 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 227-232 Original Article Effects of hyperthermic intraoperative peritoneal lavage on intra-abdominal pressure in an experimental model of peritonitis: A randomized, controlled, blinded interventional study Robert B Sanda, Aslam A Patta, Omer A Omer, Syed Ashraf, Elrasheed Omar Hail General Hospital, Hail 81451, Kingdom of Saudi Arabia, Drumheller Hospital, Drumheller, T0J 0Y1, Alberta, Canada, Code Number: am11047 PMID: 21912008 Abstract Background: Hyperthermic Intraoperative Peritoneal Lavage (HIPL) is useful for bacterial decontamination and prevention of hypothermia during damage-control surgery (DCS). Little is known about the effect of HIPL on intra-abdominal pressure (IAP) alone or in combination with peritonitis.
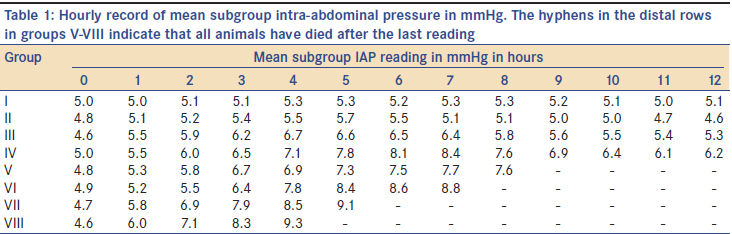
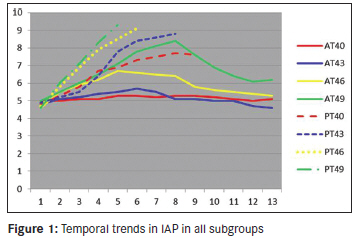
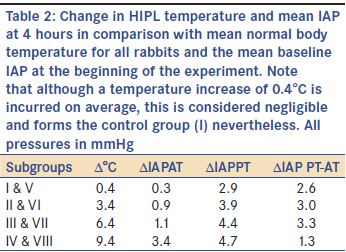
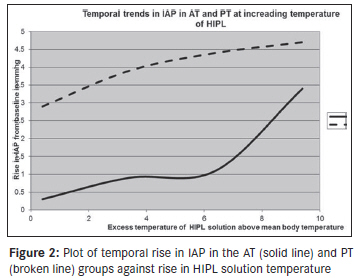
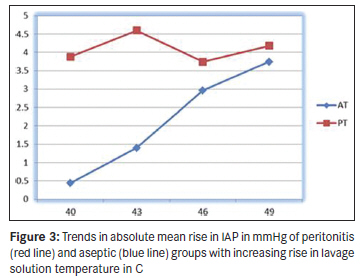
Keywords: Abdominal compartment syndrome, damage-control surgery, hyperthermic intraoperative peritoneal lavage, intra-abdominal hypertension, peritonitis Introduction Damage-control surgery (DCS) by laparotomy in septic complications of blunt or penetrating abdominal injury is associated with high complication rates in major trauma. Acidosis, coagulopathy, and hypothermia, the aptly termed "lethal triad," sustain the poor outcomes associated with these injuries. Timely intervention is life-saving. Copious lavage of the peritoneum with crystalloid solutions, a common surgical practice whose benefit is increasingly questioned in some quarters, at slightly above the normal body temperature (hyperthermic intraoperative peritoneal lavage [HIPL]) is believed to decontaminate the peritoneum and reverses or prevents hypothermia. [1],[2] In the heat of the moment in such situations, use of irrigating fluids at lower than normal body temperatures is not unlikely and could put the patient at risk of hypothermia or hyperthermia with all the detrimental consequences to the patient. In an earlier study, [3] we demonstrated that using the gloved hand as a thermal sensor to judge the temperature of irrigating fluids has low accuracy and could predispose patients to peritoneal lavage with solutions at temperatures that are associated with complications of temperature extremes. What are the consequences of using solutions at higher temperatures in patients undergoing HIPL for abdominal trauma with or without peritonitis? Aim To determine the body weights, normal body temperature, baseline intra-abdominal pressure (IAP), and the effects of HIPL at graded temperatures above the normal temperature in groups of rabbits with/out peritonitis. Materials and Methods This study was designed as a randomized, controlled, and blinded experimental interventional study. The primary objective of the study was to determine the relationship of the mean absolute rise in IAP at corresponding temperatures of HIPL at the furthest point in time, with all the animals still alive. Secondary objectives include the highest absolute rise in IAP and survival after 12 hours. A total of 63 rabbits were procured for this study. Eighteen rabbits from which data were not used for this study were utilized for the standardization of the operative procedures and measurements according to the study protocol. Similarly, no data were collected from another group of five rabbits which were used as sources of fecal matter to induce peritonitis in the 20 rabbits that formed the thermal-peritonitis (PT) group. Thus, only the data from the last 40 rabbits were used for the study. The approval of the institutional review board was obtained for this study. All the animals were treated according to the Helsinki Accord. The animals were fed liberally with dry food pellets along with lettuces, cabbages, and water for at least five days prior to the morning of the experiment when no food or water was given to them. Each animal was weighed using an electronic weighing scale (Salter 1020, HoMedics, USA). The body temperature was taken through the rectum using a digital rectal thermometer (California Veterinary Supply, USA) with a sensitivity of 0.1°C. The data were collected and recorded. Twenty rabbits were randomly assigned to the aseptic-thermal (AT) group and the other 20 to the peritonitis-thermal (PT) group. The AT group were animals that underwent laparotomy and peritoneal lavage with aseptic technique to minimize peritoneal contamination, while the PT group had peritonitis induced by the deliberate contamination of the peritoneum with freshly collected colon fecal matter from a donor rabbit and closed, and subsequently followed by HIPL after one hour. In each group, the animals were further subdivided into four subgroups of five rabbits numbered with Roman numerals in consecutive order: I AT40 , II AT43 , III AT46 , and IV AT49 corresponding to a peritoneal lavage solution at temperatures of 40°C, 43°C, 46°C, and 49°C. Similarly, the rabbits in the PT group were labeled V PT40 , VI PT43 , VII PT46 , and VIII PT49, corresponding to solutions at 40°C, 43°C, 46°C, and 49°C. Saline was warmed in a water bath and brought to the desired temperature for each group using a long-range thermometer (Brannan Co, UK). The abdominal wall of each rabbit was cleaned with povidone iodine and shaved. General anesthesia was induced by intramuscular administration of ketamine at a dose of 10 mg/kg followed by intramuscular administration of promethazine at a dose of 6 mg/kg and by infiltration of Bupivacaine at a dose of 1 mg/kg along the line of proposed incision to obtain long-term analgesia on the incision. A peritoneal balloon pouch was created and connected to a short segment of size 10 Nelaton′s catheter and brought out through a stab wound on the abdominal wall and secured to the skin by sutures. The laparotomy wound was then closed in a single layer with silk 2/0 sutures. The balloon pouch was then connected to a T-tube manometer through the intervening Nelaton′s catheter. The IAP was then measured by reading the resting level of the meniscus with the zero level corresponding to the middle of the abdomen with the animal lying on its side. The reading was initially recorded in centimeters of water and then the values subsequently converted to millimeters of mercury. After one hour, the abdomen was reopened. The peritoneal cavity was lavaged with saline at a temperature corresponding to the animal′s group temperature at a volume of 100 ml/kg for two minutes. After this, the lavage fluid was removed by dabbing the peritoneal surface with absorbent gauze pieces. The laparotomy was then resutured. Subsequently, the IAP was measured hourly by two independent observers blinded to each other, and the average of the two readings was recorded by a third observer. The data were collected for a total of 12 hours or until the animal died, whichever came first. This is the protocol followed for animals in the AT group (subgroups I-IV). For the animals in group PT (subgroups V-VIII), the experiment was identical with the following important difference: after the first reading of IAP, 5 ml of rabbit fecal solution from the five rabbits earlier mentioned was instilled into the peritoneum. The laparotomy was closed. At the next hour, the laparotomy was opened and HIPL was performed as described in the previous group. Thereafter, the reading of the IAP continued until the animal died. If the animal died earlier than 30 minutes after the last reading, the death was ascribed to the preceding hour, but if death occurred after 30 minutes, the death was ascribed to the next hour. All surviving animals were euthanized at the end of the operation. Statistical analysis of all data collected was with the Number Cruncher Statistical Software, NCSS 2007. Results The weights of the 40 rabbits [Table - 1] ranged from 662 to 1 978 g (Mean = 1 333 g, 95% CL = 1 225-1 441 g). The body temperature [Table - 1] ranged from 38.4°C to 40.4°C (Mean = 39.6°C, 95% CL = 39.4°C -39.7°C). The baseline IAP [Table - 1] ranged from 4.0 to 5.5 mmHg (Mean = 4.8 mmHg, 95% CL = 4.7 to 4.9 mmHg). [Figure - 1] shows the temporal trend in the IAP in all eight subgroups for the duration of survival up to the end of 12 hours for those that survived that far. Group I AT40 with HIPL at 40°C as against the mean body temperature of 39.6°C for the whole population sample was the control subgroup against which all the other seven subgroups were compared. The net rise in mean IAP [Table - 2] for each subgroup from the baseline was 0.3, 0.9, 1.1, and 3.4 mmHg for subgroups I AT40 , II AT43 , III AT46 , and IV AT49, respectively. The corresponding value was 2.9, 3.9, 4.4, and 4.7 mmHg, respectively, for groups V PT40 , VI PT43 , VII PT46 , and VIII PT49 . The difference in the means of I AT40 and II AT43 using the two sample t test was not significant (t = 0.1849, P = 0.85). However, when compared with III AT46 and IV AT49 , the control group (I AT40 ) showed significant difference (t = 3.9951, P < 0.001 [with III < 0.001 [with III AT46 ] and t = 5.5356, P < 0.0001 [with IV < 0.0001 [with IV AT49 ]). In comparison with subgroups in the PT group, the control group revealed statistical significance: with V PT40 (t = 4.9531, P < 0.0001), VI PT43 (t = 4.017, P < 0.001), VII < 0.001), VII PT46 (t = 4.4219, P < 0.001), and VIII < 0.001), and VIII PT49 (t = 3.8857, P < 0.01). Comparison of mean IAP at equivalent levels of HIPL temperature between the groups showed I AT40 vs V PT40 (t = 4.9531, P < 0.0001), II < 0.0001), II AT43 vs VI PT43 (t = 3.9070, P < 0.001), III < 0.001), III AT46 vs VII PT46 (t = 2.5119, P < 0.05). However, IV < 0.05). However, IV AT49 vs VIII PT49 showed no significance (t = 0.4762, P = 0.64). From [Table - 1], we selected the IAP at 4 hours as a basis for comparison, since all 40 rabbits survived up to this point. Employing multiple linear regression analysis, we found a positive correlation of all subgroup mean IAPs at 4 hours with increasing temperatures [Figure - 2]. The correlation coefficients (r) were 0.85 (AT) and 0.89 (PT), respectively. The coefficients of determination (r 2 ) were 0.73 (AT) and 0.8 (PT). Using these values, we calculated correlation equations that would predict the IAP with HIPL solutions at known temperatures within the range of 40°C and 49°C. These are presented mathematically as: Y = 5.1 + 0.2283 (T-40) for group AT Y = 6.3 + 0.2393 (T-40) for group PT Where, Y is the predicted IAP and T is the temperature of the HIPL solution between 40°C and 49°C. With regards to the secondary objectives, 100% survived for 11 hours and 90% were alive at the end of the experiment in the AT group. [Figure - 3] shows the mean rise in IAP from the baseline to the highest value attained over time. Although the AT group survived longer, the PT group all died at the fourth hour. Although the PT group attained higher mean rise in IAP compared with AT group, this was attained earlier by the fourth hour. It can be noted in [Table - 1] and in [Figure - 1] that although most animals in AT attained their highest IAP and gradually returned to lower values including the two animals that died at the 11 hour, in the PT group, death occurred at the highest IAP attained without a downward return as in AT. Discussion We demonstrated the consequence of high temperature of the HIPL solution on IAP and survival by showing the direct relationship between the temperature of the HIPL greater than the normal body temperature and the IAP rise. Up to 3°C HIPL did not show significant rise in IAP in the absence of peritonitis. Beyond 3°C and in the presence of peritonitis, however, HIPL proved to be detrimental with rapid rise in IAP and death, all manifesting earlier. At temperatures beyond 3°C, both heat and sepsis are associated with increasing morbidity. Our observation that no significant difference existed between IV AT49 versus VIII PT49 initially took us by surprise until we understood that at that temperature hyperthermia was by itself sufficiently lethal to the animal even in the absence of peritonitis. This qualitative Qualitative differences are revealed in [Table - 1] and [Figure - 1], where the animals in subgroup VIII PT49 not only attained higher IAPs on a time scale, but died much faster in comparison with subgroup IV AT49 . At equivalent temperatures, the mean value of IAP was higher in the PT group. This suggests that thermal insult has synergistic effect to sepsis-induced IAH. The abdominal cavity in man normally subtends a pressure of about 5 to 6 mmHg in health. This IAP may transiently rise above this level during normal activities of living, such as coughing, laughing, straining at micturition, or during defecation without any demonstrable pathologic effects. A sustained pressure above 12 mmHg is regarded as intra-abdominal hypertension (IAH) and is associated with subclinical organ dysfunction. Above 20 mmHg, abdominal compartment syndrome (ACS) can be predicted. [4] Peritonitis as a cause of ACS dictates laparotomy (unless laparoscopy is an option). Definitive treatment incorporates peritoneal lavage using copious amounts of normal saline to wash out pus and particulate matter to reduce bacterial and endotoxin load. In critically ill patients, the danger of inducing hypothermia through thermal diffusion by the infusion of saline at less than the normal body temperature is real and explains why surgeons have traditionally employed "warm saline" for this purpose. Compromised mesenteric blood supply caused by trauma, strangulation in a hernial sac, and thromboembolism are among reasons surgeons employ HIPL or "warm compress" on the segment of bowel to encourage blood flow where intestinal viability is equivocal in order to facilitate the decision to salvage or to sacrifice the segment bowel. During DCS in established peritonitis and when hypothermia resulting from hemorrhagic shock, resuscitation with large volumes of intravenous fluids at subnormal temperatures or environment-induced thermal loss also coexists; HIPL, at above the normal body temperature, serves the dual purposes of peritoneal decontamination and reversal of hypothermia. This is a standard procedure practiced by most surgeons. [5],[6],[7] Thermal stimuli transmitted as neural signals produce vasoconstriction at lower temperatures and vasodilation at higher temperatures than the normal body temperature. Vasodilation induces the capillaries to become hyperpermeable, resulting in the accumulation of interstitial fluids (edema), thereby increasing the size (weight and volume) of the organs involved. Outside a narrow temperature range beyond 37°C, the effect of the temperature of HIPL solution on local and remote systems is not entirely known. This situation is mitigated by is so because of the difficulty in conducting ethical human studies with the deliberate use of HIPL solutions at considerably colder or hotter temperatures, as may theoretically occur unintentionally by human error. In our previous study, [3] we found that of a total of 480 attempts, surgeons and nurses were able to accurately predict the temperature of warm saline they had prepared with their gloved hands and considered suitable to use in HIPL for peritonitis in only 40% of instances. More worrisome is the fact that in 15% of the instances, the simulated scenario would have resulted in HIPL at temperatures in excess of 41°C (hyperthermic for our purpose). Conversely, in 41% of the instances, the patients would have been exposed to solutions below 37°C (hypothermic for our purpose). We concluded that the gloved hand, which is the de facto instrument for determining the temperature of saline for HIPL in our institution, is grossly inaccurate and should not be relied upon for this purpose. To ensure that after thermal dilution, the patient is protected from (or treated for) hypothermia coexistent with anesthesia-induced poikilothermia, we recommended performing HIPL with temperatures between 38°C and 39°C. Hypothermia is associated with peripheral vasoconstriction leading to increased afterload producing increased cardiac work and oxygen demand, cardiac arrhythmias due to myocardial membrane instability, wound infection, impaired collagen deposition in the wound, and coagulopathy. [8],[9],[10],[11] Hyperthermia is associated with coagulopathy (thrombocytopenia, increased fibrin degradation products, prolonged clotting times, and spontaneous bleeding), dysfunction of the immune system (lymphopenia, suppression of circulating macrophages, and complement-mediated/cortisol-induced T-cell suppression). [12],[13],[14] We have observed [unpublished] the omentum increasing in thickness by several factors after copious HIPL in cases of peritonitis, a fact we attributed to vasodilatation and visceral edema. These results cannot be validly extrapolated to human subjects because the normal body temperature in human beings is almost 3°C lower than in the rabbits used. Although smaller in size than our species, the baseline IAP of these rabbits is remarkably similar to human beings. [4] The temporal trend of this observation as opposed to absolute values is key and may very well be operational in human subjects and applicable to clinical situations. This should be a reason for concern and should inspire human studies to compare with our observation. Until such studies contradict our findings, we would urge emergency and trauma surgeons who manage patients in the setting of DCS to pay attention to these findings in the light of our previous study. [3] No price or labor should be considered too much to pay for ensuring that the measurement of HIPL solutions is accurate and precise. Our finding suggests that the use of HIPL at temperatures up to 3°C above the normal body temperature of rabbits is safe. It may be inferred that subject to valid conclusions from appropriate human studies, it may be prudent to use irrigating fluids at a point slightly higher than 37°C for HIPL in human beings to take account of thermal dilution and can justifiably be used to correct or prevent hypothermia from causes mentioned earlier. Fluid warmers and baths equipped with thermostats that can readily provide irrigation fluids without breaking the sterility barrier at precise temperatures slightly above the normal body temperature are recommended and will go a long way to prevent both hypothermia and IAH in patients undergoing laparotomy in the setting of DCS with or without peritonitis. Conclusion We conclude that independently, HIPL at temperatures greater than 3°C in the rabbit significantly raises the IAP proportionate to the temperature of the irrigating fluid. In the presence of peritonitis, the observed effect is even more pronounced and is associated with mortality and shorter postoperative survival due to ACS. Acknowledgement The authors hereby acknowledge, with gratitude, the contribution of Dr. Narcisse Ndoumbe for the French translation of the abstract. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11047f3.jpg] [am11047t1.jpg] [am11047f1.jpg] [am11047t2.jpg] [am11047f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}