 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
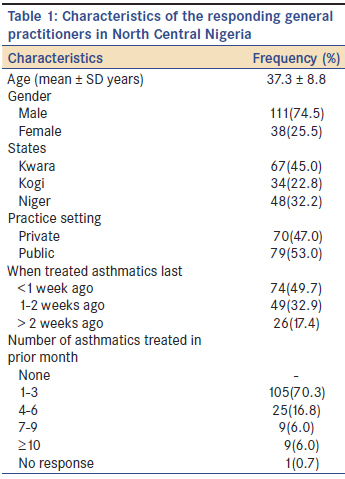
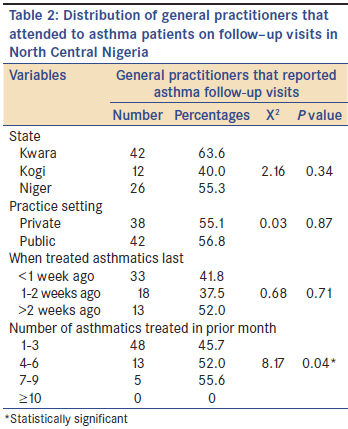
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 209-213 Original Article General practitioner reported follow-up visits among asthma patients in North Central Nigeria AE Fawibe1, KJ Joseph2, OF Olaosebikan3, AK Salami1, PO Oluboyo1, OO Desalu1 1 Department of Medicine, University of Ilorin Teaching Hospital, Ilorin, Kwara State, Nigeria PMID: 21912004 Abstract Background: Despite the benefits of regular follow-up in the long-term care of asthma, no previous study has reported on it among asthma patients in Nigeria. Keywords: Asthma care, follow-up visits general practitioners, Nigeria Introduction Asthma is a chronic inflammatory disease of the airways, resulting in widespread but variable airflow obstruction in response to a variety of stimuli. [1] The airflow obstruction is usually reversible, either spontaneously or with treatment, although airway remodeling may lead to irreversible structural changes. It is a severe and sometimes fatal disease affecting a large proportion of the population. It can limit patients′ activity levels, reduce their quality of life and increase their likelihood of being admitted to hospital. [2] For many years, asthma was perceived and managed as an episodic disorder of the airway smooth muscle. [3] With better understanding, it is now known to be a chronic inflammatory disorder of the airways which requires the daily use of controller medications in most patients to prevent symptoms, improve lung function and prevent attacks. The current goal of asthma care is to achieve and maintain control of the clinical manifestations of the disease for prolonged periods. [1] In addition to the requirement for patients to take medications as prescribed, they are also asked to adopt a range of behavior patterns in order to manage and achieve good control. These include regular follow-up visits to healthcare providers, monitoring of symptoms, avoidance of aggravating factors, exercising, and lifestyle modifications. [4] Regular follow-up visit is a key component of asthma care. [5],[6] It is a major factor necessary for the development of patient/care giver partnership. This is the first of the four components of asthma care recommended by global initiative for asthma (GINA) guidelines. These guidelines emphasized the role of regular follow-up visits in effective long-term control of asthma. [1] The regularity of follow-up visits may also help to predict medication adherence. This is because a patient that is not regular on follow-up is unlikely to adhere strictly to the prescribed treatment plan. Furthermore, patients that are not regular on follow-up may not have adequate monitoring of their lung function. Despite these benefits of regular follow-up visits, many asthma patients do not enjoy regular follow-up care from their health care team. Smith et al. [7] and, more recently, Zorc et al. [8] reported low rates of follow-up visits with primary care providers in their studies among asthma patients. Other similar studies [9],[10] from developed world have also shown that many asthma patients were treated at walk-in clinics and emergency departments, hence, did not receive regular follow-up care from medical professionals. Therefore, their education was woefully inadequate and their compliance with treatment was very poor. In Nigeria, there is paucity of data on various aspects of asthma care. And we are not aware of any previous study on follow-up visits among asthma patients in the country. This survey is therefore designed to evaluate general practitioner (GP)-reported follow-up visits among asthma patients in North Central Nigeria. Materials and Methods This was a cross-sectional survey conducted from September to December 2009 among GPs in three of the six North Central states of Nigeria. The states (Kwara, Kogi, and Niger) were selected for reasons of convenience of the investigators. Study site Nigeria, with an estimated population of about 140 million people, is the most populous black nation in the world. It is located in West Africa with a coast along the Atlantic Ocean on the Gulf of Guinea. The North Central region is one of the six geopolitical zones in the country. It has six states namely Kwara, Kogi, Niger, Plateau, Nassarawa, and Benue. Data collection All GPs in both private and public hospitals from the capital cities of the selected states were contacted for recruitment into the survey. Only those GPs who consented (verbal consent) to participate in the study were recruited. Of about 158 GPs contacted, 149 (94.3%) consented to participate. They were asked to complete a pretested, self-administered questionnaire. Ten GPs who participated in the pretest were excluded from the survey since they had already seen the items on the questionnaire. At each of the hospital visited, questionnaires were distributed to consenting GPs and collected back after 20-30 min. Whenever a participant was too busy, an appointment was scheduled for a later date. We did not leave the questionnaires with the GPs. The questionnaire was self-designed to obtain information on the age and gender of the respondents; their practice location, practice setting, when last they treated asthma patient, the number of asthma patients treated within the last one month prior to the survey. In addition, they were also asked to respond "yes" or "no" to the following questions; (a) Do your asthma patients usually come for follow-up visits? (b) Did you attend to any asthma on follow up visits within one month to the survey? Data analysis was by SPSS version 13.0. The mean ± standard deviation was calculated for the ages while percentages were calculated for the categorical variables. Data comparison for the categorical variables was done using the Chi-squared test. P value < 0.05 was considered significant. Results One hundred and forty-nine (94.3%) out of 158 contacted GPs agreed to participate in the study. They were predominantly (111; 74.5%) males with a mean age of 37.3 ± 8.8 years and a range of 25-70. Most (105; 70.5%) of them reported that they attended to an average of 1-3 asthma patients in the month preceding the survey. The other characteristics are shown in [Table - 1]. Overall, 72 (48.3%) of them reported that their patients usually come for follow-up visits (i.e. answered "yes" to the question "Do your asthma patients usually come for follow-up visits). [Table - 2] shows the distribution of GPs that reportedly attended to asthma patients on follow-up visits in the month preceding this study. Forty-two (63.6), 12 (40.0%) and 26(55.3%) of the GPs in Kwara, Kogi, and Niger states, respectively, reported that their asthma patients came for follow-up visits in the preceding month. The difference was however not statistically significant (P = 0.34). There was also no significant difference (P = 0.87) in the asthma follow-up visits reported by GPs in private hospitals (38; 55.1%) compared to those in public hospitals (48; 56.8%). Thirty-three (46.5%), 19 (37.5%), and 13 (52.0%) of the GPs who attended to patients <1 week, 1-2 weeks and >2 weeks prior to the study reported that their patients came for follow-up visits. The observed difference was however not significant (P = 0.71). As shown in [Table - 2], there is significant difference (P = 0.04) in the reported follow-up visits by GPs who attended to ≥10 asthma patients compared to other GPs. None of the nine GPs who reportedly treated ≥10 asthma patients in the month prior to this study attended to any patient on follow-up visits. All their patients came for treatment of acute exacerbation of their asthma. Discussion The results of this survey suggest that many asthma patients in North Central Nigeria do not receive follow-up care from their primary care physicians. Overall, less than half (48.3%) of the GPs reported that their asthma patients usually come for follow-up visits. In Kwara and Niger states, more than half of the GPs reported that their patients came for follow-up visits in the month preceding this study. However, follow-up visit was very low in Kogi state where only 40.0% of the GPs reported that their patients came for follow-up visits. Also, less than two-third of GPs in both private (55.1%) and public (56.8%) hospitals reportedly attended to asthma patients on follow-up visits in the month prior to our survey. These findings suggest that majority of asthma patients in North Central Nigeria do not go to their GPs for follow-up treatment of their asthma. This is similar to an earlier report in seven European countries in which majority of asthma patients only visited caregivers when they were experiencing trouble with their asthma. [11] Smith and co-workers [7] as well as Zorc et al. [8] also reported low rates of follow-up visits in their patients after they were discharged from emergency department. Despite various interventions aimed at improving follow-up visits, only 37% (Smith et al.) and 44.5% (Zorc et al.) of their patients went for follow-up. The lower rates of follow-up visits reported by them may be due to the fact that they reviewed the medical records to verify reported follow-up visits. We did not review any record in this study to verify the reported rates of follow-up. Those GPs who attended to ≥10 asthma patients in the month prior to this survey reported that none of the patients were for follow-up visits. They all reportedly came for treatment of acute exacerbation of their asthma. This is in keeping with studies of Krishnan et al. [9] and Heisler et al. [10] Both of whom had earlier reported that many asthma patients were not going for follow-up visits but were treated at walk-in clinics and emergency departments when they developed acute exacerbation of their asthma. It was difficult for us to identify the factors that were responsible for the low rates of follow-up in our study because we relied on report from the physicians. Furthermore, we are not aware of any previous local study aimed at identifying the reasons for poor follow-up visits among asthma patients in Nigeria. However, previous studies [8],[12] from other parts of the world have identified barriers to asthma follow-up visits. These barriers were broadly divided into three groups: (a) personal and social (e.g., no transportation to the appointment), (b) system and organizational (e.g., long wait to see a physician, inconvenient hours) and (c) financial barriers. [8],[12] This survey is important because of the possible impact of follow-up care on the overall outcome of asthma patients. This is because continuous monitoring of patients is a key component of asthma management. Lack of medical follow-up has also been associated with under-use of inhaled anti-inflammatory treatment by patients. [13],[14] Furthermore, the stepwise approach to asthma management recommended in the guidelines [1] necessitates regular review of treatment once asthma is under control. [15] Long- term follow- up of asthma patients is also very important because it helps to improve patient′s understanding of asthma care, assists in adapting treatment according to the evolution of the asthma, and also help in providing psychological support that is always necessary for chronic illnesses. [16] This study has a number of limitations. One of this is the fact that it is based on report by GPs who may have been biased in their report. Another major limitation is that some patients might have developed acute exacerbation while on a visit to the surveyed area. This category of patients would have been reported by the GPs as not coming for follow-up visits. Also, owing to paucity of fund for the study, data collection was limited to the state capitals thereby excluding information from the rural areas where majority of the populace resides. However, despite these limitations; this survey has shown that follow-up care among asthma patients, as reported by GPs in North Central Nigeria, is poor. We therefore recommend that further studies should be undertaken to identify the factors responsible for this in order to address them. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11043t2.jpg] [am11043t1.jpg] |
| |||||||||

{kind=link}
{kind=link}