 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
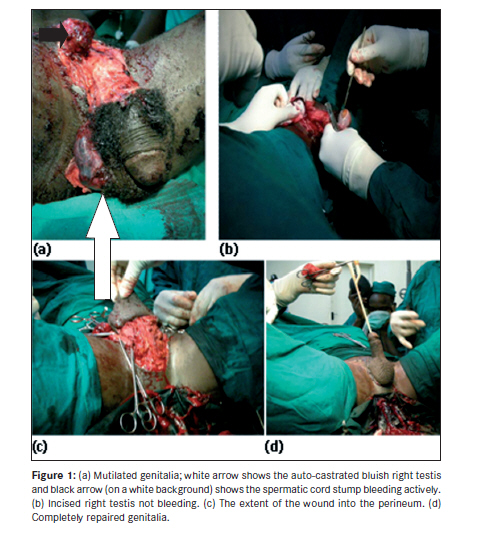
Annals of African Medicine, Vol. 9, No. 1, January-March, 2010, pp. 31-34 Case Report Genital self-mutilation Ajape AA, Issa BA, Buhari O. I. N., Adeoye PO, Babata AL, Abiola OO Division of Urology, University of Ilorin Teaching Hospital, Ilorin Code Number: am10007 PMID: 20418647 DOI: 10.4103/1596-3519.62622 Abstract We present a case report of a 22-year-old Nigerian student who presented to the accident and emergency unit of a Nigerian Teaching Hospital with a history of self-inflicted genital injury following a suicide attempt. He had background history of predisposition to depressive illness, a current diagnosis of a major depressive disorder, and had had two attempted suicidal episodes in the last 3 months prior to this event. The clinical finding shows a patient with sad affect, feeling of hopelessness, and worthlessness; however, the vital signs remained fairly stable. At examination under anesthesia, the testes were exposed and the right already self-castrated. The penis was degloved to the level of the Buck's fascia with intact corpora cavernosa and urethra. He had surgical excision of the hanging self-castrated right testis with debridement and primary closure of the genital laceration. He was promptly reviewed by the psychiatrists who comanaged appropriately.Keywords: Auto-castration, depressive illness, genital self-mutilation Introduction Genital self-mutilation (GSM) is a rare phenomenon with a little over hundred cases identified in the literature. [1] The desire for self-mutilation of the genitalia, in the absence of any discernible psychopathology, is even rarer. [2] Male GSM was recorded in the Greek mythology; the beautiful god Eshmun castrated himself to evade the erotic advances of the goddess Astronae, and auto-castration came to be known as the Eshmun complex. [3],[4] The first reported case of GSM in the English literature was by Strock in 1901. [4] Although , the act was considered unknown in Africa, [4] a few cases have been reported from Kenya and Nigeria. [5],[6] Self-inflicted genital injuries range from simple laceration of the external genitalia to more complex injuries, which include complete penile amputation, self-castration, or combination of both. [1] GSM injury presents a major challenge to both urologist and psychiatrist in its management. This case report illustrates a variant of such injuries in a black African patient. Case Report A 22-year-old single, Nigerian young man of African origin. He is from a polygamous family and first child of his mother who had five children. He was referred from a General Hospital about 100 km from our facility and presented about 4 hours following injury. He was brought to the accident and emergency unit with a history of self-inflicted perineal injury following a suicide attempt. He was in painful distress, anxious, and had a perineal wound that was bleeding actively. This had been packed with gauze. He had a background history suggestive of depressive illness, which dated back to about 3 years when he was withdrawn from his desired course of study in the University due to poor academic performances. Thence, he had to join another course. He had some financial difficulties in the recent time which resulted in him being sad, with loss of interest in usually pleasurable activities and felt life was worthless. There were two unreported attempted suicidal episodes within 3 months prior to this event. Otherwise, there was no history suggestive of psychotic illness. There was no history of drug or alcohol abuse. His academic performance had been slightly below average even though he was in the final year of his study. On arrival at the emergency unit, he was conscious, alert, but in painful distress. He had good concentration and attention but the mood was low with a sad affect, feeling of worthlessness, and hopelessness. There was no thought alienation or perceptual disturbances. Death was the motive behind the act, although he had not written any note and he did not make efforts to prevent himself from being discovered. The pulse rate was 100/min and blood pressure of 100/60 mmHg. The result of serum urea, electrolyte, and creatinine estimation were within normal limits. The packed cell volume was 33% and blood was taken for grouping and cross-match. His consent was taken for examination under anesthesia (EUA), and repair/reconstruction. Findings under anesthesia included a circumferential skin laceration extending, apparently, from the left dorsolateral part of the base of penis through the ventral aspect and perineum to the right of suprapubic region and involving the scrotum [[Figure - 1]a and c]. Both testes were exposed. The right spermatic cord was severed with the proximal part retracting under the inguinal canal [[Figure - 1]a, black arrow] leaving the right testis hanging, bluish, and non-viable [[Figure - 1]a, white arrow and 1b]. The skin laceration was deep to the Buck′s fascia and exposed the dorsal penile neurovascular bundle and the intact tunica albuginea covering the corporal tissue [Figure - 1]a. There was no clinical evidence of urethral injury. At repair, the wound was extended proximally in an oblique direction into the right inguinal region to secure proximal vascular control of the spermatic cord. The hanging, self-castrated right testis was excised and non-viable tissue was debrided. Hemostasis was adequately secured. The genital wound was repaired in layers. A size 16FR Foley urethral catheter was passed into the bladder with ease and left in place for 12 days. He had adequate analgesia, antibiotics, and tetanus prophylaxis. He developed superficial wound infection on the right lateral side of the wound, which was treated by Sitz′s bath and wound dressing. The infection cleared and the wound healed within 2 weeks of admission. The patient was seen and evaluated by the psychiatric team on day 2 of admission and a diagnosis of moderate to severe depression with suicide attempt was made. He was placed on amitriptyline, which, because of troublesome side effects, was changed to fluoxetine later. The mental state improved significantly without detectable psychopathology over the 2 weeks of admission. He was discharged on antidepressant and he was doing well as at last follow-up clinic visit. Discussion GSM is a rare phenomenon. There appears to be an increasing incidence but whether this is due to increased level of reporting in recent years remains unclear. [1] Although the act was considered unknown in Africa, all racial groups, cultures, and religions are involved making it a global malady. [4] The vast majority of reported incidents occurred among single, White male in the age range of 20s and 30s. [1] Our patient fell within these categories except for being of African descent. The first major literature review on GSM was published in 1979 [7] ; so far about 123 cases, involving both sexes, are identified in the English literature. [1],[4],[5],[6],[8],[9],[10] The degree of mutilation, the predisposing factors, and the instruments used in the perpetration of this irrational, dastardly, act varies. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10] The instruments included kitchen knives (as used in this case report), blades, scissors, chainsaw, and an axe. Injuries sustained range from simple lacerations of the scrotal skin to complete penile amputation, scrotal and testicular loss. The index case sustained significant scrotal and penile skin laceration with self-castration of the right testis. This could actually worsen the depressive state of such patients especially if both testes were castrated resulting in infertility. The motivational factor responsible for GSM varies. About one-tenth of self-mutilators intended suicide, [8] as found in this case. GSM has been categorized as belonging to three diagnostic subgroups: schizophrenic patients, transvestites, and those with complex religious and cultural beliefs. [1] Although our patient seems not to fit into any of these categories, the act of GSM and self-castration has been reported as the first sign of incipient schizophrenia. Thus there is need for close follow-up of this patient to detect any overt psychotic tendency in future. It is indeed suggested that in the absence of overt psychotic symptoms, self-castration should be considered to be a presenting sign of schizophrenia. [11],[12] With the exception of the two episodes of attempted suicide, organic psychosis, drug, or alcohol abuses are not likely to have played a significant role in this patient as history refuted these factors. However, affective disorders (depression and mania) have been implicated as causes of GSM. [4] Depressive illness seemed to be the predisposing factor in our patient. In addition, pathological guilt associated with sexual conflicts or sexual transgression, [1],[4] prevention of alopecia, [13] and grief [14] are other documented precipitating factors. The influence of religion in GSM dates back to the early Roman times and the eponym ′Klingsor syndrome′ has been coined to denote GSM resulting from religious delution. [1],[11] It was derived from a character from Wagner′s opera ′Parsifol′ who self-castrated in an attempt to gain entrance into the brotherhood of the Knights of the Holy Grail. It is, however, believed that the etiopathogenesis, the course, and the prognosis of GSM resulting from psychotic illness and religious delusions are similar. Thus the term Klingsor syndrome should encompass both the forms of GSM. [15] As the degree of mutilation varies so does the treatment; it could be complex and quite challenging. It is often a multidisciplinary responsibility, usually between the urologist, psychiatrist, psychologist, and the primary care physicians as it was done in this case report. The ultimate goal of surgical treatment includes restoration of anatomy and function as much as possible. A superficial laceration may require no more than simple suturing. Amputation of the penis would require primary anastomosis if the distal segment is available with cold-ischemic time of less than 16 hours. [1] Some researchers have attempted anastomosis even when the cold-ischemic time is greater than 16 hours with less favorable result. [16] The development of microvascular technique has improved success with regard to penile reimplantation. This facility was quite handy in the present case report as a vascular surgeon was in attendance for possible vascular anastomosis, the need for which did not arise. Complications resulting from GSM varied according to the severity of the injury inflicted and the extent of surgical repair undertaken. [1] Reported complications include erectile dysfunction, urethral stricture, urinary fistula formation, and sloughing of the distal urethra and penile skin. A significant proportion will repeat the act, die of excessive hemorrhage, or succumb to the suicide by completing it. [8] Numerous reviews [4],[8],[9],[10] and individual case reports have highlighted the inconsistencies that exist in this subgroup of patients and the myriad of motivational factors behind this unique form of deliberate self-harm. The identification of those at risk remains as difficult as ever. Even more challenging is identifying those patients at risk of repeating this act and those that will go on to complete the suicide intent. Conclusion Whether affective or psychotic, GSM is irrational; the characteristics of the perpetrators and their act vary. [ 4] While the aim at presentation remained the timely management of hemorrhage and urological injuries, a detailed psychiatric evaluation and treatment should start in earnest to reduce the incidence of repetition of the act and completion of the suicidal act. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10007f1.jpg] |
| |||||||||

{kind=link}