 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 10, No. 4, October-December, 2011, pp. 266-271 Review Article Doppler ultrasound in the assessment of suspected intra-uterine growth restriction N AL Qahtani Department of Obstetrics and Gynecology, King Fahad University Hospital, University of Dammam, Saudi Arabia Code Number: am11056 PMID: 22064251 Abstract Small fetuses constitute a large heterogenous group that includes healthy small fetuses, chromosomally abnormal fetuses and fetuses suffering from utero-placental insufficiency leading to restriction in fetal growth. This review outlines the diagnosis of intra-uterine growth restriction and describes how to differentiate this group from the group of healthy small fetuses. This is very crucial in the management of small fetuses in order to avoid unnecessary intervention in the healthy group, as well as avoid stillbirth and neonatal mortality and morbidity.Keywords: Doppler ultrasound, fetus, growth restriction, monitoring Introduction Small-for-gestational-age (SGA) fetuses are a heterogeneous group comprising fetuses that have failed to achieve their growth potential intra-uterine growth restriction, (IUGR) and fetuses that are constitutionally small. Approximately 50% to 70% of fetuses with birth weight below 10 th centile for gestational age are constitutionally small; [1] and the higher the centile for defining SGA, the higher the likelihood of IUGR. It is very important to differentiate these types of SGA fetuses for two main reasons. First, IUGR fetuses have a low growth-potential, as a result of genetic disease or environmental damage, or due to reduced placental perfusion and ′utero-placental insufficiency′; and they are at increased risk of perinatal morbidity and mortality and will require close feto-maternal monitoring and probably earlier intervention. Second, constitutionally small fetuses are perfectly healthy fetuses, with no increased risk of perinatal death or morbidity, [2] and they need minimal monitoring and should receive routine antenatal care, once they are recognized as healthy. In addition, IUGR fetuses have been shown to have increased adverse outcome in adult life. They have increased prevalence of syndrome X, a condition associating obesity with hypertension and non-insulin-dependent diabetes mellitus. [3] In this review, a brief discussion about the ultrasound diagnosis of suspected IUGR, and thereafter about the use of Doppler ultrasound in the diagnosis of IUGR, will be presented, followed by a description of how to differentiate this group from the group of constitutionally small healthy fetuses. Once an IUGR fetus is identified, the pregnancy should be followed by more specialized persons for monitoring the status during the course of pregnancy and determining the timing of delivery. Fetal hypoxia, oxygen deficiency in the tissues, of any cause leads to a conversion from aerobic to anaerobic metabolism, which produces less energy and more acid. If the oxygen supply is not restored, the fetus dies. Hypoxia may result from:
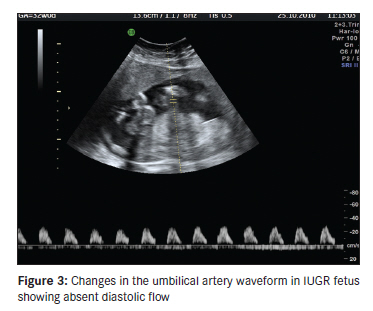
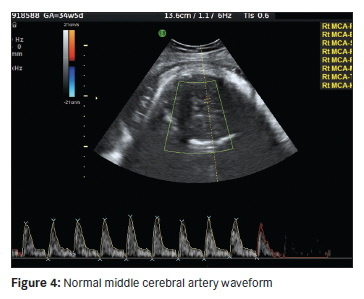
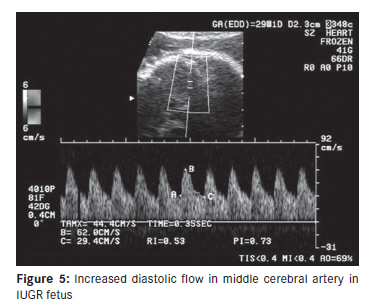
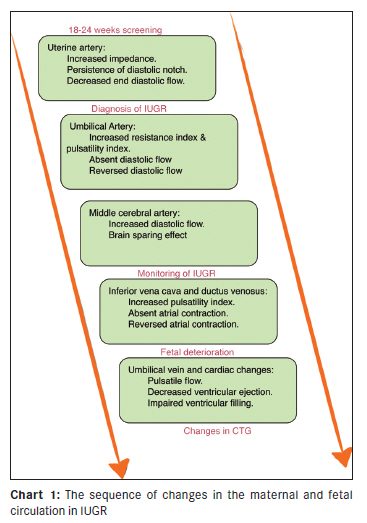
In this review, only hypoxemic hypoxia will be discussed. Diagnosis of Intra-Uterine Growth Restriction Methods employed to detect SGA fetuses include abdominal palpation, measurement of symphyseal fundal height, ultrasound biometry, ultrasound-estimated fetal weight and ultrasound Doppler flow velocimetry. All these methods, except Doppler flow velocimetry, attempt to measure the fetal size and not fetal health. For all these measurements, an accurate estimation of gestation is a prerequisite. Other important prognostic factors for SGA are maternal height, weight, ethnicity, parity and fetal gender. Clinical estimation of fetal weight (EFW) is notoriously inaccurate, [3] and ultrasound biometry of the fetus is now the gold standard for assessing fetal growth. Combination of biparietal diameter (BPD), abdominal circumference (AC), femoral length (FL) and head circumference (HC) gives the highest accuracy. The Shepard and Aoki formulas are recommended for estimating fetal weight. However, these formulas were validated over birth weights of 2,080 to 4,430 g, and therefore their use outside this range may be inappropriate. The Hadlock formula may be more appropriate when the fetus is expected to be very small. [4] When a small fetus is diagnosed, the risk of chromosomal defects should be assessed. Up to 19% of fetuses with AC and EFW less than the fifth centile may have chromosomal defects. The risk is higher when growth restriction is associated with structural abnormalities, a risk associated with normal uterine or umbilical artery Doppler. [5] Therefore, all growth-restricted fetuses need at least an ultrasound anatomical survey. It may also be appropriate to offer karyotyping. When a diagnosis of small fetus is made based on biometric measurements, the umbilical artery Doppler should be used as the primary surveillance tool. This is the main diagnostic tool to differentiate a growth-restricted fetus from constitutionally small healthy fetus. Symmetry of the fetal growth is only of value after 34 weeks; before that, all fetuses have relatively larger heads, which will mask the brain-sparing effect. When an anomaly scan and umbilical artery Doppler are normal, the small fetus is likely to be a "normal small fetus." A randomized controlled trial [6] of two regimens of fetal surveillance for SGA fetuses with normal umbilical artery Doppler found that twice-weekly compared with fortnightly monitoring resulted in earlier deliveries and more inductions of labor with no difference in neonatal morbidity. This suggests frequency of monitoring in SGA fetuses with normal Doppler need not generally be more than once every fortnight. The biophysical profile has not been shown to improve perinatal outcome, but sufficient data do not exist to rule out its value. There is evidence from uncontrolled observational studies that biophysical profile in high-risk women has good negative predictive value, i.e., fetal death is rare in women with a normal biophysical profile. [7] Given the absence of its benefit, as indicated by randomized trials, and that biophysical profile is a time-consuming test, it cannot be recommended for routine monitoring in low-risk/unselected pregnancies or for primary surveillance in SGA fetuses. However, when primary surveillance with umbilical artery Doppler is found to be abnormal, biophysical profile is likely to be useful, given its good negative predictive value in high-risk populations. [7] This recommendation is further supported by the evidence that in high-risk women, the biophysical profile was rarely abnormal when Doppler findings were normal. [8] A recent study showed, that in IUGR fetuses delivered at 32 weeks, the integration of Doppler and neonatal outcome were statistically correlated with Biophysical profile (BPP). [8] Use of cardiotocography (CTG) antepartum to assess fetal condition is not associated with better perinatal outcome; in fact, a systematic review of randomized trials showed that there was a trend towards increased mortality in the group receiving CTG compared with those who did not. [9] Doppler Studies in IUGR Uterine artery In pregnancies complicated by intrauterine growth restriction, impedance to flow in the uterine arteries is increased. Studies in women with hypertensive disease of pregnancy have reported, that in those with increased impedance (increased resistance index or the presence of an early diastolic notch), compared to hypertensive women with normal flow-velocity waveforms, there is a higher incidence of preeclampsia, intrauterine growth restriction, emergency cesarean delivery, placental abruption, shorter duration of pregnancy and poorer neonatal outcome. [10] It has been shown, that in both high-risk and low-risk pregnancies, increased impedance to flow in the uterine arteries is associated with increased risk of subsequent development of preeclampsia and IUGR. Increased impedance to flow in the uterine artery identifies 30% of those that subsequently develop IUGR. Almost every major artery and vein in the fetus has been studied in normal and growth-restricted fetuses. However, for practical management of suspected IUGR, umbilical artery and middle cerebral artery will be discussed, and study of these blood vessels will suffice for the diagnosis of IUGR in a fetus. Study of the fetal venous flow is important in the follow-up of fetuses with confirmed preterm IUGR who should be referred to feto-maternal units for further assessment and follow-up. Umbilical arteries The umbilical artery was the first fetal vessel to be evaluated by Doppler velocimetry. Flow-velocity waveforms from the umbilical artery have a characteristic saw-tooth appearance of arterial flow in one direction [Figure - 1]. In suspected IUGR with normal umbilical artery waveform with adequate growth over a period of 2 weeks, it can be assumed that the fetus is healthy and it is a constitutionally small fetus. In terms of monitoring growth-restricted pregnancies, abnormal waveforms in the umbilical artery are an early sign of fetal impairment. The median time interval between absence of end-diastolic frequencies and the onset of late decelerations was 12 days (range, 0-49 days). [11] Pathological studies have demonstrated that increased impedance in the umbilical arteries becomes evident only when at least 60% of the placental vascular bed is obliterated. [12] Clinical studies of umbilical arterial flow-velocity waveforms in intrauterine growth restriction have reported progressive increase in impedance to flow until absence and, in extreme cases, reversal of end-diastolic frequencies [13] [Figure - 2] and [Figure - 3]. The latter represents the extreme end of the spectrum. Middle cerebral artery With the color Doppler technique, it is possible to investigate the main cerebral arteries, such as the middle cerebral artery (MCA), to evaluate the vascular resistances. A transverse view of the fetal brain is obtained at the level of the biparietal diameter. The transducer is then moved towards the base of the skull at the level of the lesser wing of the sphenoid bone. Using color flow imaging, the middle cerebral artery can be seen as a major lateral branch of the circle of Willis, running antero-laterally at the borderline between the anterior and the middle cerebral fossae [Figure - 4]. The pulsed Doppler sample gate is then placed on the middle portion of this vessel to obtain flow-velocity waveforms. Due to the course of this blood vessel, it is almost always possible to obtain an angle of insonation which is less than 10°. During the studies, care should be taken to apply minimal pressure to the maternal abdomen with the transducer, as fetal head compression is associated with alterations of intracranial arterial waveforms. Increased diastolic flow velocity in the middle cerebral artery reflects fetal compensation to the utero-placental insufficiency (brain-sparing effect) [Figure - 5]. In fetuses with IUGR, the trends of the middle cerebral artery pulsatility index (MCA-PI) and middle cerebral artery peak systolic velocity (MCA-PSV) provide more clinical information than does one single measurement. A high MCA-PSV predicts perinatal mortality better than a low MCA-PI. It has been proposed that MCA-PSV might be valuable in the clinical assessment of IUGR fetuses that have abnormal umbilical artery (UA) Doppler. [14] Umbilical vein In IUGR fetuses, changes in the venous circulation follow those of the arterial circulation. The earliest changes are usually in the inferior vena cava and ductus venosus. These changes reflect preferential redistribution of the blood from the umbilical vein to the ductus venosus to the heart and brain at the expense of the hepatic circulation. In severely compromised growth-restricted fetuses, there is pulsatile flow in the umbilical vein. There are also changes in the myocardial function with decompensation. Fetal venous studies are useful in monitoring IUGR fetuses. Normal findings suggest continuing fetal compensation, while abnormal flow indicates decompensation. [Chart 1] shows the sequence of changes in the maternal and fetal circulation in IUGR . Discussion A review of 12 randomized, controlled trials of Doppler ultrasonography of the umbilical artery in high-risk pregnancies reported that, in the Doppler group, there was a significant reduction in the number of antenatal admissions [44%; 95% confidence interval (CI), 28%-57%], induction of labor (20%; 95% CI, 10%-28%), and cesarean section for fetal distress (52%; 95% CI, 24%-69%) 37. Furthermore, the clinical action guided by Doppler ultrasonography reduced the odds of perinatal death by 38% (95% CI, 15%-55%). Post hoc analyses revealed a statistically significant reduction in elective delivery, intra-partum fetal distress, and hypoxic encephalopathy in the Doppler group. It was concluded that there is now compelling evidence that women with high-risk pregnancies, including preeclampsia and suspected intrauterine growth restriction, should be offered Doppler ultrasonographic study of umbilical artery waveforms. [15] The abnormalities in umbilical artery waveform will reflect early changes in the utero-placental circulation, and the changes in middle cerebral artery will identify which fetus is compensating. The median time interval between absence of end-diastolic frequencies and the onset of late decelerations was 12 days (range, 0-49 days). [16] In the management of the preterm (before 33 weeks of gestation) growth-restricted fetus, there is uncertainty as to whether iatrogenic delivery should be undertaken before the development of signs of severe hypoxemia, with a consequent risk of prematurity-related neonatal complications; or whether delivery should be delayed, but with the risks of prolonged exposure to hypoxia and malnutrition imposed by a hostile intrauterine environment. A growth-restricted fetus leading an ascetic existence from chronic starvation during the late second or early third trimester is capable of tolerating chronic hypoxemia without damage for much longer than a well-nourished late-third-trimester fetus with high energy consumption. In the growth-restricted hypoxemic fetus, redistribution of well-oxygenated blood to vital organs, such as the brain, heart and adrenals, represents a compensatory mechanism to prevent fetal damage. When the reserve capacities of the circulatory redistribution reach their limits, fetal deterioration may occur rapidly. In clinical practice, it is necessary to carry out serial Doppler examination to estimate the duration of fetal blood flow redistribution. The onset of abnormal venous Doppler results indicates deterioration in the fetal condition, and iatrogenic delivery should be considered. Recently, examination of the fetal venous system has allowed refinement in our understanding of normal fetal circulation, as well as fetal well-being. Venous vessels commonly assessed include the umbilical vein, ductus venosus and inferior vena cava. The interrogation of the ductus venosus has yielded the most robust results as far as prediction of neonatal complications is concerned, and likely serves as the best ′trigger′ for delivery when abnormalities are found. When placental dysfunction is the cause of IUGR, cardiovascular system compromise is believed to follow a pattern of ′deterioration′ that can be assessed by both fetal arterial and fetal venous Doppler interrogation. Briefly, early changes are noted first in the umbilical artery, followed by changes in the umbilical vein and ductus venosus, and finally in the pulmonary artery and aorta. Serial assessments of the circulatory changes in the growth-restricted fetus may identify this pattern of change, allowing for intervention prior to irreversible intrauterine damage. [17] On average, the time interval between the onset of abnormal umbilical arterial Doppler results and the onset of late fetal heart rate decelerations is about 2 weeks, but this interval differs considerably among fetuses and is shorter in late than early pregnancy. [18] Postnatal follow-up studies, at the age of 7 years, have reported that growth-restricted fetuses with abnormal aortic velocity waveforms had minor neurological dysfunction and impaired intellectual outcome. If these findings are confirmed in prospective studies with adequate controls for confounding variables, such as degrees of prematurity, smallness and management, it may be advisable to deliver growth-restricted fetuses before these blood flow alterations occur. On the other hand, fetuses showing the brain-sparing effect did not have an increased risk for moderate or severe neurological handicap at the age of 2 years. [19] The best assessment of IUGR fetuses requires a combination of parameters testing both circulatory and behavioral responses to placental insufficiency. Integration of many Doppler measures and five components of biophysical profile scoring may be difficult to use for assessment, producing a combination of alarming and reassuring results. A recent study addresses the need to eliminate redundant parameters from this assessment. In the complex evaluation of IUGR fetuses, multiple tests must be integrated to give the best prediction. Most parameters yield significant improvement when added to the assessment, although they differ in strength. [20] Conclusion It will always be a challenge to weigh the risks and benefits of early interventions against each other; and it is a dynamic process, in which advancements in both fetal and neonatal medicine are of crucial importance for the counseling of parents and the management of these pregnancies. Limitations in such an approach remain, however. For instance, the influence of prematurity, in and of itself, prior to 27 weeks is so strong that it likely eclipses any predictive value of abnormal Doppler assessments to newborn outcomes. After 27 weeks, an abnormal ductus venosus Doppler study is likely a better predictor of perinatal outcome and thus performs better as a trigger for delivery, as the influence of prematurity at and beyond 27 weeks in the modern neonatal intensive care unit becomes less compelling. Ultimately, a combination of biophysical and cardiovascular parameters may be useful in determining appropriate management, and timing of delivery, for the growth-restricted fetus. [21] The current evidence mandates that Doppler velocimetry of the fetal arterial and venous circulation should be an integral component of fetal surveillance in pregnancies complicated with fetal growth restriction. Obviously, no single testing modality should be regarded as the exclusive choice for fetal surveillance, as these tests reveal different aspects of fetal pathophysiology, often in a complementary manner. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11056f2.jpg] [am11056f3.jpg] [am11056f5.jpg] [am11056f1.jpg] [am11056f4.jpg] [am11056c1.jpg] |
| |||||||||

![Figure - 1].](/showimage?am/photo/am11056f1.jpg){kind=link}
![Figure - 2]](/showimage?am/photo/am11056f2.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}