 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
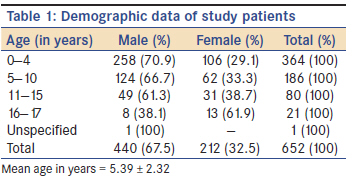
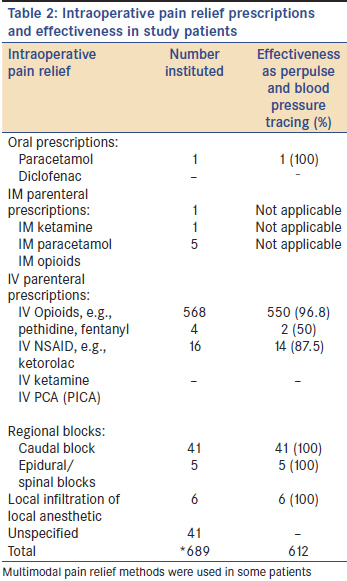
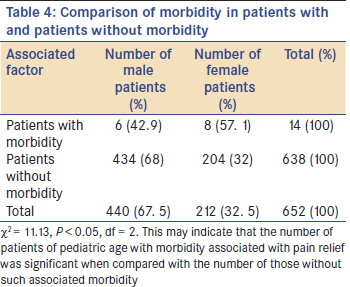
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 233-237 Original Article Trends in intraoperative pain relief in anesthesized Nigerian pediatric patients: Implications for a developing economy OP Adudu1, I Isa2, FO Longway2 1 Department of Anaesthesiology, College of Medical Sciences, University of Benin, Benin City, Nigeria Code Number: am11048 PMID: 21912009 Abstract Background : New drugs and new modalities for intraoperative pain relief is the current trend in pain management. Keywords: Intraoperative period, pain relief, trends Introduction Acute pain management for surgical patients intra and postoperatively is important for patient comfort. It leads to an improved perioperative experience and reduction in pulmonary complications. [1],[2] This results in reduced hospital costs due to shorter hospital stay especially in ambulatory surgical patients. [3],[4] Currently available are new drugs for intraoperative pain relief such as remifentanil [5] and the use of new modes of pain relief such as the administration of systemic local anesthetics such as lignocaine which has antiinflammatory modulatory properties. [6] Also, there is new sophistry in prescription orders in administering analgesia such as parent controlled analgesia [7] and automated anesthesia information management systems. [8] These have led to prompt, safe, and effective intraoperative pain management worldwide. Computerized physician order of prescriptions [9] and patient clinical information are a part of automated anesthesia information management systems. Furthermore, the utilization of acute pain service facilities has ensured that the gains of effective intraoperative pain management continued into the postoperative period for surgical patients. [10] The new modalities for acute pain management are not available in the sub-region including organized acute pain service. [11] The study therefore set out to examine the intraoperative pain relief practices in our centre, UBTH, in Nigeria. An organized acute pain service for pediatric surgical patients can be developed within the limits of available manpower and technology in Nigeria. This study therefore focuses on the trends in intraoperative analgesia in anesthesized children and its implications for a developing economy such as ours. Materials and Methods The retrospective cohort study of pediatric surgical patients on trends in their intraoperative analgesia was carried out in UBTH from January 2006 to June 2008. The anesthetic charts and case notes of the pediatric surgical patients were selected and examined. The pediatric age used for the study was the legal definition of 17 years and below. Demographic data, method of intraoperative pain relief used, associated morbidity and complications, surgical procedure, and anesthetic management including technique were documented. Data were subjected to statistical tests using the Statistical Package for Social Sciences (SPSS) with the level of significance set at 0.05. Results Six hundred and fifty two surgical patients of age 0-17 years were studied. They include 440 males (67.5%) and 212 females (32.5%). The mean age of the pediatric surgical patients was 5.39 ± 2.32 years [Table - 1]. The surgical procedures carried out in the 652 pediatric patients in the study was a total of 670 and include herniotomies (106 i.e. 15.8%), plastic and orthopedic surgery (107 i.e. 16.0%), excisions including biopsies (81 i.e. 12.1%), appendisectomies (62 i.e. 9.3%), urethroplasties, nephrectomies, and pyeloplasty (54 i.e. 8.1%), ear, nose, and throat surgery (44 i.e. 6.6%), maxillofacial surgery including cleft lip (40 i.e. 6.0%), colostomies including closures (27 i.e. 4.0%), cardiothoracic surgeries including oesophagoscopies (18 i.e. 2.7%), neurosurgeries including neurodiagnostic procedures such as CT scans (31 i.e. 4.6%), laryngoscopies, and foreign body removal (13 i.e.1.9%), skin graft (18 i.e. 2.7%), omphalocoele repair (14 i.e. 2.0%), anoplasty (15 i.e. 2.2%), and unspecified surgeries (40 i.e. 6.0%). Multiple surgical procedures was carried out in some patients. The pain relief methods used in the intraoperative period for the study patients were mainly parenteral opioids (573 i.e. 87.9%) and regional blocks mainly caudal blocks (46 i.e. 7.1%) [Table - 2]. The other methods of pain relief used include parenteral ketamine (17 i.e. 2.6%), ketorolac (4 i.e. 0.6%), local infiltration using 1% lignocaine and 0.25% bupivacaine (6 i.e. 0.9%), and oral and parenteral paracetamol (2 i.e. 0.3%). Multimodal methods of pain relief were used in some patients. There was no evidence of the use of infusion pumps for pain relief or of the use of computerized orders for physician prescriptions. There were no automated anesthesia information management systems (AIMS) for use for pain relief in pediatric surgical patients. The morbidities associated with modalities of pain relief used were found to be significant in 14 patients (2.1%) and are as shown in [Table - 3] and [Table - 4] (χ2 = 11.13, P < 0.05, df = 2). The anesthetic technique used was mainly general anesthesia in 650 patients (99.6%) which includes the concomitant use of regional analgesia in 46 patients which had to be established under general anesthesia in young pediatric patients, and, two solely spinal anesthetic technique in two older children (0.31%). Discussion The current trend in intraoperative pain relief in the pediatric patients studied revealed that parenteral methods were still the mainstay of acute pain management. However, there is a paradigm shift from the use of intramuscular route [12] to the use of intravenous route (87.9%) for analgesic drug administration. Furthermore, we found an increase in the use of regional blocks mainly caudal blocks for acute pain management in these patients. [10] The drugs used have remained old conventional opioids. [13] This trend in the study lags behind the current worldwide trend of new sophistry in the use of new generation drugs such as remifentanil and new modalities for drug administration including infusion pumps and controlled analgesia machines by patients (older children), parents (especially in children with disabilities) and nurses. The new use of intravenous lignocaine, [6] and fascia iliaca nerve blocks [14] for pain relief is also of current interest. [6] In addition, the trend for improved safety of drug administration using computerized systems reduces medical errors in drug administration. [15] The implication of establishing the current trend for intraoperative pain relief in pediatric patients is enormous costs in terms of equipment, drugs and facilities to be used. It is however, cost effective as it improves socioeconomic life. Also, the training of physician personnel, pharmacists, and nurses on information technology is essential for the development of a modern intraoperative pain management. The finding in the study that the use of regional blocks which is an area of current focus in acute pain management, is low, is worrisome. The increased use of regional blocks for intraoperative pain relief reduces the incidence of side effects of drugs used in the conventional methods of pain relief with decreased morbidity and shorter hospital stay. It has important implications as an incidence in morbidity of 2.1% was found to be significantly associated with the pain relief methods used in the study (c2 = 11.13, P < 0.05, df = 2). Anesthetists need to be encouraged to use regional blocks for the safety and improved outcome in patients. The limitations of the study include incomplete data especially on the rescue interventions made in the course of management of morbidity associated with intraoperative pain relief. It does not however diminish our findings in the study that intraoperative pain relief (acute pain management) in anesthesized pediatric patients were mainly parenteral methods although the mode had shifted from intramuscular to intravenous drug administration of old conventional opioids. Conclusion Current intraoperative pain relief practices were mainly conventional old generation opioid drugs such as pethidine, fentanyl, etc. administered intravenously. Also, old generation local anesthetic drugs such as bupivacaine were administered in the caudal and subarachnoid spaces. New opioid drugs such as remifentanil, new local anesthetics such as ropivacaine and new modes of drug delivery of analgesic drugs such as controlled analgesia machines by patients, parents and nurses via intravenous and epidural routes were not used. The implications of this lagging behind trend found in our study for the development of an efficacious and cost-effective intraoperative pain relief for pediatric patients is enormous in terms of costs for equipment, drugs, facilities, and personnel development. Its benefits of safety, improved outcome, reduced hospital stay, and improved socioeconomic life with less disruption of family and school life outweighs its high cost. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11048t2.jpg] [am11048t1.jpg] [am11048t4.jpg] [am11048t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}