 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
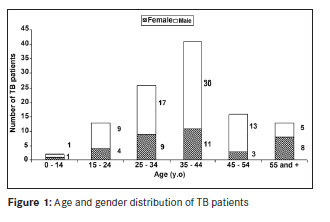
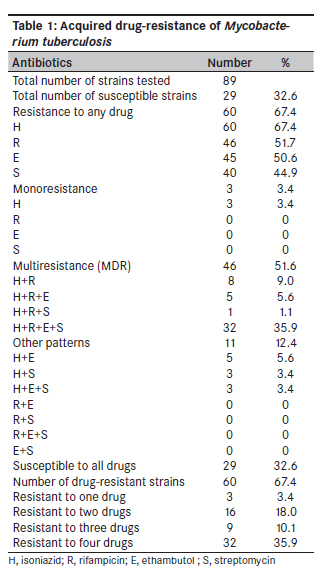
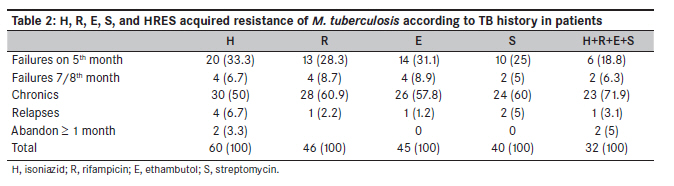
Annals of African Medicine, Vol. 9, No. 1, January-March, 2010, pp. 15-19 Original Article Mycobacterium tuberculosis drug-resistance in previously treated patients in Ouagadougou, Burkina Faso Sangare L, Diande S, Kouanda S, Dingtoumda BI, Mourfou A, Ouedraogo F, Sawadogo I, Nebie B, Gueye A, Sawadogo LT, Traore AS University Hospital Centre Yalgado Ouedraogo, 03 BP 7022 Ouagadougou 03; and Faculty of Health Sciences, University of Ouagadougou, 03 BP 7021 Ouagadougou 03 Code Number: am10004 PMID: 20418644 DOI: 10.4103/1596-3519.62619 Abstract Background: Tuberculosis drug-resistance becomes common in sub-Saharan Africa; however, very few data are available in Burkina Faso. The aim of this study is to assess the acquired resistance of Mycobacterium tuberculosis complex strains identified in TB patients to four first-line drugs in Ouagadougou.Methods: One hundred and ten (110) pulmonary tuberculosis patients with acid-fast bacilli-positive sputum and in situation of failure, relapse, or treatment abandonment were included in the study. Ninety six strains, including 92 (95.8%) M. tuberculosis and 4 (4.2%) M. africanum, were isolated from the sputum samples of these patients. Their drug susceptibility testing was performed using the proportion method. The first-line drugs tested were isoniazid (INH), streptomycin (STR), ethambutol (EMB), and rifampicin (RIF). Results: The overall drug-resistance rate of M. tuberculosis was 67.4% (n=60), including 3.4% to one drug, 18% to two, 10.1% to three, and 35.9% to four drugs. The resistance to INH, RIF, EMB, and STR were 67.4%, 51.7%, 50.6%, and 44.9%, respectively. Two strains of M. africanum were resistant to all drugs. Forty-six (51.7%) strains were multidrug-resistant (resistant to at least INH and RIF). Conclusions: In previously treated patients, the level of resistance of M. tuberculosis complex to commonly used anti-tuberculosis drugs is very high in Ouagadougou. Our results showed that multidrug-resistant tuberculosis could be a public health problem in Burkina Faso. Keywords: Burkina faso, drug resistance, Ouagadougou, tuberculosis Introduction The resurgence of tuberculosis (TB) is a major concern at the global level. The World Health Organization (WHO) estimates that 1.7 to 2 billion people are infected with Mycobacterium tuberculosis and that each year, 7-9 million develop TB of which 3 million die. [1] In Africa, TB prevalence remains high due mainly to the epidemic of HIV infection and the spread of multidrug-resistant (MDR) tuberculosis. [1],[2],[3],[4],[5] T he drug-susceptibility testing of M. tuberculosis remains a significant part of the monitoring process of the TB resistance to drugs. [6] Surveillance of drug-resistance, notably by periodic assessments, can guide the decision-maker in defining the standardized regimens and for assessing its quality on the field. Thus, the level and trend of resistance enables appropriate adjustments to be made either at the organizational level or changing the treatment regimens at patients′ level. In Africa, drug-susceptibility testing for M. tuberculosis is rarely done. Nevertheless, some useful information has been obtained in some countries in the course of investigations conducted by WHO and the International Union against Tuberculosis and Lung Disease (IUATLD), [7] or as part of studies done locally. [8],[9],[10],[11],[12] For the specific case of Burkina Faso, one study conducted at the Centre Muraz in Bobo-Dioulasso in 1996, a year after the adoption of directly observed treatment (DOT) in the country, showed an 8.6% overall prevalence of resistance to TB drugs in new cases. [13] Since then, no other study or evaluation has been conducted despite the fact that clinical treatment failures which suggest the existence of drug-resistant strains are recorded increasingly. Such a gap in information could complicate the implementation of any successful drug control program. The aim of this study was to assess the prevalence of M. tuberculosis resistance to antibiotics in patients experiencing failure, relapse, and treatment abandonment in order to assess the quality of treatment provided in Burkina Faso. Materials and Methods Setting The study was carried out in the laboratory of the National Tuberculosis Centre (NTC) in Ouagadougou, Burkina Faso. All bacteriological examinations were run in this laboratory where new TB cases are detected and where the bacteriological response to therapy of TB patients is monitored. It strongly supports the activities of the National Tuberculosis Programme (NTP). Patients and ethical consideration From April 2005 to February 2006, 110 patients experiencing failures, relapses, or treatment abandonment for at least 1 month and with acid fast bacilli (AFB) positive sputum smears were consecutively enrolled in a cross-sectional study. The aim of the study was explained to each participant in his language of communication. After obtaining informed consent, a standard questionnaire was completed for each patient to collect demographic data and the history of the disease such as: previous anti-TB treatment, treatment duration with or without injection (streptomycin), recognition of the anti-TB drugs on behalf of the patient, previous pulmonary radiographs and examinations of sputa. Bacteriological study Microscopic examination and strains isolation. Sputum smears were prepared and stained by the Ziehl-Neelsen hot method, as recommended by IUATLD. [14] One AFB-positive sample from each patient was used for the culture. The sputum samples were decontaminated with 4% NaOH, according to the Petroff method, [15],[16] centrifuged, and the sediments transferred onto Loewenstein-Jensen (LJ) media, LJ supplemented with pyruvate (LJ+pyruvate), and LJ containing 5 mg/L hydrazide of the thiophene-2-carboxylic acid (TCH) (LJ+TCH). These culture media were incubated at 37°C and observed on days 3 and 7 to detect contaminations and/or fast growth of atypical mycobacteria and subsequently every week to note the growth rate and the morphology of the colonies. Identification and drug-susceptibility test Isolates were identified by acid fast staining, colony growth time, resistance to TCH, culture abundance in LJ+pyruvate media, and activity to usual biochemical assays (niacin, nitrate reductase, catalase activity at 22°C and 70°C). [17] The antibiotics were tested according to the method of Canetti, Rist, and Grosset. [18] The concentrations used were 0.2 μg/mL for isoniazid (INH), 40 μg/mL for rifampicin (RIF), 4 μg/mL for streptomycin (STR), and 2 μg/mL for ethambutol (EMB). A strain was declared resistant to an antibiotic if the bacterial growth on medium with the drug was ≥1% compared to the control or sensitive when their growth was < 1%. Drug resistance was acquired if the patient was previously treated with antituberculosis drugs. A M. tuberculosis H37 ATCC 27294 strain was used for quality control in DST. Proficiency testing for culture and identification were done in collaboration with the National reference Center for Mycobacteria in Borstel (Parkallee Borstel Germany): 10 strains of M. tuberculosis Complex and 10 of atypical mycobacteria strains were used for this control. Statistical analysis The data were recorded and analyzed on SPSS version 12.0. The results were interpreted using standard chi-square test (χ2 ). A significant threshold was P<0.05. Results Demographic characteristics of patients One hundred and ten previously treated patients were included in the study, with 73 (66.5%) cases of failure, 25 (22.7%) relapses, and 12 (10.9%) cases of treatment abandonment at least for 1 month. The failures occurred at the fifth month in 24 (21.8%) patients, at 7/8th month in 7 (7.3%) patients, and in 41 (37.3%) failures after two courses of treatment (the chronics). The age and gender distributions are presented in [Figure - 1]. The sex ratio was 2.4, with 74 (67.3%) men and 36 (32.7%) women. The age range was 14-76 years old, with a mean of 38.3 11.4 years. Mycobacterium resistance to the drugs tested All the 110 patients were AFB-positive, while the culture was positive for 105 (95.5%), negative for 1 (0.9%), and contaminated for 4 (3.6%) patients. Among the 105 strains identified, there were 92 (87.6%) M. tuberculosis, 4 (3.8%) M. africanum, and 9 (8.6%) non-tuberculosis Mycobacterium which were excluded. Three isolates of M. tuberculosis were excluded because of insufficient number of colonies. Drug-susceptibility testing to INH, RIF, EMB, and STR was performed with 89 M. tuberculosis and 4 M. africanum strains. The results showed that 29 (32.6%) M. tuberculosis strains were sensitive to all antibiotics tested and 60 (67.4%) were resistant. Monodrug-resistance was 67.4% to INH, 51.6% to RIF, 44.9% to STR, and 50.5% to EMB. However, 32 (35.9%) strains were MDR for INH and RIF. The other resistance details are presented in [Table - 1]. Two of the four M. africanum isolates were resistant to all antibiotics tested. Resistance of M. tuberculosis to INH, RIF, EMB, and STR separately or combined was higher in chronic cases than among cases of relapse and treatment abandonment [Table - 2]. Chronic TB patients were more resistant to RIF and STR than those with failures at the 5th and 7/8th months (P=0.031 and 0.042, respectively) and also more resistant to any drug than the cases with relapse and abandonment of less than 1 month (P=0.0001). Discussion In this study and generally in sub-Saharan Africa, TB is more prevalent in patients aged 20 to 45 years, with a clear male prevalence. [19] In fact, young adults, and especially male adults, are the most economically productive and are committed in various activities from where the transmission of the tuberculosis bacillus can occur easily. [19] These reasons could also explain why there is more failure and relapse in this group. The prevalence of M. tuberculosis drug-resistance in this study was 67.4%. Lower rates have been described in Nepal, Italy, Estonia, [14] in Mexico, [20] and in Prague [21] (40.9%, 47.2%, 58.1%, 65%, and 52%, respectively). Higher rates were found in Egypt (68.2%), Russian Federation (73.3%), Kazakhstan (82.1%), [20] Ivory Coast (79.0%), [19] and Japan (80.0%). [22] The drug-resistance rate was higher in chronic cases (failure after two courses of treatment) than in other patients (failure after 5th or 7/8 th month and the relapses). It seems that the proportion of patients with resistant bacilli becomes dominant after failure of two treatment courses. It is probable that the provision of a second course of treatment as recommended by WHO will fail in the treatment of these chronic cases because when a strain is resistant to both INH and RIF, the chance of successful therapy is low. [23] The chronic cases could have been detected if the culture and drug susceptibility tests were performed after the failure of the first course of treatment. Unfortunately, in vitro surveillance of M. tuberculosis resistance to drugs is not effective in the country, despite the current need. Presently, a further study is ongoing to detect XDR tuberculosis in these strains. The MDR observed among patients in a situation of failure (particularly the chronics), relapse, and abandonment of treatment may reflect the quality of care or their poor compliance. This is an important public health problem considering the high level of resistance to drug used in the country. Monitoring of drug-resistant M. tuberculosis should be enhanced by periodic surveys to assess trends in resistance and take corrective action when necessary. Acknowledgments We express our gratitude to "Secure The Future" from BMS Foundation for the entire financial support. We thank Dr. Elvira Richter of National Reference Center for Mycobacteria (Parkallee Borstel Germany) for his comments, the health professionals at the CNLAT in Ouagadougou, and the laboratory of mycobacteria of the Centre Muraz in Bobo-Dioulasso for their technical assistance. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10004t2.jpg] [am10004t1.jpg] [am10004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}