 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
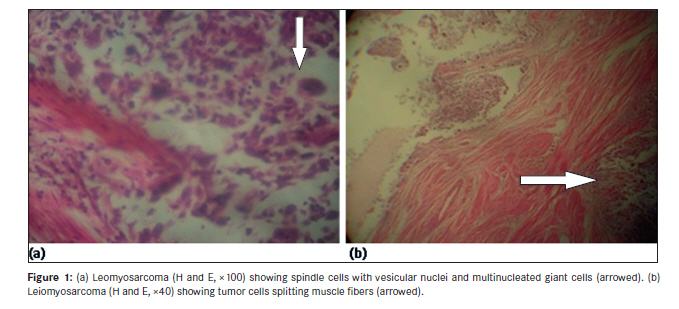
Annals of African Medicine, Vol. 9, No. 1, January-March, 2010, pp. 35-38 Case Report Leiomyosarcoma uteri in a white woman Adesiyun AG, Samaila M. O. A. Departments of Obstetrics and Gynaecology, Ahmadu Bello University Teaching Hospital, Shika, Zaria, Kaduna State Code Number: am10008 PMID: 20418648 DOI: 10.4103/1596-3519.62623 Abstract Sacroma of the corpus uteri should be considered as a differential diagnosis in postmenopausal women presenting with severe abdominal pain, thought to be due to degenerative changes of leiomyoma uteri. We present a rare case of leiomyosacroma in a postmenopausal White woman. Diagnosis was missed preoperatively for degenerating uterine fibroid.Keywords: Incidental, leiomyomasacroma, surgery Introduction Leiomyosarcoma is one of the three most common histological variants of uterine sarcoma. [1] Others are endometrial stromal sarcoma and malignant mixed mullerian tumors. A high index of suspicion is needed in the diagnosis of this rare but highly fatal tumor. We report a 55-year-old White woman of Ukrainian decent who had laparotomy based on a presumed diagnosis of uterine leiomyoma with degenerating changes. However at surgery, she was found to have a uterine malignancy and this was confirmed to be leiomyosarcoma after pathologic examination. Case Report A 55-year-old para 1+0 White woman was referred with intractable lower abdominal pain of 4 months duration. There was associated abdominal swelling and postmenopausal vaginal bleeding. Her last childbirth was 24 years ago. Her past medical history revealed no significant illness. There was no history of exposure to radiation. She is sexually active. The family history and review of system were unremarkable. On examination, she appeared ill. Her temperature was 38.7 o C, blood pressure 125/80 mmHg, and heart sounds were normal. There was no abnormal finding detected in the chest. Examination of the abdomen revealed a tender uterus consistent with 20 weeks pregnancy size. The liver, spleen, and kidneys were not palpably enlarged. There was no evidence of ascites. Pelvic examination showed a grossly normal cervix. A clinical diagnosis of uterine fibroid with degeneration was made. The patient′s hemoglobin was 7.5 g/dl and white blood cell count was 13.8 Χ 109 /l. Urine analysis was normal; however urine culture yielded E. coli growth. Transabdominal ultrasound examination revealed an enlarged globular uterus with transverse diameter of 14.3 cm, the uterine cavity was empty, endometrium was thin, the myometrium contained multiple circumscribed heterogeneous masses and the largest measured 7.1 cm, and the ovaries were hypoplastic. An ultrasound diagnosis of multiple uterine fibroids was made. The patient had transfusion with two units of cross-matched blood. She was also placed on analgesia, antimalaria, and intravenous antibiotics (ceftriaxone and metronidazole). She was taken for surgery 72 hours after stabilization treatment. At laparotomy, the enlarged uterus was delivered from the abdominal cavity. A ruptured lesion on the right anterolateral aspect of the uterus measuring 7 Χ 6 cm was seen; it egressed discrete tissue up to 35 ml. The lesion was hitherto walled by contact with the overlying parietal peritoneum. There was significant induration and matting together of the structures to the right side of the uterus. The ovaries looked grossly normal and there was no enlarged aortic/ paraaortic lymph nodes. She had total abdominal hysterectomy and bilateral salpingo-ophorectomy. Postoperative recovery was uneventful. A globular total abdominal hysterectomy and bilateral salpingo-oophorectomy specimen that measured 16 Χ 15 Χ 11 cm and weighed 1225 g was sent to the pathologist. Area of spontaneous rupture of the myometrial wall was noted on the right side of the uterus. Cut surface showed a necrotic tumor with solid grey and yellow areas, fairly circumscribed compressing an intact endometrial cavity. Microdescription shows necrotic tumor composed of spindle cells having oval to elongated nuclei, prominent nucleoli, and moderate amount of eosinophilic cytoplasm. Many bizarre osteoclast-like giant cells and mitotic figures are noted [Figure - 1]a. There were features of vascular invasion. Tumors cells splitting muscle fibers were also noted [Figure - 1]b. Histological diagnosis of leiomyoscaroma uteri was made. The patient was referred with stage III uterine leiomyosacroma to the oncologist for radiochemotheraphy. Discussion Leiomyosarcoma uteri is a highly malignant neoplasm. [1] Of all the types of uterine sarcoma, leiomyosarcoma is the most common pure form, accounting for about 1% of all uterine malignancies. [2] Reported incidence of leiomyosarcoma is in the range of 0.3-0.4 per 100,000 women per year. [2] The age of the patient reported falls in the bracket of quoted median age of patients with LMS 50-55 years. [3],[4] The patient reported had no significant medical history apart from long-standing history of infertility; risk factors for endometrial cancer like nulliparity, obesity, diabetes mellitus, and hypertension do not apply to cases of leiomyosarcoma. [5] History of exposure to pelvic irradiation was reported in 4% of leiomyosarcoma cases. [6] The patient reported had no history of exposure to irradiation. As was the case in this patient, in a series abnormal vaginal bleeding was the most common symptom, followed by the presence of a pelvic mass and abdominopelvic pain. [7] Leiomyosacroma is known to exhibit similar symptoms to leiomyoma; however suspicion should be high in patients presenting with rapid increase in uterine size after menopause, severe abdominal pain, and irregular vaginal bleeding. [5] Although this patient had presumptive diagnosis of leiomyoma, leiomyosarcoma uteri are usually not associated with leiomyoma. The incidence of sacromatous changes in leiomyoma is between 0.13% and 0.81%. [6] Endometrial biopsy done in the pre-operative evaluation of the patient was not helpful. Authors have, however, reported infrequent diagnosis of leiomyosarcoma on endometrial sampling. [6],[8] Intraoperatively, there was no palpably enlarged para-aortic or aortic lymph node in this patient. Studies have reported low lymph node metestasis in cases of leiomyosarcoma. The need to evaluate lymph nodes remains controversial. [6],[8] Authors have suggested that evaluation of lymph node is important if lymph nodes were clinically suggestive or if there was presence of intra-abdominal disease. [9],[10] This patient had total abdominal hysterectomy and bilateral salpingo-ophorectomy. There is controversy on the fate of the ovaries in premenopausal patients with leiomyosarcoma. Studies have come out with beneficial effect of ovarian preservation on treatment outcome, [11],[12] while other studies found no significant difference in disease-specific survival. [13],[14] Although with no consensus, several prognostic indicators like premenopausal state, stage of disease, and mitotic index have been mentioned in the literature. [3],[4],[14] Several studies have reported better outcome in premenopausal women, [14],[15] while other experiences from other studies did not confirm this. [16],[17] On the balance stage of the disease is an important prognostic indicator. For tumor confined to the corpus uteri, the size of the neoplasm with best demarcation at 5 cm have been reported as an important prognostic factor. [18],[19] Mitotic index have been reported to be of prognostic significance [3],[4],[14] but other studies did not found it useful. [20] African American women have a higher incidence and poor prognosis. [6] The patient reported was an European resident in Nigeria for an upward of 20 years. The patient was referred to the oncologist with stage III disease. While adjuvant pelvic irradiation decreases the rate of local recurrence, it does not appear to significantly improve survival. [7],[21] Chemotherapeutic regimen containing doxorubicin is believed to have the best activity against uterine leiomyosarcoma. [22],[23] Piver demonstrated a low occurrence rate in patients with stage I leiomyosarcoma of the uterus [24] but on the contrary, Omura did not find a statistically significant difference in the recurrence rate. [25] In resource-poor setting where accessibility to modern diagnostic method is limited, conscious effort should be directed at ruling out uterine sarcoma in all patients with presumptive diagnosis of leiomyoma, [26] more especially if they are postmenopausal. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10008f1.jpg] |
| |||||||||

{kind=link}