 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
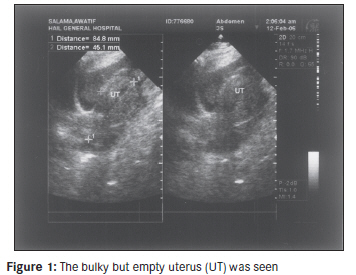
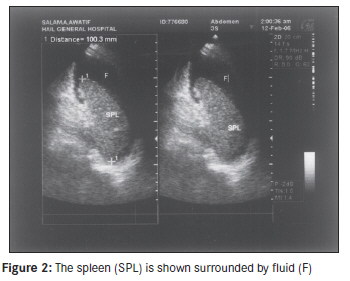
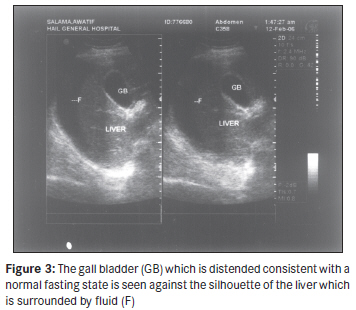
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 252-255 Case Report Abdominal Compartment Syndrome complicating massive hemorrhage from an unusual presentation of ruptured ectopic pregnancy Robert B Sanda1, Rafeeqa Aziz2, Abdulrazaque Bhutto3, Salah I Seliem1 1 Department of Surgery, Hail General Hospital, Hail 81451, Saudi Arabia, Code Number: am11053 PMID: 21912014 Abstract Abdominal Compartment Syndrome (ACS) is characterized by intra-abdominal hypertension (IAH), elevation and splinting of the diaphragm, high pleural pressure, and poor venous return to the heart, producing low cardiac output and shock which, in turn, results in poor venous return across the capillaries to set in a vicious cycle. Unless the Intra-abdominal pressure is reduced quickly by urgent surgical or medical interventions, death is inevitable. We report a case of ACS resulting from an unrecognized slow but massive intra-abdominal bleeding caused by a ruptured ectopic pregnancy (REP) in an Arab woman. Due to the unusual nature of the presentation of the REP, the diagnosis proved elusive for over a week until the patient succumbed to hypovolemic shock after losing about 4.2 l inside the peritoneal space. The fruitless effort at aggressive fluid resuscitation was at operation found not due to hypovolemia per se but due to IAH causing ACS. The lessons learned from this case emphasize the need for awareness about atypical presentations of REP and the need for quick intervention to terminate the vicious cycle of ACS. Keywords: Abdominal Compartment Syndrome, hemorrhage, intra-abdominal hypertension, intra-abdominal pressure, ruptured ectopic pregnancy, shock Introduction On any given day, ruptured ectopic pregnancy (REP) is an easy diagnosis. It can, on rare occasions, be a diagnostic challenge and under-reported. In the absence of a high index of suspicion and zealous adherence to the dictum, every woman of reproductive age is pregnant until proved otherwise; victims of REP will be condemned to needless suffering and delay in commencement of treatment. The symptoms may be insidious, atypical, and protean. Abdominal Compartment Syndrome (ACS) is characterized by intra-abdominal hypertension (IAH), elevation and splinting of the diaphragm, high pleural pressure, and poor venous return to the heart, producing low cardiac output and shock which, in turn, results in poor venous return across the capillaries setting a vicious cycle. All the systems of the body are affected in this deadly pathophysiological conundrum. ACS has been classified into primary, secondary, and tertiary subtypes. Primary ACS occurs in disease or trauma within the abdominopelvic region such as blunt and penetrating trauma, hemorrhage from ruptured abdominal aortic aneurysm, and closure of the abdomen under tension postoperatively. Secondary ACS occurs in diseases remote from the abdomen, such as massive fluid resuscitation in burns and severe acute pancreatitis. Tertiary ACS defines the recurrent condition after a successful treatment of primary or secondary ACS. [1] Because ACS tends to occur in acutely ill patients with other dramatic symptoms that tend to distract, it is not an easy diagnosis to make. Case Report A 34-years-old woman was referred to us from a district general hospital in shock. Her vital signs were as follows: pulse = 132/ min, blood pressure (BP) = 80/40 mmHg, and respiration = 44/ min. She had a transfusion of blood and infusion of dopamine on-going as she arrived. She was restless, pale with a distended, tender abdomen. She was immediately rushed to the Intensive care unit where invasive monitors and resuscitation including mechanical ventilation was begun. Her Central venous pressure was zero cmH 2 O. After rapid infusion of 2 l of crystalloids, she remained in shock. The patient had presented to her primary care physician 12 days earlier complaining of epigastric pain, vomiting, and diarrhea. She was breastfeeding a 5-month-old infant and had not resumed menses since delivery. Routine Complete blood count showed her hemoglobin as 9.5 g/100 ml. She was treated for anemia and gastroenteritis. She returned 9 days later complaining that her epigastric pain and vomiting were persistent and in addition, she became tired easily. A repeat CBC found her hemoglobin level at 5.5 g/100 ml. She was admitted for further investigations and treatment. Three days into her admission, she suddenly collapsed with the following vital signs: pulse = 130/ min and systolic BP = 70 mmHg. She was referred to us by ambulance. On arrival, an urgent abdominal ultrasonography showed a large collection of free fluid in the abdomen. The uterus was slightly enlarged, but the cavity was empty. The adnexae could not be clearly-visualized [Figure - 1], [Figure - 2] and [Figure - 3]. Ultrasound-guided paracentesis abdominis yielded unclotted blood. The indication for paracentesis was to rule narrow down the diagnostic possibilities by eliminating a tense ascites from cardiac, renal, or portal hypertension. The general surgeon present consulted the gynecologist on-call who, unfortunately, was on her way into the operating room at that very moment to deliver a case of fetal distress by caesarean section. Immediate laparotomy was decided. The gynecologist agreed to join the general surgical team in the adjoining operating room as soon as it was feasible to do so. As soon as the patient was placed on the operating table, her BP was unrecordable but there was pulseless electrical activity. The decision to proceed with laparotomy was taken. Within 30 seconds of opening the peritoneal cavity, the patient′s BP rebounded to 105/60 mmHg without application of pressure on the abdominal aorta and without vasopressor drug administration or any significant fluid input. There was 4.8 l of blood in the abdomen. The cause of bleeding was found to be a ruptured right tubal pregnancy and a small vessel was still bleeding. A right salpingectomy was done and the abdomen was closed. On the sixth postoperative day, the patient was discharged home with a hemoglobin of 10.8 g/100 ml. She received six units of blood in total. Three months later, she was found to be in good health and has returned to her normal activities. Discussion Amenorrhea, lower abdominal pain, and vaginal bleeding with abdominal tenderness and rigidity are the usual presentations of REP. However, in about 50% of women, there is spotting at the time of their expected menses that mimics regular menses and so they do not realize that they are pregnant. [2] In about 25% of women, vaginal bleeding does not feature in REP. [3] Rarely, the finding of a negative β-HCG in REP may complicate matters. [4],[5] Rather than present with lower abdominal pain, this patient presented with epigastric pain leading her primary care physician to think she had gastritis. The pooling of blood in the pouch of Douglas can irritate the rectum and lead the patient to present with tenesmus, diarrhea, or even rectal bleeding. [6],[7] This was the case with our patient. Intra-abdominal pressure (IAP) measurement is to ACS what BP measurement is to hypertension. The normal IAP is between 6 and 12 mmHg. A sustained IAP above this range is pathological and is referred to as IAH. ACS occurs above IAP of 20 mmHg in the adult patient and surgical decompression is recommended as a life-saving procedure. The subtlety of presentation of ACS has mandated routine measurement of IAP monitoring in the ICU. Unfortunately, because the thought of ACS did not cross our minds until the operation was well underway, we did not afford ourselves the opportunity to measure her IAP. Despite the prolonged period of bleeding, this patient compensated very well until the last day of hospitalization in the referring hospital. Decompressive laparotomy reduces the IAP by relieving the tension exerted by the abdominal wall on the inferior vena cava and the portal vein to allow more blood to return to the heart. This explains the sudden normalization of the patient′s BP on cutting the abdomen open. Conversely, where closure of the abdomen following a laparotomy cannot be done without tension, it is recommended that delayed closure (staged abdominal repair) be undertaken to prevent IAH and ACS postoperatively. The algorithm for the management of ACS is still evolving. The treatment for ACS, however, has to be individualized according to the circumstances. There is a growing body of literature supporting a medical (conservative) management of ACS. Where bleeding, sepsis, and pancreatitis are the identified causes of ACS, most experts agree that a prompt surgical approach is the best option. Conclusion REP can present with atypical features in any woman of reproductive age, including the absence of history of pregnancy. IAH and ACS should be suspected in any patient with refractory shock and abdominal distension. Routine determination of IAP in critically ill patients will assist in early diagnosis and save lives. Acknowledgment The authors hereby express their gratitude to Dr. Narcisse Ndoumbe for translating the abstract into french. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11053f2.jpg] [am11053f3.jpg] [am11053f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}