 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
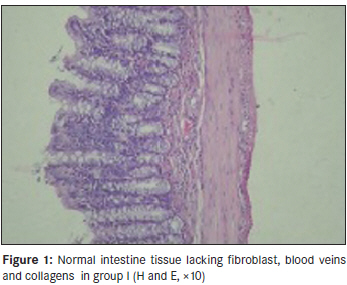
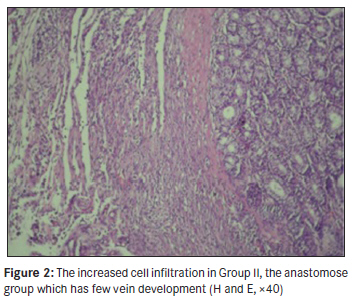
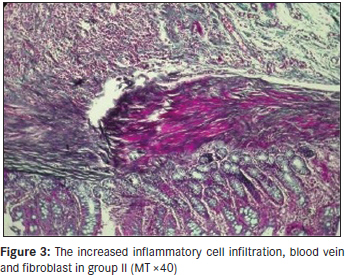
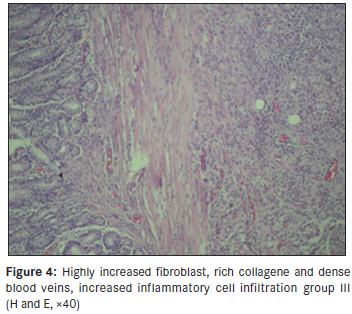
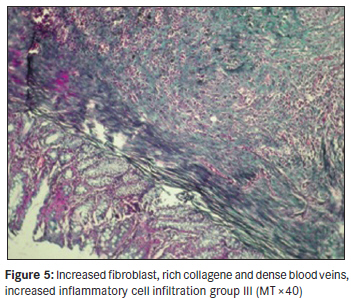
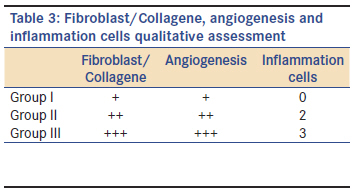
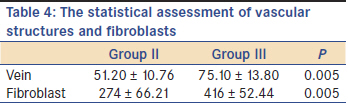
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 220-225 Original Article The effect of extracoporeal schock waves on intestinal anastomosis Ceyhun Pekin, Sakir Tekin, Tevfik Kucukkartallar, Murat Cakir, Ahmet Tekin, Adil Kartal Selcuk University, Meram Medical Faculty, Department of General Surgery, Turkey Code Number: am11045 PMID: 21912006 Abstract Background and Objectives : To investigate the effect of extracorporeal shock waves on the healing of intestinal anastomosis. Keywords: Extracorporeal shock wave, intestinal anastomoses, wound healing Introduction New methods aiming at healing process of wounds and ideal scar occurrence by affecting the factors playing role in the healing of wounds such as inflammatory cells, platelets, mediators, extracellular matrix. The effects of physical powers like electrical current, laser, ultrasound on tissue damage repairing were demonstrated in experimental studies. These energy types will significantly contribute to healing of the wounds and become beneficial methods with technological developments. One of them is the study done with ultrasound waves. Ultrasound is applied, microscopic sized air bubbles occure on the tissue. This process causes changes in the cell membrane permeability. Ultrasound have on the tissue is its producing a measurable decisive mechanic power. The change in the cell membrane permeability and the increase in diffusion caused by air bubbles and mechanic current is claimed to have positive effect on the healing of the wounds. [1] Besides, it was also demonstrated that it directly stimulate the forming of cells like fibroblast and macrophage and new vessels. The latest area of clinical application of extracorporeal shock wave treatment (ESWT) is in wound healing. The experience with ESWT so far suggest that it is effective and may be useful in variety of complex wounds. The studies have shown that ESWT increases the release of critical wound growth factors and contributed to vascular development. [2] From this observation, we became interested in studying the effects of postoperative extracorporeal shock waves on colon anastomoses in the prevention of anastomotic leaks which is associated with increased mortality, morbidity, and cost hospitalization and loss of productivity. Materials and Methods With approval from Ethical Board of Meram Faculty Research Center at Selcuk University. 30 Wistar Albino female rats whose average weight is 200 g were procured for this study. The rats were fed liberally in the days leading up to the study including drinking water under 25°C until. 12 hours before the operation. The rats were divided into three groups each composed of 10 rats. After all the subjects were subjected to general anesthesia with 50 mg/ kg intramuscular (im) ketamine, the right colon was approached by median laparotomy incision. By keeping the right colon bleeding, 1 cm segment resection was done on the right colon 5 cm distal to ileocecae valve. The proximal and distal intestine were anastomosed end-to-end with 6/0 Vicryl (Ethicon) sutures. Eight sutures were put in each anastomosis. Afterwards, the abdomen was closed with continioued sutures using 3/0 Vicryl. The control group (group I) rats were only subjected to laparotomy. Anastomosis group II subjects were subjected to colon resection and anastomosis. ESWT group III rats were given extracorporeal shock waves with Dornier MPL 9000 device working with electrohydraulic system under ketamine anesthesia on the 3 rd , 5 th , and 7 th days after colon resection and anastomosis. In each session, 14 KV and 400 impulses were applied, 1200 impulses 0.12 mj/mm 2 shock waves totally. The rats were sacrificed with high dosage of ether inhalation on the 10 th day after laparotomy. The abdomen and anastomose were explored in the second look and the colon segment which includes 4 cm colon segment was resected and the two ends were tied together 3/0 silk suture and obliterated after catheter was placed into the lumen. To measure the pressure a manually operated sphygmomanometer was attached to catheter. The intraluminal pressure was increased with air in a container full of liquid. The explosion pressure measurements were done by technicians who were blinded to the operation. The explosion pressure was recorded as the value measured at the time when anastomotic leak with air bubbles on the anastomose line are seen. Later on, 1 cm tissue including 0.5 cm distal and proximal of the anastomotic line was resected and fixed with 10% formalin for histopathological examination. The tissues were prepared in paraffin-block, the thin sections were dyed with Masson′s Trichrome (MT) to show angiogenesis and inflammatory cells, Hematoxylin-Eosin (HE) and fibroblast-collagen tissue and were examined under light microscopy. The sections taken from each tissue were examined under 40 or 400 times enlargement and their vascular formations and fibroblast were counted. The scoring used by Rayner et al. which scales the severity of inflammation from 0 to 3 was used to score inflammation. Accordingly, 0 means no inflammation, 1 means rare patched lymphocyte and plasma cells, 2 means increased lymphocyte, neutrophil and plasma cells, 3 means a great deal of complex inflammation cells and the existence of micro-apse. [3] According to the method proposed by Brown, each prepared was assessed as rare (1 positive), mild (2 positive), dense (3 positive). [4] All the statistical evaluations were carried out by using the SPSS (Windows release 10.0, SPSS Ine, the USA). The anastomosis explosion results on the 10 th day after anastomose recovery was assessed with Student t test. In addition, one-way variance analysis (ANOVA) was used in the assessment of the number of the vascular structures and fibroblasts. In all the comparisons, P < 0.05 was accepted to be significant. Results During the experiment all the subjects tolerated the operation. No macroscopic anastomose leak was found in sacrificed subjects and there occurred no death after operation. The explosion pressures of the sacrificed rats in Group I and Group II were given in [Table - 1] and the statistical assessments were given in [Table - 2]. The mean for group anastomosis explosion pressures (μ ± SD) was 220 ± 6.8 mmHg in Group II and was 272 ± 7.8 mmHg in Group III. The explosion pressure of Group III was significantly higher than that of Group II (P < 0.05). In histopathological assessments, the normal intestine tissue poor in blood vessels and collagen were observed [Figure - 1]. In Group II increased inflammatory cell infiltration, blood veins, dense fibroblast proliferation and rich collagen density [Figure - 2] and [Figure - 3], in Group III highly increased fibroblast, collagen, blood vessel formation-compared to Group II- and inflammatory cell infiltration were observed [Figure - 4] and [Figure - 5]. The qualitative assessment results of collagen, angiogenesis and inflammatory cell infiltration formation by a pathologist is given [Table - 3], the average rates of the number of the vein and fibroblast in these sections and their statistical comparisons are given at [Table - 4]. Using Tukey HSD, the means of the three groups were significantly different from each other, which means that the angiogenesis and fibroblast number in ESWT applied Group III was statistically and significantly higher compared to that of laparotomy group (Group I) and the anastomosis (Group II). Discussion There have been many experimental studies examining the relation between the integrity of colon anastomosis and wound collagen content. In the first few days following anastomose, there is collagen formation-destruction not only in the anastomosis region but also in the adjacent intestine wall. These studies showed that the hydroxylproline level on the suture line and decreased after colon anastomoses. [5],[6],[7] Hawley et al. [8] attributed this decrease to the activity of collagen enzymatic degradation. There needs to be a balance between collagen synthesis and degradation for the healing process of the colon. It is thought that decreasing or limiting the collagen degradation, in particular during the initial phase of wound recovery, will increase post-operative wound tensile strength and decrease anastomotic leakages. [9],[10] Unlike its use in the treatment rationale in kidney stones, the reason for application of shock waves in orthopedic is to stimulate tissue regeneration. The studies have demonstrated that ESWT increased the release of the growth factors and stimulated vein growth in critical wound recovery. [1],[11],[12] Although the effects of extracorporeal shock waves on angiogenesis, cell proliferation and tissue regeneration which are the basic factors in wound recovery are not known completely, it was shown in animal studies that it stimulated the early expression of the angiogenesis related growth factors like eNOS (endothelial nitric oxide synthesis), VEGF (vascular endothelial growth factor) and PCNA (proliferated cell nuclear antigen). Later on, it induces neovascularisation which provides blood flow and stimulate the cell proliferation and tissue regeneration. [13],[14] Therefore, we thought that ESWT can positively contribute to wound recovery and we examined wound recovery and anastomose safety by applying ESWT to the anastomose area. Histopathological studies show beneficial features in the definition of the healing process at tissue level. In our study, we looked for fibroblast, blood vessels and collagen. In the ESWT group (Group III), we noted increased fibroblast, collagen, neo-vascularisation and increased inflammatory cell infiltration. In the same group we have noted increases in vascular sizes compared to those of colocolic anastomosis (Group II) and control group (Group I) (P < 0.005). This is an important finding which makes us think that ESWT induced angiogenesis. In ESWT group fibroblast/collagen levels are significantly higher than those of the other groups (P < 0.05). These findings make us think that ESWT has to the healing of the anastomosis. In a study involving 102 patients (18), 100-1000 shock cm 2 0.1 mj/mm 2 ESWT was applied to 104 soft tissue wounds with poor healing capacity, the treatment was applied in one week intervals or every other week in 1 to 6 cures (mean 3) according to tissue regeneration rate. The average cure period was 3 minutes and after 3 to 12 week monitoring the epitalization rate was carefully determined. Accordingly, there was 81% complete healing, 12% partial healing. However, there was no epitalization over 50%. Although the wounds were colonized by bacteria, no antibiotics were used. The fact that infection did not aggravated was attributed to the probable bactericidal effect of ESWT. Even in chronic venous stasis and arterial insufficient ulcers, there was observed a fast recovery. In 53% of the patients recovered fully, in 28% of the patients there was 50% epithelization. [15],[16] Although ESWT technology is rather different from standard soft tissue treatment, its potential benefit for the wound is the same in the content. Besides ESWT locally decreasing the bacteria amount in the wound and increasing the granulation tissue production, it also increases vascular density and blood flow in the wound. [17] This hastens healing and inhibits bacterial growth. It was shown that ESWT decreased the need for secondary suture, flap or graft and provided potential epitalization. [17],[18] Ludwig et al. described that ESWT has positive effect on wound healing. [19] In the clinical research carried out by Schaden it was demonstrated that ESWT is very effective in venous and arterial ulcers, decubitus ulcers, post-traumatic wounds and many acute chronic ulcers including burns. [16],[17],[20] Mechanic parameters are the most reliable tools in assessing anastomotic healing. Explosion pressure is the resistance of the wall to the increasing intra-luminal pressure and it is the most reliable measurement as it correctly reflects the tensile strength of the intestine therefore, it is used frequently. The explosion pressure is especially reliable as the most valid parameter in the early postoperative periods (3-7 days) when the anastomosis separation is the largest. [19],[21],[22] In our study, in the explosion pressure measurements we found that it was statistically higher in ESWT group compared to anastomose group ( P < 0.05). The tension power of intestine wall is essentially determined by sub-mucosal collagen. The main element determining intestinal anastomotic strength is the quality of collagen fibrils in addition to collagen mass. [23],[24] The most important factor that provides the mechanic stabilization and the tension strength of collagen fibrils is the formation of inter-molecular cross-links. Although it is thought that impaired healing will result in the reduction of the tensile strength of anastomosis in cases with impaired formation of these cross-links, there is very little information about the structural features of intestinal anastomose collagen cross-links. [7],[19],[22] It is found there is generally no correlation between anastomotic collagen content and mechanical parameters. It is thought to have resulted probably from researchers focusing on the mass of the collagen rather than the collagen quality of the researches. [19],[25],[26] Because of the problem in showing newly synthesized collagen, methods radiolabelled proline injection to reflect new collagen synthesis directly were defined but their being expensive limits their usage. Therefore, we thought that it would be beneficial to use MT stain in the histopathological sections of the anastomotic line. In our study, we have found that the collagen level is significantly higher in ESWT group compared to other groups. Conclusion We have demonstrated that, extracorporeal shockwave treatment positively affected the anastomotic healing parameters (angiogenesis, fibroblast, collagen) after colon anastomosis. We conclude that it will enhance anastomotic integrity and prevent anastomotic leaks. Further experimental and clinical studies may shed more light on this. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11045f2.jpg] [am11045t1.jpg] [am11045t4.jpg] [am11045t2.jpg] [am11045f4.jpg] [am11045f1.jpg] [am11045t3.jpg] [am11045f5.jpg] [am11045f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}