 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
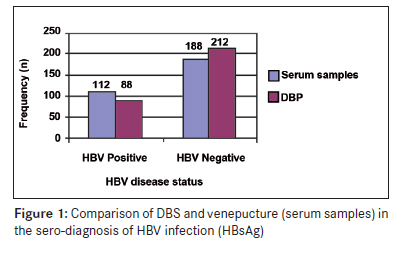
Annals of African Medicine, Vol. 9, No. 1, January-March, 2010, pp. 44-45 Letter To Editor Application of dried blood spot in the sero-diagnosis of hepatitis B infection (HBV) in an HBV hyper-endemic nation Forbi JosephC, Obagu JoyO, Gyar SilasD, Pam ChristopherR, Pennap GraceR, Agwale SimonM Virology Research Laboratory, Innovative Biotech, Keffi/Abuja, Nasarawa State Code Number: am10010 PMID: 20418650 DOI: 10.4103/1596-3519.62625 Dear Sir, Over two billion people are infected with hepatitis B infection (HBV) worldwide and every year approximately one million people die of HBV infection, 33% caused by hepatocellular carcinoma, and the rest with terminal complications of liver disease. [1] The use of dried blood spot (DBS) on filter papers in the molecular diagnosis of hepatitis B infection by polymerase chain reaction (PCR) has been shown to be specific, sensitive, and has the ability to detect as little as 10 virus particles by ethidium bromide staining of the PCR products. [2] The use of DBS in the diagnosis of infection makes the collection and transportation of samples easier especially in countries like Nigeria where HBV is hyper-endemic. [3] This study evaluates the applicability of DBS for the routine serological diagnosis of HBV infection. Three hundred (n = 300) samples (age range = 18-45 years, all males) collected by venepuncture and small amounts of blood from the syringe applied to filter papers (DBS) (Whatman no. 3 filter paper, Whatman international Ltd, England) were serologically tested for HBsAg. The larger volume of whole blood was spun and the sera stored in cryovials at -20 0 C at the Virology research laboratory, Innovative Biotech, Nigeria, until used. For the filter paper samples, individual drops of blood from the syringe, each approximately 25 ΅l, were spotted onto filter paper, air dried, stored at room temperature (not desiccated) until used. Hole punch was used to detach the filter paper containing a DBS into a 1.7-ml Eppendorf tube and flamed forceps were used to force the disc into the bottom of the tube. One disc of blood collected from each subject (approximately 25 ΅l of blood) was used for testing. And 50 ΅l of phosphate buffer saline (PBS) was added to each tube. This was incubated at 4C overnight. Each sample was spun at 8000 rpm for 5 min to force the filter paper disc and other debris to the bottom of the tube. Supernatants were used for the test. HBsAg were determined using a third-generation commercial enzyme-immunoassay (Shantest TM - HBsAg ELISA, India, lot number: DHB 01306) for both sera and DBS. The test was conducted according to manufacturers′ instructions and the microplates read at a wavelength of 450 nm using an ELISA reader (BIO-RAD 2100, version 6.1, USA). The presence or absence of HBsAg was determined by relating the absorbance of the unknown sample to the cut-off value. The cut-off value is the mean of the optical density (OD) of the negative control plus the factor 0.025. Specimens with OD values greater than or equal to the cut-off value established with the negative control were considered positive, while those with ODs lower than the cut-off value were recorded as negative. Only individuals who signed the inform concern form were allowed to participate in this study. The following mathematical calculations were used to determine the sensitivity and specificity of the DBS in the serological determination of HBV status: Sensitivity = Number who are both disease positive and test positive/number who are disease positive = True positive/true positive + false negative Specificity = Number who are both disease negative and test negative/number who are disease negative = True negative/true negative + false positive Of the 300 samples tested, 112 and 188 were positive and negative, respectively, using serum samples while 88 and 212 were positive and negative, respectively, using DBS. The sensitivity of the DBS in screening for HBV infection was 78.6%, while its specificity was 88.6%. Twenty-four (n=24) HBV-positive samples that were detected using serum samples were not detected using BDS. This is further illustrated in [Figure - 1]. Sero-diagnosis of HBV in Nigeria is traditionally carried out by collecting venous blood and testing for HBsAg. [4] The use of filter papers is an attractive alternative to the use of larger volume tubes for blood collection and storage for several reasons. Only a few drops of blood are applied to the paper, and this amount can be obtained by a heel stick. Venepuncture of small infants is not always successful; the amount of blood obtained is sometimes insufficient and mothers of small infants are often more comfortable with a heel stick than venepuncture. [5] Dried blood samples on filter can be stored at room temperature, eliminating the need to store and transport whole or separated blood samples in liquid nitrogen. The use of filter papers also provides fewer chances for mislabeling because there are no transfer steps once the blood is applied to the paper. In developing countries like Nigeria, sample collection, storage, and processing are difficult and expensive. Our evaluation of the use of DBS on filter paper showed a sensitivity and specificity of 78.6% and 88.6%, respectively. This is not optimal as 24 of 112 HBV-positive samples could not be detected by this method. We think that these could be the border-line sample with low titres. We, therefore, conclude that the use of DBS on filter paper is not as optimal in the serological diagnosis of HBV as it is good in molecular diagnosis by PCR and should not be used for the routine sero-diagnosis of HBV infection. We also think that the type of filter used in this study could have affected the results. We propose further studies to elucidate our findings. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10010f1.jpg] |
| |||||||||

{kind=link}