 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
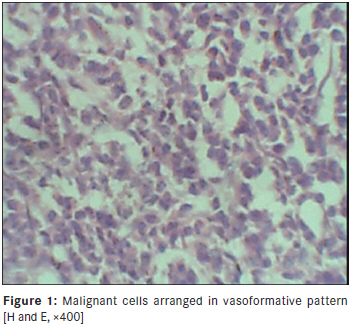
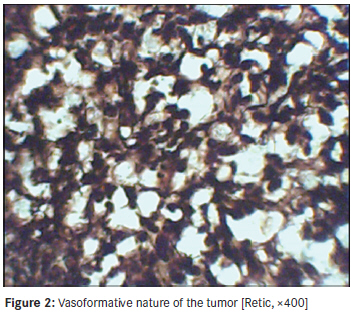
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 246-248 Case Report Angiosarcoma of the small intestine A Mohammed, HO Aliyu, AA Liman, K Abdullahi, N Abubakar Department of Pathology, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria Code Number: am11051 PMID: 21912012 Abstract Primary gastrointestinal angiosarcomas are very rare and those of the small bowel even more rare. We report a case which is the first in the literature from this part of the world. It presented in a 25-year-old woman with multiple dissemination and rapid fatality. Diagnosis was based on histological morphology using Hematoxylin and Eosin (H and E) stains, plus reticulin special stain to outline the vascular nature. Keywords: Angiosarcoma, small intestine, rare Introduction Primary gastrointestinal (GIT) angiosarcomas are very rare [1],[2] and those of the small bowel even more rare. [1],[3] A few reported cases suggest that angiosarcomas of the small intestine may occur at sites of previous irradiation therapy and may be causally related. [2],[3] The tumor manifests as nonspecific symptoms such as gastrointestinal bleeding, abdominal pain, abdominal distension, weight loss, shortness of breath and weakness from anemia. [1],[2],[3],[4] It is one condition in which upper and lower endoscopies usually do not demonstrate any lesions. [1],[2],[4],[5] This tumor is characteristically multiple and it is recognized by an anastomosing proliferation of atypical endothelial cells. [1],[5] Immunohistochemical demonstration of CD31, and less consistently the vonWillebrand factor is diagnostically useful. [1] Treatment generally consists of surgery, sometimes followed by neoadjuvant chemotherapy. [1],[6] The diagnosis is often made at an advanced stage and this makes for a bad prognosis. [1],[6] Most cases progress rapidly with a two-month median survival after diagnosis. [5] Case Report We report a case of a 25-year-old woman who presented with a four-week history of intermittent abdominal pain, weight loss and progressive abdominal distension, a seven-week history of shortness of breath, hematemesis and malena. Her medical history included a peptic ulcer disease. On physical examination, she was pale, dyspneic with features of left-sided pleural effusion, gross ascites and multiple, firm, nodular intra-abdominal masses involving the large and small bowel area. A chest tube was inserted into the left pleural cavity and drained 900 ml of straw-colored fluid over 48 h. Hematological tests showed a microcytic hypochromic anemia (Hb-7.3 g/dl) with monocytosis (18.1%) and raised hepatic enzymes, ALT-47 IU/L (range 16-40 IU/L); AST-69 IU/L (range 5-22 IU/L). The patient′s status for HIV 1 and HIV 2 was negative. Ultrasonography revealed moderate ascites, and multiple solid masses involving the large and small bowels. The liver, spleen, rectum, urinary bladder, kidneys, uterus and its adnexae were all normal. The patient was resuscitated and optimized for an exploratory laparotomy that revealed 3.5 L of straw-colored ascitic fluid, flimsy adhesions, widespread, variably sided, firm to hard tumors with contact bleeding studding the surface of the small and large bowel, omentum, pelvic walls and pouch of Douglas. The largest was on the small bowel and measured about 14 × 10 cm, while only two tiny lesions were present on the large bowel, with the largest measuring 5 mm in its widest dimension. Other internal organs appeared grossly normal except for slightly edematous fallopian tubes. Two of the lesions were biopsied from the ileal surface. Histopathologic analysis revealed a tumor composed of sheets of polygonal cells having hyperchromatic nuclei with an irregular coarse chromatin pattern and moderate amphophilic cytoplasm forming highly anastomosing channels of varying size and shape, some of which contained red blood cells. Both solid and vasoformative areas were noted, including areas of extensive tumor necrosis [Figure - 1]. A reticulin stain was also done, further confirming the vascular nature of the tumor [Figure - 2]. A morphologic diagnosis of malignant hemangioendothelioma was made. The patient deteriorated in the second week following surgery and died on the 11 th postoperative day. Postmortem examination could not be done. Discussion Angiosarcoma of the small bowel is usually a high-grade malignancy and very elusive to routine endoscopic detection. [1],[2],[4],[5] So the wide spread of nature the tumor would not have been prevented by our routine gastrointestinal examinations. Computerized tomographic (CT) scan would have been helpful in early detection if routinely done in otherwise healthy individuals in most environments. Such inadequacy could be contributory to the late presentation and fatal outcome. The possibility of using CT scan for routine examination is currently not feasible due to financial constraints. However, it can be recommended in individuals in the high-risk group for developing GIT angiosarcomas. This patient had no antecedent history of radiation to the abdominal region, nor other etiological risk factors reported in the literature. [1],[2],[4],[5],[6] We believe that this is the first case of angiosarcoma of the small bowel to be reported from this part of the world. Data from the archives of the Armed Forces Institute of Pathology (AFIP), United States of America, report a series of 366 cases out of which the commonest site of the tumor was the skin (33%) followed by the soft tissues (24%). It was least common in the heart and orbit (3% each). No occurrence in the small bowel or the gastrointestinal tract has been reported. This further buttresses the rarity of this tumor in this site. [7] In conclusion, the diagnosis of angiosarcoma of the gastrointestinal tract is a challenge, especially in a resource-poor setting. Attempts at early diagnosis can include CT scan in individuals with known risk factors for this tumor, especially immunosuppressed patients or those exposed to irradiation. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11051f2.jpg] [am11051f1.jpg] |
| |||||||||

{kind=link}
{kind=link}