 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
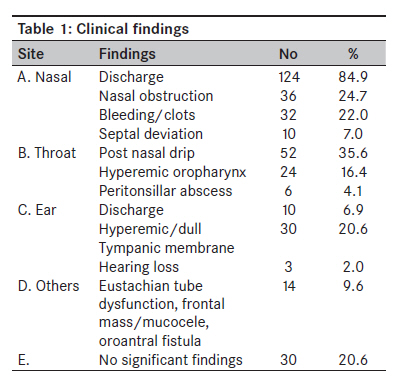
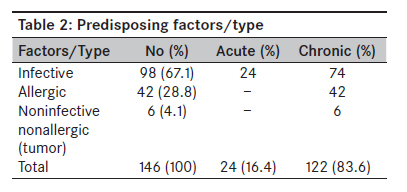
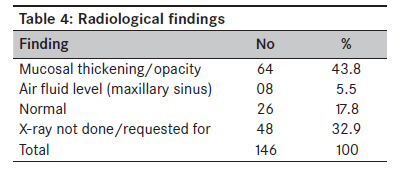
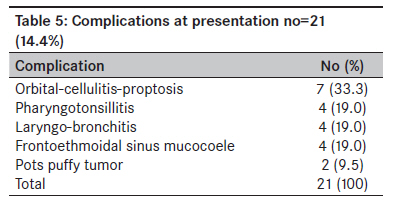
Annals of African Medicine, Vol. 9, No. 1, January-March, 2010, pp. 20-26 Original Article Rhinosinusitis: A retrospective analysis of clinical pattern and outcome in north western Nigeria Iseh KR, Makusidi M Department of ENT, Usmanu Danfodiyo University, Teaching Hospital, Sokoto Code Number: am10005 PMID: 20418645 DOI: 10.4103/1596-3519.62620 Abstract Background/Objectives: Rhinosinusitis is the commonest viral infection in man and the commonest inflammatory disorder encountered by general practitioners, chest physicians, and otorhinolaryngologists all over the world. The clinical pattern and outcome of conventional management measures were assessed.Method: All new patients with the diagnosis of rhinosinusitis over a 2-year period from July 1999 to July 2001 were analyzed for clinical features, conventional radiological findings, and treatment modalities over a period of 3 years follow up. Results: There were 195 (11.7%) new cases of rhinosinusitis out of a total number of 1661 patients seen over the period under review. Only 146 case notes were accessible for the study. Eighty-four (57.5%) were males and 62 (42.5%) were females. Their ages ranged from 7 months to 70 years. The main clinical symptoms and signs were nasal discharge or rhinorrhea (84.9%), nasal obstruction (24.7%), epistaxis (22.0%), and sneezing (20.6%). The duration of symptoms ranged from few days to about 10 years with 24 (16.4%) being acute cases while 122 (83.6%) were chronic cases giving a prevalence of 1.4% and 7.3%, respectively. Maxillary sinus (58.9%) was the commonest sinus involved. More than one sinus involvement accounted for 37.7% of the cases. Infective causes accounted for 67.1% of cases followed by allergy (28.8%). There were complications in 21 (14.4%) cases with orbital involvement (33.3%) being the commonest complication. Mode of treatment were medical (86.3%), and conventional surgery was carried out in 13.7% of the cases for either failed medical treatment or associated complications. Facial paraesthesia along the sites of surgery was the commonest complications, otherwise the outcome of treatment was excellent. Conclusion: Rhinosinusitis in this region was more of chronic (83.6%) variety than acute (16.4%) variety. Infective causes (67.1%) and allergy (28.8%) were the commonest etiological factors. About (86.3%) were amendable to medical treatment while surgical treatment was carried out in 13.7% of the cases. Rhinosinusitis should be managed medically first before recourse to surgical measures in carefully selected cases. Endoscopic sinonasal surgery is most desirable in keeping with current global trends of treatment of rhinosinusitis but where facilities do not exist, conventional surgical measures may be used. Keywords: North western Nigeria, pattern, rhinosinusitis Introduction Rhinosinusitis is an inflammatory process involving the mucosa of the nose and one or more sinuses. [1] The mucosa of the nose and the sinuses form a continuum and thus more often than not the mucous membranes of the sinuses are involved in diseases which are primarily caused by an inflammation of the nasal mucosa. [1] Acute viral rhinosinusitis often referred to as common cold is the commonest viral infection in man and the commonest inflammatory disorder encountered by general practitioners, chest physicians, and otorhinolaryngologists all over the world. [1],[2],[3],[4],[5] It is estimated that between 30% and 50% of all patients seen by the family practitioner suffer from some form of rhinosinusitis. [6],[7] It is the most commonly reported ailment constituting about 14% (30 million) cases in USA census department at an estimated cost of $5.78 billion per year. [1,8] An average young adult experiences about 2-5 attacks per year while in children, about 6-10 attacks are experienced per year with peak age group occurring between 3 and 6 years. [1],[5] Rhinosinusitis may be broadly considered under the following headings: allergic, infectious, and "other" or non-allergic non-infective. [6] A widely accepted set of classifications or definitions developed by the Rhinosinusitis Task force of the American Academy of Otolaryngology-Head and Neck Surgery which was reported by Lanza and Kennedy was based mainly on temporal time frames. [2],[3],[4],[5] These are acute rhinosinusitis (ARS) 7 days to ≤ 4 weeks, subacute rhinosinusitis (SRS) 4-12 weeks, recurrent acute rhinosinusitis (RARS) ≥ 4 episodes of ARS per year, chronic rhinosinusitis (CRS) ≥ 12 weeks, acute exacerbation of chronic rhinosinusitis (AECRS): sudden worsening of CRS with return to baseline. [2],[3],[4],[5] The European position paper on rhinosinusitis and nasal polyps in 2007 defined rhinosinusitis from three main areas namely (1) clinical definition, (2) definition for use in epidemiological studies/general practice, and (3) definitions for research. [1] For epidemiological studies, the definition is based on symptomatology without ENT examination or radiology. [1] ARS is defined as sudden onset of two or more symptoms, one of which should be either nasal blockade/obstruction/congestion or nasal discharge (anterior/posterior nasal drip) ± facial pain and pressure, ± reduction or loss of smell for < 12 weeks with symptom-free intervals if the problem is recurrent with validation by telephone or interview. [1] CRS is defined as the presence of two or more symptoms one of which should be either nasal blockade/obstruction/congestion or nasal discharge (anterior /posterior nasal drip) ± facial pain and pressure, ± reduction or loss of smell for < 12 weeks with validation by telephone or interview. [1] Rhinosinusitis could be diagnosed based on two major or one major and two minor symptoms. [2],[5] According to rhinosinusitis taskforce′s definition, major symptoms and signs include facial pain/pressure, facial congestion/fullness, nasal obstruction/blockade (continuous or intermittent), nasal discharge/purulence, hyposmia/anosmia, purulence on nasal examination, and fever (for ARS only). [2],[5] The minor symptoms and signs include headache, fever, halithosis, fatique, dental pain, cough, ear pain/pressure/fullness. [2],[5] Generally it must be noted that beside local symptoms stated above, there are distant and general symptoms. [1] Distant symptoms are pharyngeal, laryngeal, and tracheal irritation causing sore throat, dysphonia, and cough whereas general symptoms include drowsiness, malaise, and fever. Rhinosinusitis may be caused by genetic predispositions such as defects in mucocilliary clearance (Kartegener′s syndrome), increased viscosity of mucous (cystic fibrosis), or acquired from viral, bacterial, fungal, protozoal infection, allergy, chemical, gaseous septal deviation, neoplastic and physical trauma, or fractures. [1],[2],[3],[4],[5],[6],[7],[8] The underlying pathophysiology is the obstruction of sinus ostia drainage at the osteomeatal complex from inflammatory edema, impaired mucociliary clearance, followed by stasis of exudates and secondary bacterial infection. [1],[2],[3],[4],[5],[6],[7],[8] The clinical armamentarium available to the physicians guides the physician in establishing a diagnosis and institution of treatment measures. While this may be quite sophisticated in developed nations and the western world, particularly in imaging and endoscopy this may not always be so in nations with limited options for diagnostic and therapeutic interventions. The European position paper on rhinosinusitis and nasal polyps favored additional support from imaging but acknowledged that this certainly is not the case in many countries and has been reviewed. [1] Rhinosinusitis can be diagnosed based on clinical features and medical treatment instituted without complex diagnostic tests and investigations. Availability of good imaging and endoscopic techniques has added value to quality diagnosis and treatment options with comparison of findings, treatment measures, and results with other centers. In this study, the clinical presentations of rhinosinusitis and conventional management measures offered were carefully studied. Although facilities are limited in our region when compared to the western world, the diagnosis of rhinosinusitis was mainly clinical and patients with rhinosinusitis presented with various clinical scenarios with various therapeutic challenges in the region. It must be emphasized that availability of good imaging and endoscopic facilities in the region will improve the quality of diagnosis and treatment options in the region. This paper is the first of its kind from this region while similar studies have been carried out from other regions in the country. [9],[10],[11],[12],[13],[14],[15] Materials and Methods One hundred and ninety five (195) new cases of rhinosinusitis were seen between July 1999 and June 2001 at the ENT department of Usmanu Danfodiyo University Teaching Hospital Sokoto. Out of these, only 146 (74.9%) case notes or records were accessible for the study. The history, physical findings, relevant investigations, treatment measures, and outcome after a 3 year follow up were recorded. For the purpose of clarity of definition and comparison with other studies, acute rhinosinusitis in this study was defined as the presence of symptoms of rhinosinusitis for a duration of < 12 weeks while chronic rhinosinusitis was the presence of rhinosinusitis symptoms for a duration of> 12 weeks. Plain sinus x-rays were routinely ordered as computerized tomographic (CT) scan was not affordable by all patients. CT scan was a prerequisite prior to any surgical intervention but not necessarily mandatory. CT scan was also done in selected cases who presented with complications. All patients were commenced on medical treatment. Surgical treatment was carried out where medical treatment failed or when there was presence of complication. Absence of complete facilities for endoscopic sinus surgery coupled with unstable CT scan facilities limited the surgical measures to conventional methods combined with rigid endoscopy with 0 and 30° telescopes. New patients after commencement of medical treatment were seen in the outpatient clinic. Thereafter they were followed up on monthly basis on medical treatment until resolution of symptoms. Surgical cases after discharge from the ward were seen on weekly basis at outpatient clinic for nasal toileting sometimes aided by saline irrigation until the site of surgery was completely clear of crusts. At each visit, their overall well being was assessed subjectively by response to questions addressed toward the effectiveness of treatment such as "were they feeling better, worse, or no change to their condition pre- and post-treatment"? Were there any complaints arising from the treatment measures? Patients upon resolution of symptoms were discharged from follow up and were asked to call back whenever there was reoccurrence of symptoms. Results A total number of 1661 patients were seen over the period under review. One hundred and ninety five (11.7%) patients had rhinosinusitis of which only 146 case notes were obtained. Out of these, 84 (57.5%) were males and 62 (42.5%) were females with a male-to-female sex ratio of approximately 1.4:1. The age range was from 7 months to70 years, while the duration of symptoms ranged from few days to 10 years. Clinical features The clinical findings were classified mainly according to site as rhinological (nose), oropharyngeal/laryngobronchial (throat), and ontological (ear) as shown in [Table - 1]. Rhinological symptoms were more prominent as nasal discharge in 124 patients (84.9%), nasal obstruction 24.7%, and epistaxis (22.0%) and sneezing (20.6%). Other symptoms such as headache, excessive throat clearance, and hearing loss constituted 19.2%. Predisposing factors/type The duration of symptoms ranged from few days to about 10 years with 24 (16.4%) being acute cases, while122 (83.6%) were chronic cases giving a prevalence rate of 7.3% for CRS and 1.4% for ARS. Infective causes were 98 accounting for 67.1% of the cases, while allergy accounted for 28.8% of the cases and noninfective nonallergic (tumors) were responsible for 4.1% of the cases [Table - 2]. Sinus involvement The maxillary sinus (58.9%) was the commonest sinus involved as shown in [Table - 3]. There were 46 cases (28.8%) of inflammation of all the sinuses (pansinusitis) and more than one sinus but not all (multisinusitis) in 8.9% of the cases. Radiological findings By using conventional x-rays, significant mucosal thickening and opacity was detected in 64 cases (43.8%) as shown in [Table - 4]. Airfluid levels were detected in 5.5% of the patients, while in 26 cases (17.8%) the x-rays were normal and in 48 cases (32.9%) radiological investigation were not carried out. Complications Rhinosinusitis was complicated in 21 cases (14.4%) with orbital complications (33.3%) being the commonest as shown in [Table - 5]. Mode of treatment Rhinosinusitis in this region was amendable to medical treatment in 126 cases (86.3%). Surgery was carried out in 20 cases (13.7%), while 10 who were scheduled for surgery defaulted. Outcome of treatment There was overall improvement in 130 patients (89%) described as feeling better, while in 15 (10.3%) patients their response could not be ascertained. Patients on medical treatment who responded to treatment did not comply with regular check up for the 3-year period. Only 84 (66.7%) were followed up regularly for 3 months. Surgical patients were followed up a bit longer (range 4-6 months). Thereafter patients were seen irregularly for the 3-year period and some never bothered to come back upon resolution of symptoms. Discussion Rhinosinusitis is the commonest rhinological disorder and second commonest otorhinolaryngological disorder encountered in the otorhinolaryngological clinic of Usmanu Danfodiyo University teaching hospital Sokoto north western Nigeria. It constituted about 11.7% of the total number of otorhinolaryngological patients seen during the period of study. Rhinosiusitis in its many forms constitutes one of the commonest conditions encountered in medicine and may present to a wide range of clinicians from primary care to accident and emergency, pulmonologists, allergists, otorhinolaryngologists, and even intensivists and neurosurgeons when severe complications occur. [1] Males (57.5%) were affected more than females (42.5%) to the ratio of 1.4:1 and was characterized by the presence of more chronic variety (83.6%) than acute cases (16.4%) giving a prevalence rate of 7.3% for CRS and 1.4% for ARS. This is not surprising as inadequate treatment of acute cases may be responsible for the progression to the chronic variety or due largely to unidentified primary cause or predisposing factor. Chronic maxillary sinusitis is a common condition in otolaryngology practice from various regions in Nigeria. [9],[10],[11],[12],[13],[14],[15] Ogunleye et al. reported 93% cases of chronic sinusitis in Ibadan, south western Nigeria, while Sogebi et al. reported 75.6% cases of chronic rhinosinusitis in their study. [10,11] A comparative study in the north of Scotland and the Caribbean found that in otorhinolaryngology clinics in both populations, there was a prevalence of 9.6% and 9.3% of CRS, respectively. [1],[15] The incidence of acute viral rhinosinusitis (common cold) is very high. [1] It has been estimated that adults suffer two to five colds per year and school children may suffer seven to ten colds per year. [1],[6] Approximately 0.5-2% of viral upper respiratory tract infections are complicated by bacteria infection. [1] An average of 8.4% of the Dutch population reported at least one episode of ARS per year in 1999. [1] The infective type (67.1%) followed by allergy (28.8%) were the commonest clinical types in this study. Viral infection with added bacterial and, sometimes fungal infection, have been known to be infective causes of rhinosinusitis. A wide range of viruses, bacteria, and fungi with their various subtypes have been implicated in the etiopathogenesis of rhinosinusitis. Da lilly-Tariah reported 72.7% cases of chronic infective rhinosinusitis as the commonest type of rhinosinusitis in PortHarcourt South south region of Nigeria. [16] Allergy (28.8%) remains a significant cause after infective causes of chronic rhinosinusitis in this environment. Sogebi reported allergic rhinosinusitis (40.5%) as the commonest form of rhinosinusitis in Sagamu south western Nigeria followed by infective causes. Review articles on sinusitis have suggested that atopy predisposes to rhinosinusitis. [1] Mucosa in an individual with allergic rhinitis might be expected to be swollen and, therefore, more liable to obstruct sinus ostia, reduce ventilation, leading to mucus retention, which might be more prone to infection. [1] Savolainen studied the occurrence of allergy in 224 patients with verified ARS by means of an allergy questionnaire, skin testing, and nasal smears. [1],[17],[18] Allergy was found in 25% of the patients and considered probable in another 6.5%. [1],[19] Newman et al. reported that while 39% of patients with CRS had asthma, raised specific 1gE or an eosinophilia, only 25% had true markers to show they were atopic. [1],[19] Although rhinological symptoms predominate in rhinosinusitis, extra nasal symptoms and signs such as otitis media, pharyngotonsillitis, laryngobronchitis [Table - 1], etc. may be indicators of underlying rhinosinusitis disorder. The implication is that if the underlying pathology of rhinosinusitis is not treated, persistence of symptoms or recurrence of symptoms may occur despite medical or surgical treatment of the condition in question. The maxillary sinus (58.9%) was the commonest sinus involved in this study, while involvement of all the sinuses (pansinusitis) occurred in 46 cases (28.8%). The maxillary sinus remains the commonest sinus involvement in most studies. [1],[2],[9],[10],[11],[12],[13],[14],[15],[16] Pansinusitis occurring in 28.8% of the cases is almost similar to the number of cases reported by Ogunleye et al. who recorded 29% of pansinusitis in their study. [10] In this study, plain x-rays were used to assess the level of sinus involvement. Significant mucosal thickening and opacity were detected in 64 cases (43.8%), airfluid level in 8 cases (5.5%), normal findings in 26 cases (17.8%), while in 48 cases (32.9%) x-rays were not ordered for. Plain sinus x-rays are insensitive and of limited usefulness for the diagnosis of rhinosinustis due to the number of false positive and negative results. [1] Ezeanolue et al. in their study based on specificity and positive predictive value concluded that plain x-rays showing antral air fluid level and opacity were highly predictable of maxillary sinusitis with retained secretions. [9] Plain x-rays are inferior in quality and not very accurate in diagnosis of rhinosinusitis when compared to CT scan or MRI. Details of the sinus pathology are better shown with the CT scan such as the extent of sinus involvement, the underlying pathology at osteomeatal complex, the infundibulum, agar nasi cells, frontal recess, and associated orbital and intracranial complications. CT findings should be interpreted with caution as apparently symptom-free individuals have been shown to have abnormal CT findings. MRI is not the primary imaging modality in rhinosinusitis but is usually reserved in combination with CT for the purpose of more serious conditions such as neoplasia. [1] Inadequate radiological diagnosis is bound to lead to inadequate approach to treatment and propensity to recurrence of rhinosinusitis with attendant complications and inadequate management of complications. Medical treatment of rhinosinusitis proved to be beneficial in 126 cases (86.3%), while surgery was carried out in 20 cases (13.7%). Standard conservative treatment for rhinosinusitis is based on short- or long-term antibiotics and topical steroids with the addition of decongestants mostly in a short-term regime and for the acute attack itself. [1] Many other types of preparation have been investigated but substantial evidence for their benefit is poor. [1] These medications include antral washings, isotonic/hypertonic saline as nasal douche, antihistamine, antimycotics, mucolytic agents/phytomedical preparations, immunomodulators/immunostimulants, and bacterial lysate preparations. [1] For selected patients with CRS, and gastrointestinal reflux, the impact of antireflux treatment on sinus symptom scores has been studied. [1] Rhinosinusitis was complicated in 21 cases (14.4%) in this study [Table - 5] with Orbital (33.3%) involvement as the commonest complication followed by frontoethmoidal mucoceles (19.4%), pharyngotonsilitis (19.4%), and laryngobronchitis (19.4%). There were no intracranial complications in this study. Ogunleye et al. reported 33 cases (37%) of complications of sinusitis with orbital complications constituting 41% followed by sinus wall (32%). [14],[20] Iseh et al. reported that chronic rhinsinusitis was the underlying predisposing factor in all the cases of paranasal sinus mucoceles reported. [21] If sinus infection is untreated or inadequately treated, complications can develop. Complications of rhinosinusitis are classically defined as orbital, osseous, and endocranial though rarely some unusual complications can develop such as lacrimal gland abscess, nasal septal perforation, visual field loss, mococoele or mucopyocele, displacement of the globe, and septicemia. [22],[23],[24],[25],[26] In 130 patients (89%) in this study, there was general improvement described as the absence of symptoms and feeling better, while in 15 patients (10.3%) their response could not be ascertained. Several studies have been carried out to evaluate patients′ response to treatment and their quality of life. [1],[2],[3],[4],[5],[6],[7],[8] Such evaluations are necessary to compare the outcome of various treatment protocols, and also compare with other studies. In conclusion, rhinosinusitis in north western Nigeria was characterized by the presence of more chronic infective variety, followed by allergy. Medical treatment proved to be beneficial, while surgery was reserved for selected cases of either failed medical treatment or complications. Although the response to treatment was excellent in 89% of cases, availability and affordability of modern imaging and endoscopic techniques will certainly improve both diagnostic and therapeutic measures. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10005t5.jpg] [am10005t1.jpg] [am10005t2.jpg] [am10005t4.jpg] [am10005t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}