 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
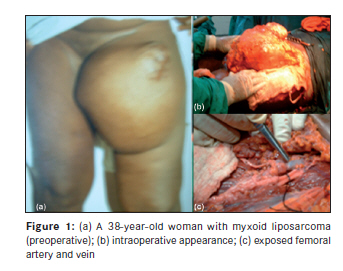
Annals of African Medicine, Vol. 9, No. 1, January-March, 2010, pp. 39-43 Case Report Soft tissue sarcoma of the thigh: Need for angiography in the developing countries Ismaila Abiona Adigun, Ganiyu Adebisi Rahman, Kolawole Olubunmi Ogundipe Division of Plastic and Reconstructive Surgery, University of Ilorin Teaching Hospital, Ilorin Code Number: am10009 PMID: 20418649 DOI: 10.4103/1596-3519.62624 Abstract Background: Soft tissue sarcomes (STS) are relatively rare tumors that are seldom seen in many surgical practices. In the developing countries, most patients present lately to the tertiary center either because of poverty, ignorance, or poor management by the primary health workers that first come into contact with these patients.Methods: We bring you five patients with large STS thighs that were managed by unity between the years 2005 and 2007. Results: Three of these patients are deceased, and one of the two surviving patients has amputation below the knee. The two surviving patients lost view after 3 months. Conclusion: Although angiography has been relegated to the background by the advent of modern techniques such as tomography imaging by computer (CT) and imaging by magnetic mirroring (IRM), in the developing countries angiography remains important as one prι-opιratoire of surgical guide in the thigh STS. Keywords: Angiography, sarcoma Introduction Soft tissues are the extra-skeletal tissues of the body that support, connect, and surround other discrete anatomic structures. These tissues contribute more than 50% of the body weight and include muscles and tendons as well as fibrous, adipose, and synovial tissues. Soft tissue sarcomas (STS) are relatively uncommon tumors that are infrequently seen in most surgical practice, accounting for 0.7% of adult malignancies but up to 15% of childhood malignancies. [1] Lipomas are the most common benign neoplasm and usually present no diagnostic or therapeutic difficulties. Sarcomas, however, rarely develop from pre-existing benign soft tissue tumors. [2],[3] It is estimated that there are 100 benign lesions for each sarcoma. [4] The American Cancer Society estimates that in 2004, approximately 8,680 new STSs will be diagnosed in the United States, and 3,660 deaths from STS are predicted accurately from 0.63% of all cases and 1.15% of deaths from cancer. [5],[6] In Nigeria, there is paucity of information on STS, with a few reports from Ibadan, Calabar, Lagos, Zaria, Port-Harcourt, and Ilorin. [7] STS can occur in any anatomic region of the body because of the ubiquitous nature of connective tissue, but most sarcomas (60%) develop in the extremities, more commonly in the legs than in the arms. The common clinical presentation is an enlarging painless soft tissue mass in the thigh, typically 5-10 cm in diameter. Two-third of the tumors are intramuscular. [8] When there is pain, it is usually very mild and occurs later in the course of the disease. Thus a patient might delay seeking medical attention, and a definitive diagnosis also might be delayed. [9] In the developing countries, most patients present lately to the tertiary center either because of poverty, ignorance, or poor management by the primary health workers that first come into contact with these patients. We present five patients with large STS of the thighs. Even though angiography has been relegated to the background by the advent of modern imaging techniques such as computerized tomography (CT) and magnetic resonance imaging (MRI), these new imaging techniques are not readily available in most centers in the developing countries and when they are available, they are mostly unaffordable to most patients. Angiography that has been largely outdated by the aforementioned investigation thus remains a valid tool in investigating the involvement or otherwise of the vessels. We suggest that all patients with STS of the thigh should have vascular angiography done before surgical excision of the tumor based on our experience in the management of cases presented. Case Reports Case 1 A 23-year-old barber was referred from the General Outpatient Unit of Ilorin University Teaching Hospital with a history of multiple swellings all over the body of 6 years duration and progressively enlarging swelling of the right thigh of 1 year duration. He had noticed development of nodular swellings over his body about 6 years before presentation. The nodules were painless with no associated pruritus but increasing in number. One of the swellings on the right thigh began to increase in size about 1 year before presentation. There was no associated hearing or visual loss. He was the 8th child of the parents. There was no family history of similar lesion and no evidence of mental retardation. Examination revealed a young man with multiple cutaneous nodules of various sizes spread all over the body with multiple cafι-au-lait spots and left inguinal freckling. Swelling on the anterior-medial aspect of the upper third of the thigh measured 15 Χ 10 cm in size; an assessment of neurofibromatosis with malignant transformation was made. Patient defaulted and represented after 3 months. At this time, the mass measured 30 Χ 24 cm in size. Chest x-ray showed multiple cannon-ball metastatic lesions in both lung fields. He had a wide surgical excision of the tumor. Intraoperatively there was no neural or vascular invasion. The tumor was superficial to the femoral vessels. After 10 days, another mass recurred from the surface of the wound, his clinical condition deteriorated, and he died 1 week later. The histopathology result of the excised mass confirmed neurofibrosarcoma. Case 2 A 38-year-old woman was referred to the Surgical Outpatient department from the General Outpatient department with a 3-year history of soft tissue swelling in the left thigh. The mass was painless but increasing in size gradually. There was no associated weight loss, she is a known hypertensive patient, and was on medication. Examination revealed a large mass in the upper part of the left thigh with irregular edges, firm in consistency, and no clinically palpable lymphadenopathy. X-ray of the left thigh showed evidence of calcification within the mass and a thickening of the medial cortex of the femur. Chest x-ray did not show evidence of pulmonary metastases. Angiography was not requested for. Patient was prepared for an excisional surgery. Intra-operatively, there was entrapment of the superficial femoral vessels and the femoral artery and veins within the tumor. The femoral artery and veins were transected during the course of dissection [Figure - 1] a-c. The transected vessels were repaired. The period of ischemia was between 10 a.m. to 8 p.m. (10 hours). When the vascular clamps were released to establish circulation to the affected limb, patient had cardiac arrest. Cardioplumonary resuscitation was started; she was given intravenous adrenaline and sodium bicarbonate all to no avail. She was certified dead from probable reperfusion ischemic injury. Histopathology result confirmed myxoid liposarcoma Case 3 A 40-year-old woman noticed a swelling on her left thigh 2 years prior to presentation. The swelling was not painful but progressively increasing in size. She has had excision of the mass twice, 15 years and 6 years ago after recurrence, but no histopathological study of the specimens removed. Examination revealed a mass measuring 36 Χ 26 cm, multilobulated, occupying the anteriomedial and posterior aspects of the left thigh extending from the knee joint to within 5 cm of the thigh crease. A 4 Χ 4 cm fungating ulcer was on the medial aspect of the mass. Plain x-ray of the left thigh showed no bony involvement and chest x-ray did not reveal evidence of metastases. Abdominopelvic ultrasound did not show any abnormality. CT angiography revealed extensive entrapment of the superficial femoral vessels; the circumflex vessels were not clearly outlined. She had an angiographic guided excision of the tumor done with split thickness skin grafting of the bed. Two weeks postoperatively, she developed gangrene of the left foot and lower leg. She probably developed deep vein thrombus. She had a below knee amputation done and was discharged home on crutches. Case 4 A 32-year-old man was referred from a private hospital on account of a right groin mass. The mass started as a painless nodule about 3 years prior to presentation; it was slowly increasing in size until the mass got ulcerated. There was history of weight loss despite good appetite. Examination revealed a fungating tumor approximately 12 Χ 8 cm in size with serosangunious discharge and no significant peripheral lymphadenopathy. Plain x-ray did not show any evidence of bony involvement. Chest x-ray did not show pulmonary metastases. CT angiography showed that the mass was clearly separated from the femoral vessels. The external iliac arteries and veins were also normal bilaterally. No remarkable abnormal vascular supply to the mass was seen. He had a wide excision of the mass with a split thickness skin grafting of the bed. Histopathology result showed that the tumor was leiomyosarcoma. This result was highly questionable. The histopathology slide was then reviewed both by the surgical team and the pathologists; the tumor was highly suspicious of leiomyosarcoma. Case 5 A 16-year-old boy presented with a 3-month history of recurrent mass on the left thigh. He had presented with a 2-year history of a swelling that was painless but gradually increasing in size to a private hospital where the mass was excised and specimen discarded. Three months later, the mass recurred, but now growing at a faster rate; it later ulcerated and bled occasionally. The patient was the 5th child of his parents. Examination revealed an ulcerated mass measuring 28 Χ 30 cm in diameter on the anterior-medial part of the left thigh [Figure - 2]. A tissue biopsy done confirmed malignant fibrous histocytoma. Plain chest x-ray showed multiple cannon-ball metastases. Patient could not afford angiographic study and so we could not go ahead for surgical excision. Even though the absence of angiography was not an absolute contraindication to surgery, we felt there was no need to operate without an angiography considering distance metastases of the tumor in this patient. His condition deteriorated and the patient died 8 weeks after presentation. Discussion Sarcomas of soft tissue are a heterogeneous group of relatively uncommon tumors that arise predominantly from the embryonic mesoderm and localized mainly at the extremities. There is no identifiable etiology in most cases of STS. The radiologic evaluation of a suspected soft tissue mass has changed dramatically with the advent of computer-assisted imaging. The currently available imaging modalities offer numerous non-invasive methods to diagnose stage and plan for surgical intervention in suspected STSs. Imaging of STSs requires a multimodality approach, with no single imaging modality being ideal for every tumor. The diagnostic evaluation should begin with radiographs of the mass or the region involved. Plain radiographs are still very much rewarding in the developing countries; they are easily accessible and affordable to most patients. They can provide invaluable information when positive. They may reveal skeletal deformity; they can also provide an excellent method for the assessment of osseous involvement by the STS, such as periosteal reaction or overt destruction. [10] All our five patients had plain radiograph of the affected thighs as well as chest-x-ray. None of them had involvement of the underlying femur or pelvic bone, but two of the patients had canon-ball metastases to both lung fields. Although CT is the preferred modality for the identification of pulmonary metastases, [11] none of our patients could afford to have CT of the chest. Ultrasonography is now rarely used as the primary modality for the evaluation of a soft tissue mass; it is a useful adjunct, especially in differentiating cystic from solid masses. [11] Combined color and power Doppler ultrasound, as well as spectral wave analysis, may enable assessment of vascular architecture and altered flow in musculoskeletal tumors. [12] All our patients had abdominopelvic ultrasonography done, but none of them showed evidence of hepatic metastases or any other intra-abdominal organ involvement. Angiography remains important as a preoperative guide to the surgical approach in STS, [13] even though it has been relegated to the background by CT and MRI, we strongly believe that for surgical practitioner in the developing countries where these modern imaging techniques are not readily available, angiography is a necessity in STS close to blood vessels to define the tumor vasculature like in the STS of the thigh. In Case 1, the entire tumor was superficial to the femoral vessels; we probably took advantage of this by not insisting on having angiography done for Case 2 as shown in [Figure - 1]a. Little did we realize that as the femoral vessels emerge below the inguinal ligament, it entered the tumor in a zig-zag manner that only a proper imaging technique will define the relationship of these vessels to the tumor. The tumor was adequately exposed as shown in [Figure - 1]b. As we were excising the mass from the base, guiding the excision with the palpation of the femoral artery proximally, we had transected the femoral vessels more distally in about two to three places. At this point, the vascular surgeons then joined the team to repair the vessels as shown in [Figure - 1]c (the probe pointing to femoral vein while the artery is held by O-silk suture). However, as soon as the vascular clamps were released and the circulation restored to the affected limb, patient had cardiac arrest and all efforts to resuscitate her failed; she was later certified dead. That experience informed our insisting on an angiography before surgery for Case 3. Even if the patient had survived after these prolonged 10-hour ischemic time, the lesson we have learnt there is that angiography is a necessity for surgeons practicing in this part of the world before embarking on such procedure. The tumor in Case 3 is more distally located as shown in [Figure - 2]. Angiography revealed extensive entrapment of the superficial femoral vessels; the circumflex vessels were not clearly outlined. Intraoperatively, we were well guided even though the circumflex vessels that could not be outlined by the angiography were involved with the tumor. The surgical excision was successful without damage to the neurovascular bundles of the affected thigh. We also insisted on angiography for Case 4 before the surgical excision took place, the angiography revealed no relationship of the tumor to the major vessels. The tumor was removed without injury to the femoral vessels. Case 5 was a 16-year-old boy with STS of the thigh as shown in [Figure - 2]. We insisted on having the angiography done before the surgical excision; patient could not afford the cost of the investigation. He later died while still searching for money to do the investigation. Patient with advanced STS like in this 16-year-old boy almost always succumb to death from metastases which he had already had, so removing the tumor without angiography is not likely to prevent death in this patient. CT remains the most effective modality for the detailed evaluation of osseous architecture. It is ideally suited for evaluation of lesions in areas in which osseous anatomy is complex. [14] CT should precede angiography in the investigation of soft tissue tumors and angiography may primarily be reserved for those lesions where vascular relationships are not adequately demonstrated by CT. [15] In a multi-institutional study by the National Institute of Health, the Radiology Diagnostic Oncology Group found no statistically significant difference between CT and MRI in determining tumor involvement of muscle, bone, joint, or neurovascular structures. [14] MR diagnostic accuracy was however said to be superior to that of other techniques; thus MRI replaces CT, while angiography is to be used in highly selected cases. [16] MRI can accurately elucidate the anatomic location of a lesion and the lesion′s relationship to the neurovascular bundle and bone. [17] Recent advances in both hardware and software imaging technology have provided marked improvement in vascular imaging. Magnetic resonance angiograph (MRA) now accurately depicts vascular anatomy obviating conventional diagnostic angiography in most cases. [17] Surgery is still the treatment of choice for STS, although in recent years, it has been integrated with radio-chemotherapy. A lot of progress has been made by these combination treatments; there has been a dramatic reduction in the need for amputations, compartmental excision, and disinsertion of muscle group. We must educate our patients in this part of the world to present early to the hospital. All the five cases presented are large tumors. The clinical stage of the tumor is the most important prognostic factor and it is defined by the tumor grade, size, and presence of distant metastases. The size of an STS is an important prognostic variable. [18] Tumors smaller than 5 cm at presentation have survival rate of 79-82%; tumor of 5-10 cm have survival rate of 62-68%, and those tumors larger than 10 cm have survival rates of 41-51%. [8] The early presentation with small sized tumor have better prognosis than the late presentation with large sized tumors, which are very common in our environment. In the developing countries, we do not have access to most of these recent imaging technologies such as CT, MRI, PET, and MRA; therefore we have to make use of what is available to us. Angiography in the developing countries remains important as a preoperative guide to surgical approach in STS of the thigh; it allows us to guide our dissection with respect to the adjacent vascular structures, thus reducing the operative time significantly and reducing the ischemic time in cases where we have to clamp the femoral artery. This will reduce incidence of reperfusion ischemic injury. Practitioners in this part of the world must ensure that angiography is done by all patients with STS of the thigh undergoing surgical resection; it is a necessity for a good intra-operative tissue dissection. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10009f1.jpg] [am10009f2.jpg] |
| |||||||||

{kind=link}
{kind=link}