 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
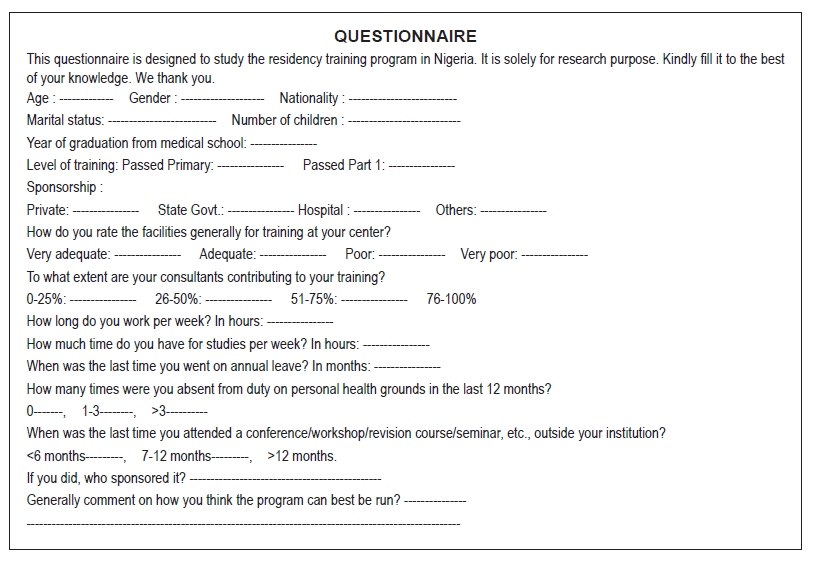
Annals of African Medicine, Vol. 9, No. 2, April-June, 2010, pp. 91-94 Original Article Residency training program: Perceptions of residents L. M. D. Yusufu, A. Ahmed, V. I. Odigie, I. Z. Delia, A. A. Mohammed Department of Surgery, Ahmadu Bello University and University Teaching Hospital, Zaria, Nigeria Correspondence Address: Dr. L. M. D. Yusufu, Department of Surgery, Ahmadu Bello University and University Teaching Hospital, Zaria, Nigeria. yusufulazarus@yahoo.com Code Number: am10019 PMID: 20587931 DOI: 10.4103/1596-3519.64745 Abstract Background: There is a phobia among doctors for the residency training program, since the establishment of the program over 30 years ago. The reason for establishing the program was mainly to provide the much-needed specialists in medicine. Objectives: To ascertain the perception of the residency training program among residents. Materials and Methods: Structured questionnaires were administered to residents at 3 training institutions in Nigeria. Results: One hundred nineteen (85.5%) questionnaires were returned out of 140. The ages of respondents ranged from 27 to 42 years, the median age being 30 years. There were 110 males and 9 females. One hundred six (89.1%) were junior residents. Ninety (75.6%) were sponsored by the training institutions. Seventy-four (62.25%) felt their consultants were contributing just 50% or less to their training. Sixty-two (52.2%) of the respondents had attended a revision course, conference or seminar within the last 6 months. Majority of the residents would want better remuneration, up-front payment of examination and revision fees, more teaching by the consultants and less emphasis on the provision of services as ways of improving the program. Conclusion: Majority of the residents are sponsored by the training institutions.Keywords: Decentralization, motivation, perception, remuneration, residents Résumé Arrière-plan: Est une phobie pour le programme de formation de résidence par les médecins, depuis l’établissement du programme il y a plus de trente ans. La raison de l’établissement du programme était principalement de fournir l’indispensable spécialistes en médecine. Objectifs: Pour vérifier la perception du programme de formation de résidence par des résidents. Methodes: Structuré questionnaires ont été administrés à des résidents à 3 établissements de formation au Nigéria. Resultats: Une centaine et dix-neuf questionnaires ont été renvoyées d’un cent et quarante, 140 (85.5%).The âges des répondants varies de 27-42years, âge médian était 30years.There étaient 110 mâles et 9 femelles. Une centaine et six, 106(89.1%) étaient des résidents juniors. Quatre-vingt-dix (75,6%) ont été parrainés par les institutions de formation. Soixante-quatre (62.25%) estimaient que leurs consultants ont contribué à seulement 50% et moins de leur formation. Soixante deux (52.2%) des répondants avaient assisté à un cours de révision, Conférence ou un séminaire au cours des six derniers mois. La majorité des résidents voudrait une meilleure rémunération, haut-avant le paiement de frais d’examen et de révision, plus pédagogique par les consultants et moins l’accent sur la prestation de services comme des moyens d’améliorer le programme. Conclusion: La majorité des habitants sont commandités par les institutions de formation. Mots clés: Résidents, rémunération, perception, decentrilization, motivation Introduction The residency training program in Nigeria was formally established in 1974, with the objective of providing specialist training at a high level and appropriate to the needs of Nigerian population. The other objective was to halt the brain drain taking place as a result of relocation of the much-needed medical specialists to the developed world. [1],[2],[3] The training of specialists in our country in the long run was cheaper, with the downturn of the Nigerian economy. There is a perceived phobia for this program among students and doctors alike. Residency training in America began in the 20 th century; then, trainees lived in hospitals and served variable periods of time in service in an apprenticeship mode. [4] This training began to be associated with medical schools soon after, in addition to rotating internships. This study was carried out to ascertain the perception of the residency training program among residents in some training institutions in northwestern Nigeria. Materials and Methods One hundred forty 18-item self-administered questionnaires were distributed among residents at Ahmadu Bello University Teaching Hospital, Zaria; Aminu Kano University Teaching Hospital, Kano; and Usmanu Danfodio University Teaching Hospital, Sokoto, in March 2005. The questionnaires sought to know from the respondents their general perceptions of the program and their suggestions on how to improve the program. The data obtained was analyzed using simple statistics. Results are presented as percentages and in the form of tables, and they form the basis of this report. Results There were 119 (80%) respondents - 110 males and 9 females. The ages of respondents ranged from 27 to 42 years, the median age being 30 years. Of these, 106 (89.1%) respondents were junior residents, while 13 (10.9%) were senior residents (those who had passed part I). Residents work for between 80 and 168 hours per week (median, 92 hours), excluding call duty. Sixty-two (52.1%) of the respondents had attended a conference, revision course or a workshop within the last 6 months of the study, while 12 (10.1%) were yet to attend any course, since joining the program. Sixty-one (51.3%) of the residents had not gone on any form of leave during the last 12 months as at the time of the study. Analysis of the respondents showed similar findings for both senior and junior levels of training. Discussion The introduction of the residency training program in Nigeria over three decades ago was meant to provide the much-needed medical specialists locally. The number of male residents far outnumbered that of the female residents, which is probably a reflection of the graduation pattern in our medical schools. Recently more women are being challenged to pursue postgraduate medical education in all specialties of medicine. [5] The greater proportion in favor of junior residents indicates that the number of doctors pursuing postgraduate education is increasing. [6] The training institutions sponsor majority of the residents [Table - 1]. This is commendable and is in keeping with their statutory mandate, the other responsibilities being the provision of service and research. These training institutions are accredited by the National and West African Postgraduate Medical Colleges. [5] The sites for this study were all tertiary institutions, where most of the training is done in the country. There are a few secondary institutions and private hospitals where training is done in some specialties. [5] The perceptions may not entirely reflect the views of residents in smaller programs. Most residents considered the facilities in their centers as being below average [Table - 2]. This is worrisome and is supported by reports that accreditation of some centers has been withdrawn completely or partially in some specialties. The contribution by consultants to training is between 26% and 50% as reported by some 53 (44.5%) of the respondents [Table - 3]. This finding is disturbing and calls for urgent issues to be addressed. Consultants as leaders, teachers, role models and mentors should guide, train and impart knowledge to residents in particular. [5] In spite of the limitations of the current training program and the working conditions in the country, consultants should make sacrifices for the sake of the profession and country at large. Consultants can assist by insisting that residents make judicious use of their time and pass through the graded promotion from internship to chief residency. [5],[7],[8] Residency should be educational rather than a means of supplying cheap assistants and manpower to both the consultants and the training institutions. [1],[5],[7] Conference, seminar attendance and revision courses are very important for continuing education. These should be encouraged and supported by the training institutions. Residents must justify the huge investment by government on them, by studying and taking active part in patient care. [1],[5] The working hours of the residents appear to be within the approved government regulation. In the clinical setting, majority of the clinicians work, the essence being patient care rather than time spent at the duty post. In America, the effective date of a new work-hour week restriction was July 2003. [9] The residents are now limited to working no more than 80 hours per week, in-house call can be no more frequent than every third night and 24-hour shifts must be followed up by at least 10 hours free of clinical duties. There are concerns about the new regulation already; one study reported that residency training and patient care have worsened. [9] The traditional graded operative experience of surgical education was altered, and a decrease of operative continuity care by residents was reported by another study. [10] Depending on the schedule of various units, rest in the form of leave is beneficial in the long run, as fatigue from overwork invariably can lead to lower productivity and increase the risk of errors and adverse events. [11] The summary of this study is indicated by the suggestions made by the residents [Table - 4]. The suggestions made by the residents as ways of improving the training program are timely. Considering the Nigerian economy, the total take-home pay of the residents can be improved upon, as an incentive to attract many young doctors into the program. Consultants as team leaders must use their abilities as teachers, role models and mentors to positively influence the residents. [12] The training of residents in general and the surgical residents in particular has become complicated because of the expansion of human medicine and its subspecialties. It is becoming increasingly difficult to get admitted for training in many centers in our country and the United States of America. There is so much to teach and there are increasing limitations of time and opportunity, and this has brought about a growing concern about the expertise of the residents, after completing the program. [13] The provision of environment conducive to learning, educational aids, journals, improved funding; and establishment of more training centers will go a long way in addressing the complaints of residents. The National Postgraduate Medical College of Nigeria has started decentralizing the examinations at the primary level, for some time now. Effectively decentralizing the examinations at all levels will require more examiners, more funds and more training centers. With government support, this is realizable in the near future. Government at this time should consider re-introduction of the 1-year elective posting abroad. This elective posting had helped bridge the gap between our training and the training abroad. [7] It had also offered the residents the opportunity to observe and practice medicine at the best of centers. The benefits of this cannot be overemphasized. The reason for the suspension of the elective posting program was lack of funds, which is no longer tenable considering the state of the Nigerian economy. Conclusion The training institutions are responsible for the training of majority of the residents. There are more male residents than female residents. Training facilities were considered poor by majority of the residents, who also considered contribution by consultants to their training as being 50% or below. Majority of the residents suggested improved remunerations and funding of training centers, provision of environment conducive to learning, more teaching by the consultants as some ways of improving the residency program. The other suggestions made by a few residents were, less emphasis on provision of services, decentralization of the examinations and re-introduction of the 1-year elective posting abroad, among others. References
Copyright 2010 - Annals of African Medicine The following images related to this document are available:Photo images[am10019t4.jpg] [am10019t3.jpg] [am10019t2.jpg] [am10019t1.jpg] [am10019q1.jpg] |
| |||||||||

![[Table - 1]](/showimage?am/photo/am10019t1.jpg){kind=link}
![[Table - 2]](/showimage?am/photo/am10019t2.jpg){kind=link}
![[Table - 3]](/showimage?am/photo/am10019t3.jpg){kind=link}
![[Table - 4]](/showimage?am/photo/am10019t4.jpg){kind=link}
{kind=link}