 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
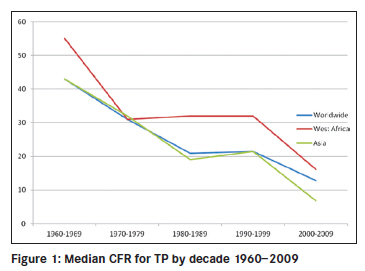
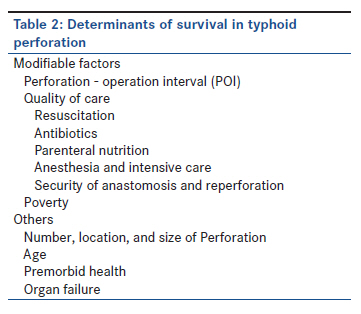
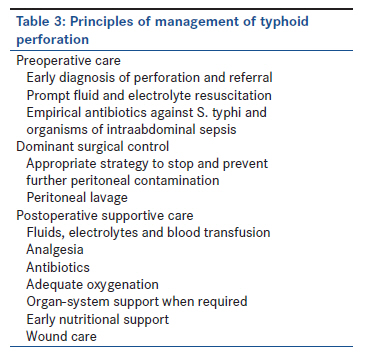
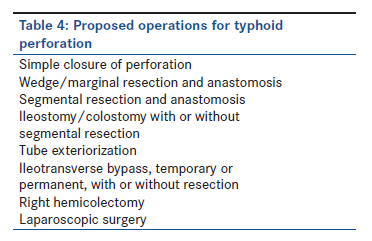
Annals of African Medicine, Vol. 10, No. 4, October-December, 2011, pp. 259-265 Review Article Progress in management of typhoid perforation AY Ukwenya, A Ahmed, ES Garba Department of Surgery, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria Code Number: am11055 PMID: 22064250 Abstract Case fatality rate (CFR) for typhoid perforation (TP) has been on gradual but variable decline world wide. This review highlights the progress in management of TP from 1960 including the controversies, current principles of management and the advances associated with the best results of treatment. This is a review of publications on TP from 1960 to 2010 principally from Medline and Ovid databases. Main search terms used are typhoid and perforation. The median CFR by decade was estimated from studies that reported CFR. With advances in surgery and supportive care, median CFR for TP declined from over 50% in 1960 to single digits in the last decade in some countries but with West Africa lagging behind at 16%. Variations in CFR are attributed to differences in perforation-operation interval and quality of care. Opportunities now exist for patients with TP to recover from the disease but priority remains with prevention of enteric fever in endemic areas.Keywords: Intestinal perforation, mortality, typhoid Introduction Typhoid (enteric) fever is a systemic human infection caused by Salmonella enterica subspecies enterica serovar serotype typhi (Salmonella typhi, S. typhi) in most cases; and to a lesser extent, Salmonella paratyphi, A, B, and C strains. An estimated 22 million people are infected worldwide annually with 200 000 deaths. [1],[2] Control of the infection has been achieved in Europe and North America by effective Public Health measures, but Africa, South East and South Central Asia continue to bear the burden of the disease, principally because many communities still fall short of standards for drinking water, hygiene and sanitation. Intestinal perforation is the most serious complication of typhoid fever estimated to be solely responsible for 25% of deaths. [3] In most parts of the world, perforation rate ranges from 0.6% to 4.9% of enteric fever cases, [2],[3],[4] but in West Africa, higher rates of 10%-33% have been reported. [5],[6],[7],[ 8] This is more of a reflection of statistics from Teaching Hospitals where the very ill patients are seen rather than local disease virulence. Hosoglu et al., [9] have shown that the risk of perforation will be increased if disease progression is not halted by prompt antimicrobial therapy at effective doses to which the local strains of Salmonella typhi are sensitive. Other risk factors include leucopenia, a shorter history of fever and male gender. Mortality from TP has been on gradual but variable decline worldwide. Centers capable of better quality of care are now reporting mortality rates less than 5%. [10],[11],[12],[13],[14],[15] The decline has resulted from improved understanding of the disease pathogenesis and progress in areas of supportive and surgical care. Pathology of Typhoid Perforation Perforation affects the terminal 40 cm of the ileum in 72%-78% of cases; the jejunum, caecum, colon and gallbladder to lesser degree. [8],[11],[16],[17],[18],[19],[20] There are rare reports of duodenal and appendiceal perforations. [21],[22] Perforations may be multiple (3%-40% of series), especially in younger children, as demonstrated by Ekenze and Ikefuna who estimated perforation rate of over 2 per child in children less than 5 years of age. [5],[6],[8],[10],[12],[13],[16],[17],[19],[23],[24],[25],[26],[27],[28],[29],[ 30] In an unprecedented case, Nasir et al., reported 32 perforations in one patient. [31] Pathological changes are not just restricted to perforation sites. [10],[32],[33] The diseased gut is characterized by diffuse nonspecific enterocolitis with hypertrophy, necrosis and ulceration of intestinal and mesenteric lymphatic tissue. Acute and chronic inflammatory cells are involved with predominance of CD68 + leucocytes (macrophages) and CD3 + T lymphocytes at perforation sites. Nguyen et al. were unable to confirm the involvement of Peyer′s patches in most of their series of typhoid perforation in contrast to what is widely believed. [10] Current evidences suggest the mechanism of intestinal injury complicating enteric fever to be immunologically mediated, through release of cytokines from macrophages. [10],[33],[34] The Sanarelli-Shwartzman′s reaction gave insight to this mechanism in 1937 by demonstrating that guinea pigs primed subcutaneously with S. typhi developed skin necrosis and ulcerations when injected with another intravenous dose. [33] Gut macrophages are activated by Salmonella typhi directly by their Toll-like receptors or indirectly via antigen presenting cells. The first gut exposure primes the macrophages which release damaging cytokines such as tumor necrosis factor-alpha at second exposure. Once perforation has occurred, peritoneal contamination will depend on the duration, number, location, and size of perforation. Compounding the patient′s problems will be systemic and metabolic effects of weeks of pre-existing fever. It is perhaps fortunate for the victims of enteric fever that perforation occurs predominantly between the ages of 5 and 30 years when the immune system is fully developed, because the severity of disease and mortality increases steeply away from this age group. [35] In 42%-89% of patients, peritoneal contamination is severe, peritonitis poorly localized and omentum is away from the site of perforation. [8],[14],[18],[19],[26],[36],[37] Peritonitis may occur without gut perforation in about 5% of cases. [8] In line with other forms of secondary peritonitis, infection starts with organisms which survive the peritoneal environment from initial contamination (predominantly facultative gram-negative organisms such as Escherichia coli and Klebsiella). Eventually obligate anaerobes from colon such as Bacteroides species will dominate. [38],[39],[40] Cytokines and other mediators released by immune cells in response to infection cause local and systemic inflammation. The cytokine response has the potential to become self-perpetuating, even after successful control of infection source leading to systemic cellular injury and multiple-systems organ failure. Diagnosis The diagnosis of peritonitis in a patient with pre-existing fever can readily be made at the bedside in most cases. Experience and high index of suspicion may however, be required in a subset of patients particularly, children under 5 years of age in whom peritoneal signs are masked by overwhelming sepsis or immunosuppression. [6],[8],[23] Conventional methods of laboratory confirmation of Salmonella typhi as cause of intestinal perforation have often been unreliable. [41],[42],[43] Identification of Salmonella typhi DNA by polymerase chain reaction with a 100% sensitivity and specificity is set to become the gold standard where it is affordable. [10],[44] Mortality Decline The discovery of chloramphenicol in 1948 was a major landmark in the treatment of enteric fever, dramatically reducing the mortality of nonperforated cases from 15%-25% to 1% and perforated cases from 70% to 50%. [4],[45] This however, heralded the perception that typhoid perforation could be treated nonoperatively, championed by Huckstep. [46] The consequences of the ensuing controversy of surgical and non-surgical management was clearly exposed in the review by Butler et al., [3] in 1985 when they showed that the CFR for patients treated surgically in combination with antibiotics had reduced to 26% while those treated nonsurgically stagnated at 70%. From studies in West Africa, estimated median CFR declined from 57% during the 1960s to 32% by the next decade only to stagnate for thirty years and then decline again to 16.1% in the last decade. [5],[6],[7],[8],[19],[23],[24],[25],[26],[27],[28],[29],[30],[37],[47],[48],[49],[50],[51],[52],[53],[54],[55],[56],[57],[ 58] Comparatively, Asia and other parts of the world with typhoid scourge have enjoyed more gradual decline to appreciable single digit figures in the last decade [10],[11],[12],[13],[14],[15],[16],[18],[25],[36],[59],[60],[61],[62],[63],[64],[65],[66],[67],[68],[69],[70],[71],[72],[73],[74],[75],[76],[77],[78],[79] [Figure - 1]. It must be noted that right from the 1970s, single digit mortality rates had been recorded by authors from Hong Kong, South Korea, Mexico, Turkey, and Nigeria [Table - 1]. Authors such as Chatterjee et al., [79] who reviewed their experiences over three decades from 1966 showed mortality decline from 47.2%, 17.7% to 7%, respectively. They also proffered explanations for the improvements in results, namely, the abandonment of nonoperative management for aggressive resuscitation and early surgery, change of antibiotic policy from chloramphenicol only to chloramphenicol and metronidazole combination and eventually to ciprofloxacin and metronidazole by the third phase. Advances in supportive care have been critical to reducing mortality to single digit. The introductions of aggressive resuscitation, improved anesthetic services, availability of intensive care and organ-system support contributed to reduction in perioperative deaths. Newer and more potent antimicrobials have been introduced over the years taking into consideration the polymicrobial nature of TP peritonitis and the emergence of S. typhi resistance initially to first line antibiotics (chloramphenicol, amoxicillin, and cotrimoxazole), later quinolones and eventually third generation cephalosporins. [44],[81],[82],[83],[84] Those who have added total parenteral nutrition (TPN) to the treatment of their patients have reported dramatic improvement in results. [11],[12],[13],[55],[68] The factors which affect the results of treatment of TP are summarized in [Table - 2]. Published mortality rates vary worldwide because of differences in the quality and access to care. Differences in the perforation-operation interval (POI) indicate that patients are treated at different levels of disease severity in different communities. While some centers have achieved mortality rates less than 5% in the last decade, Nuhu et al. in 2010 still report 28.3% from a tertiary hospital in Northern Nigeria. [26] POI is a major determinant of severity of illness at the time of surgery for TP. [8],[12],[13],[16] Kim et al., [16] from South Korea reported a mortality rate of 9.9% with patients whose POI averaged 38 hours while over half of Archampong′s [8] patients who accounted for 29.8% mortality presented after 5 days of perforation. POI is prolonged in West Africa and other parts of the world because of delayed diagnosis of perforation, poorly regulated patient referral from peripheral hospitals, difficulties sourcing funds for treatment and diversion of patients to alternative medical treatment, among other reasons. The current principles of management of TP are summarized in [Table - 3]. A rationale antibiotic prescription should take into account the life-threatening nature of TP and the possible spectrum of organisms involved. Combinations of metronidazole with ceftriaxone, a quinolone, azithromycin, or cefixime should be adequate but the local pattern of Salmonella typhi multidrug resistance strains and the patient′s ability to fund these drugs have to be taken into account. The emerging preference for fewer antibiotics for peritonitis and multidrug resistance should curtail the use of first-line anti S. typhi drugs which are traditionally prescribed with two other drugs, gentamicin and metronidazole, but as noted by Meier and Tarpley, these drugs are often the ones available or affordable in endemic rural areas. [37],[38] The proliferation of fake and adulterated drugs, access to antibiotics without prescription rampant in countries like Nigeria no doubt poses serious challenge to S. typhi eradication and survival from perforation. Surgical Management A successful operation for TP must control abdominal infection by thorough peritoneal lavage and repair of the perforation site. The strategy to control the perforation should take into consideration the risks of reperforation and anastomotic disruption, the development of which carry serious consequences for the patient. Search for solution to the unacceptably high mortality led to the proliferation of several surgical procedures for TP [Table - 4]. These operative strategies have evolved from reports of surgeons′ experiences rather than prospective randomized control studies, which are the gold standards for introducing new treatment. In addition, many of the studies comparing results of new operative strategies have been misleading because of use of conflicting outcome measures and lack of risk stratification of the patients as highlighted in a study by Mohil et al. [85] Only a hand full of reports on typhoid perforation have risk stratified patients with any of the available methods such as acute physiologic and chronic health evaluation II (APACHE II) and Mannheim peritonitis index (MPI). [12],[85],[86] Valid arguments still, therefore, exist about the superiority of segmental bowel resection over simple closure of single perforation, the benefits of ileostomy over primary repair in presence of severe peritoneal contamination and the advantages of tube ileostomy over the conventional method. The principle of segmental resection is eradication of inflamed, unhealthy bowel around one or multiple perforations and construction of a single anastomosis using viable bowel with better chances of healing and less risk of reperforation or anastomotic disruption. [87] Resection of small bowel reduces need for diversion of fecal stream in patients with severe peritonitis or may be combined with such procedures in selected cases. Ameh et al., [88] from Zaria, Northern Nigeria, in a prospective nonrandomized study showed that patients who had segmental resection and anastomosis had lower reperforation and mortality rates than simple closure and wedge resection and closure. In one of the larger series from a centre involving 352 patients over 25 years, Athie et al., [14] from Mexico city reported the benefits of directed resection of 10 cm of small bowel proximal and distal to a perforation site reducing morbidity and mortality to 1.72% compared to 33.47% and 7.20% when conventional simple closure or resection and anastomosis are used. Atamanalp et al., [18] from Turkey who documented their observations over a 26-year period recorded 12.86% mortality with 70 patients from 1978 to 1990 treated by the policy of simple closure for single perforation, segmental resection and anastomosis for multiple perforations and ileostomy for severe peritoneal contamination. From 1991 to 2004, resection and anastomosis became their preferred operation with no mortality with 12 patients. The advocates of simple closure of single perforation as opposed to segmental resection point to the speed and ease of operation in a patient who may be critically ill. [12],[13],[36] To their credit, improvements in supportive care especially parenteral nutrition has reduced the effects of the dreaded failures of surgery more often associated with simple closure, namely, reperforation and anastomotic disruption such that very good results have been obtained by surgeons who stuck to simple closure of single perforation. [11],[12],[13] The role of ileostomy as a first line operation for TP continues to be debated. It has been recommended for patients with severe peritoneal contamination; enhancing intestinal decompression with improved healing, early resolution of ileus and early start to enteral feeding. [12],[13],[18] Morbidity and hospital stay have been found to be less with patients on ileostomy. Combining ileostomy with resection aims to further reduce the risk of reperforation. The major drawback is the need for a second operation to restore intestinal continuity, the specialized care before closure and the attendant cost which reduces its popularity. [18] Many surgeons resort to ileostomy only for its life saving value in patients with continuing peritoneal contamination from reperforation or anastomotic leak. Tube ileostomy confers the advantages of conventional ileostomy without the need for second operation. Pandey et al., [88] successfully used T-tube as alternate to open ileostomy in 12 patients with severe peritoneal contamination, extubating after an average of 13.2 days with healing of post T- tube fistula in 8.58± 2 days. It has become obvious over the years that a single operation may be inadequate for source control in some patients with secondary peritonitis. [38],[39],[90],[91],[ 92] In children, the anatomically narrow terminal ileum compounded by inflammatory edema of typhoid enteritis presents additional challenges to the security of an anastomosis in presence of severe peritoneal contamination. Such children may benefit from staged operations either in the form of ileostomy to divert fecal stream or planned relaparotomy to combat persistent peritonitis. A properly conducted control study is required to determine the criteria for identifying such patients early in the course of management. Chang et al., [11] who successfully managed 24 children with colonic perforation from enteric fever have suggested that wedge resection and simple closure may be sufficient for solitary caecal perforation which is the commonest. They also employed simple closure and ileostomy; and partial colectomy with colostomy for caecal and colonic perforation. Laparoscopy [93],[94] is a relatively new addition to the treatment of typhoid perforation with promising results. The current numbers treated are small and it is rather too early to define its role. With most patients now surviving surgery for TP, focus is inevitably shifting to the high morbidity rate and prolonged hospital stay which place huge burden on the cost of care. The average patient is unable to feed orally until after the 8 th postoperative day because of paralytic ileus. [37] The average length of hospital stay ranges from 8 to 10 days reported by Shukla et al., [39] to 24.5 days. [11] Wound infection rate can be as high as 81% reported by Gupta et al., [70] but more serious complications such as burst abdomen, intraabdominal abscess and faecal fistula may occur. The POI and severity of peritonitis have been identified as the main factors associated with increased morbidity rate and hospital stay. [12],[13] Onen et al., [13] showed that addition of total parenteral nutrition to treatment from second postoperative day reduced hospital stay from 15.6 ± 3.5 to 10.3 ± 3.1 days while patients on ileostomy were less likely to have wound related complications. Adesunkanmi and Ajao [95] in a retrospective series reported no extra benefit with delayed primary closure of surgical incision for TP compared to primary closure but Duttaroy et al., [96] in a randomized control study showed that delayed primary closure of dirty abdominal incisions which included patients with TP was associated with significant reduction in rates of wound infection (2.7% vs 42.5%), wound dehiscence (2.7% vs 25%) and length of hospital stay (13.86 vs. 18.52) days compared to primary closure. Conclusion Progress in the last five decades has provided opportunities for the patient with once dreaded TP to recover from the disease. Mortality however, continues to be high in the West African subregion because of suboptimal quality of care. Future investments must center on prevention of typhoid fever and perforation because they are achievable, cheaper and safer than cure. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11055t3.jpg] [am11055f1.jpg] [am11055t2.jpg] [am11055t4.jpg] [am11055t1.jpg] |
| |||||||||


{kind=link}
![Table - 1]](/showimage?am/photo/am11055t1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}