 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
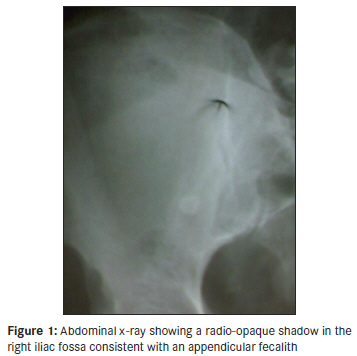
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 249-251 Case Report Perforated appendicitis in a septuagenarian Robert B Sanda, Salah I Seliem, Elrasheed Omar, Syed Ashraf Department of Surgery, Drumheller Hospital, Drumheller AB, T0J 0Y1, Canada Code Number: am11052 PMID: 21912013 Abstract Appendicitis in the elderly is becoming an increasingly frequent clinical encounter due to the increased life expectancy in the human race over the last half-century. Appendicitis in this age group has, therefore, become relatively more common with an atypical presentation that incurs delay in diagnosis with attendant morbidity and mortality. We present a septuagenarian who presented atypically with a rapidly progressing feature of appendicitis that emphasizes the need for early operative intervention. In addition, the patient presented with other comorbidities that could detract from a diagnosis of appendicitis to the unwary. Keywords: Appendectomy, appendicitis, elderly, peritonitiss Introduction The increased life expectancy that came about during the late 20 th and the first decade of the 21 st centuries has compelled surgeons and physicians to undertake medical procedures in increasingly older patients. The most common emergent surgical operation, appendicitis, previously regarded as a pediatric operation, is increasingly being seen in older patients. The geriatric patient with appendicitis, however, presents remarkably differently from his pediatric counterpart, largely due to the changes in the body′s physiologic reserves and disease manifestation. Thus, stereotyping of the presentations of appendicitis could put elderly patients presenting with it at risk of morbidity and delayed implementation of treatment due to delay in making the diagnosis. Aim We present a case of appendicitis in a patient in his eight decade, which illustrates the atypical presentation and the rapid evolution of the disease in this age group. Case Report A 75-years-old man presented to our hospital complaining of abdominal pain and fever all of 12-hour duration. The pain began suddenly around the right iliac fossa and was nonmigratory and constant. Within four hours, he developed fever with chills and rigors. There was no history of nausea, vomiting, or altered bowel habits. He had Parkinson′s disease for two years and was on Trihexyphenidyl (Artane® ) and Propranolol (Inderal® ). On examination, the patient was lying still and was mildly febrile (T = 37.8°C). Other vital signs were: Pulse = 93/ min; BP = 134/68 mmHg; and RR = 16/ minute. There was tenderness over a wide area of the right lower abdominal quadrant with guarding, rebound tenderness and a positive Rovsing′s sign. The bowel sounds were subdued. Examination of the central nervous system revealed intact sensorium and cognition. Resting tremor of the hands and cog-wheel rigidity at the wrists was noted. There were joint stiffness involving the hips, the knees, and the ankle joints. A provisional diagnosis of localized peritonitis due to bowel perforation in the vicinity of the cecum, appendix, and terminal ileum with Parkinson′s disease and multi-joint osteoarthritis was made. Laboratory examination revealed a total leukocyte count of 10.4 × 10 9 /l with elevated neutrophils (85%). X-ray of the abdomen showed a normal gas pattern, bone, and soft tissues. A rounded radio-opaque shadow was evident in the right iliac fossa that was suggestive of an appendicular fecalith [Figure - 1]. There was no free air under the diaphragm. Electrocardiography showed evidence of mild left ventricular hypertrophy.Within one hour of presentation to the hospital general anaesthesia was induced to commence the operation. At operation, the findings were a markedly inflamed appendix with involvement of the wall of the cecum. The appendix was perforated at the base with contamination of the peritoneum over a wide area [Figure - 2]. Appendectomy was done and the fecalith was identified [Figure - 3]. A peritoneal swab subsequently tested positive to Escherichia coli, sensitive to all the 21 antibiotics against which it was tested including the three the patient was taking. Wound closure was by a delayed primary closure over a closed drainage system. Recovery was uncomplicated. Discussion Increased life-expectancy in the late 20 th century has brought with it an increased demand for abdominal operations among the elderly, including appendectomy. [1] Appendicitis is a difficult diagnosis to make with certainty in this age group and carries unacceptably high complication and mortality rates. [2] In an observational study from Finland of operative interventions for nonvascular acute abdomen among 201 elderly patients aged 65 years and over between 1986 and 1989, Kettunen et al. found appendectomy accounting for 20% of their operations. [3] These authors also observed a 44% mortality rate following appendectomy among the patients that were older than 80 years. In these patients, 64% were risk-categorized into American Society of Anaesthesiologists class IV or V at admission. The morbidity and mortality rate in another elderly population from the USA were estimated at 31% and 20%, respectively. [4] The difficulty in establishing the diagnosis early can be attributed to several factors. Elderly patients tend to seek help relatively late from the onset of symptoms. [5],[6] When they do, in a sizable proportion, the presenting features are atypical. [7],[8],[9] Clinical and laboratory features of inflammation like pain, vomiting, and leukocytosis may be greatly attenuated, presumably due to an ageing immune and neural systems. Our patient presented with nonmigratory pain without vomiting and with just borderline leukocytosis, despite having a perforated appendicitis with localized peritonitis. Even though our patient presented early (and there was no delay in carrying out the operation), the appendix was already perforated by the time of operation. It has been suggested that due to the atrophy of the wall of the appendix and due to the involution of the gut-associated lymphoid systems, the appendix tends to perforate relatively early in this age group. [10] For this reason, appendectomy should not be delayed in the elderly. [11] Comorbid conditions often vie for consideration in the differential diagnosis and may be a factor for consideration in general anesthesia. [3] We had no doubt about the diagnosis of appendicitis in this patient when he presented because the clinical findings were strongly supported by the presence of a radio-opaque shadow in the abdominal x-ray that suggested an appendicular fecalith. When in doubt, Ultrasonography and Computerized Tomographic (CT) scans are helpful in establishing the diagnosis or in ruling it out. [12] Laparoscopic appendectomy has been found to have several advantages in a large study population in the USA. [13] In this nationwide large sample, elderly patients who underwent laparoscopic or open appendectomy between 1998 and 2000 were compared in terms of length of hospital stay, rate of routine discharge, and in-hospital morbidity and mortality rates. The results revealed a significant outcome benefit for the laparoscopic group as compared with the open appendectomy group. Similar observations were made in a prospective study from Taiwan but admittedly with a smaller patient population. [14] On the contrary, others have observed no statistically significant differences among a population of elderly patients who underwent appendectomy by laparoscopy aided by preoperative CT scan in terms of measurable outcomes like morbidity and mortality. [15] It would be rational to recommend that although CT and laparoscopy remain useful diagnostic tools, good clinical acumen and a low threshold for operative intervention should be the goal all in elderly patients presenting with features suggestive of appendicitis. Acknowledgement The authors hereby acknowledge, with gratitude, the contribution of Dr. Narcisse Ndoumbe for providing the French translation of the abstract. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11052f3.jpg] [am11052f1.jpg] [am11052f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}