + 11.36 years. Majority of the respondents were aged between 40-50 years representing 58.8% of the study population. The study population consisted of 66 (41.3%) females and 94 (58.8%) males. One hundred and fifteen (71.9%) of the subjects were married and 45 (28.1%) were not married and 120 (75%) of the respondents described their relationship with their partners as good, while 40 (25%) described their relationship as poor. Of the subjects studied, 116 (72.5%) were educated but 44 (27.5%) had no form of education. Also, 121 (75.0%) were employed at the time of the study while 39 (24.4%) were not employed. A statistically significant association was found between depression and gender status of the respondents (df=l, x2 =11.135, P=0.001), marital status (df=1, x2 =13.57, P=0.002), and the nature of relationship with sexual partners (df=1, x2 =8.335, P=0.04). There was no statistically significant difference between having the diagnosis of depression and the educational attainment of the respondents (df=1, x2 =1.229, P=0.268), employment status (df=1, x2 =0.04, P=0.84), and the respondents age groups (df=l, x2 =1.530, P=0.216) [Table - 1] and [Table - 2]. Discussion The study sample consisted of 160 patients and their ages ranged from 28 to 83 years. This is expected since young diabetic patients of less than 18 years are usually referred to the pediatric out-patient department of the hospital. Another possible explanation for the preponderance of adults in this study could be related to the fact that the most common form of diabetes is the type 2 with onset in adulthood. [20] The 19.4% 1-year prevalence of major depression in this study agrees with that in a systematic review of 20 studies by Gavard et al. [30] that shows the prevalence of depression among diabetic subjects to be within the range of 8.5-27.3%. It is, however, higher than the 4% prevalence of depression among diabetics reported by Coker et al. [12] in a study to assess psychiatric morbidity among diabetics at a Nigerian General Hospital but lower than the reported prevalence of 25.3% of depression among diabetics at the University College Hospital (UCH), Ibadan. [5] Since the SCID is used for the diagnosis of major depression, cases of mild and moderate depression were not accounted for. This would account for the disparity in the prevalence rate between this study and the one at Ibadan. This is an indication of the fact that depression is a common psychiatric morbidity among diabetics. At the time of the study, 67.7% of the depressed subjects had minor depression and 32.5% had moderate to severe depression based on the HDRS rating. This suggests that at the time of study, 67.7% had experienced an amelioration of their symptoms, which is explainable by the cyclical nature of depression. Depression in this study was significantly associated with the sex of the subjects studied with a male-to-female ratio of 1:3. This finding is similar to the general trend of gender distribution of depression in the general population. [31] It also concurs with that of Anderson et al. [10] who reported depression to be significantly higher in diabetic women (28%) than in diabetic men (18%). This could be attributable to gender-specific issues like menstrual cycle changes, pregnancy, miscarriage, postpartum period, premenopause, and menopause. [32] More so, many women also face additional stresses such as responsibilities both at work and at home, single parenthood, caring for children, and for aging parents, [33] which could all lead to depression. The study did not find any association between depression and age groups of the respondents, a finding which contrasts with that of Gregory and Jonathan, [34] who reported majority of the patients diagnosed with depression to be of younger age group. In this study, only adult diabetic patients were studied with 90% of the total subjects being 40 years and above. A larger sample size that includes younger patients is, therefore, necessary to generalize this finding. Depression in this study was significantly associated with the non-married group. The over representation of the non-married among the depressed suggests some relative protection offered by being married and is similar to that reported in a study in the United Kingdom, [35] where depression among diabetics was reported to be significantly related to the marital status of the subjects studied. This finding could be explained by the fact that married people are more likely to have a confidant whom they can share their problems with and who can give them the needed support when in a stressful situation like having a chronic illness such as diabetes. Depression in this study was also significantly associated with having a poor relationship with the respondents′ sexual partners. Marital discord, for example, is known to create problems and acts as a precipitant for depressive disorders; it may also perpetuate the disorder in patients who are already depressed. Additionally, persistent disharmony among sexual partners could influence negatively the emotional and physical conditions of both partners; this would account for the higher frequency of depression among subjects with poor relationship with their partners. Contrary to the findings in a study where lack of education was associated with the development of depression among diabetics by Engum et al., [36] this study could not find a significant association between educational status of the respondents and the diagnosis of depression. It is possible that most diabetics without education did not see the need of coming to a tertiary hospital for treatment, or would have died due to their low socioeconomic status. A community-based study may, therefore, be necessary to establish this association. This study has shown that depression is a common psychiatric disorder among diabetic patients in this environment. This underscores the need to screen such patients for depression to enable early detection and treatment, especially those at higher risk like females, the unmarried, and those who are experiencing marital problems. This would improve compliance to treatment, prevent the development of complications, and ultimately improve the quality of life of the patients. The major limitation of this study is the choice of the site of the study. JUTH is a tertiary health care facility and ideally with a very good filtering mechanism that allows mainly complicated cases reach the center; hence the sample cannot be representative of the general population. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10002t2.jpg] [am10002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}