 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 10, No. 4, October-December, 2011, pp. 272-277 Original Article Anemia in pregnancy at two levels of health care in Ibadan, south west Nigeria Adesina Olubukola1, Akinyemi Odunayo2, Oladokun Adesina1 1 Department of Obstetrics and Gynaecology, Medical Statistics and Environmental Health, College of Medicine, University of Ibadan, Nigeria Code Number: am11057 PMID: 22064252 Abstract Background: In Africa, anemia in pregnancy contributes to non-attainment of the MDG goals 4 and 5. This study examined the prevalence and some risk factors for anemia at two levels of health care in the Ibadan metropolis.
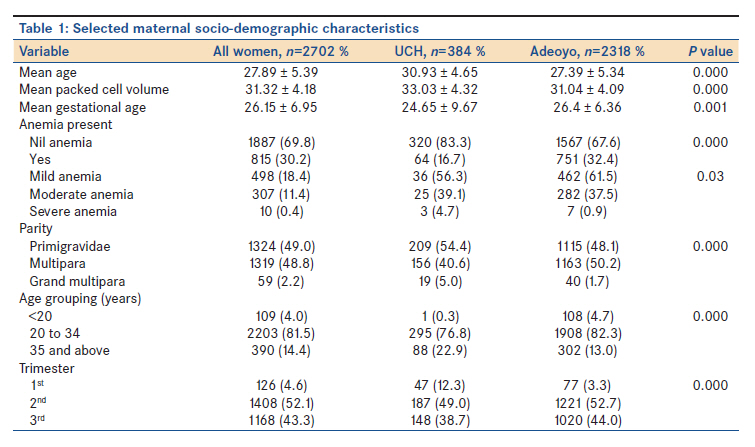
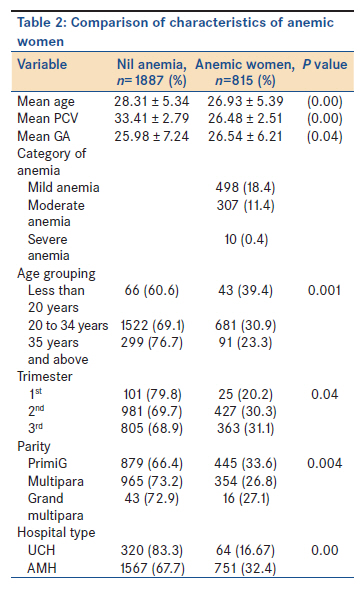
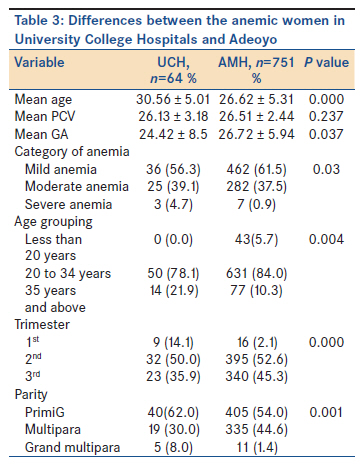
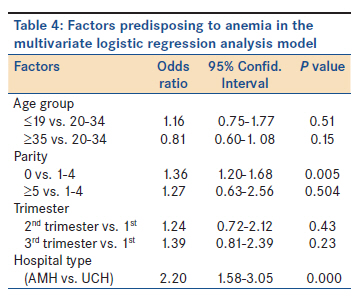
Keywords: Anemia, empowerment, etiology, parity, pregnancy Introduction An estimated 58.27 million women worldwide are anemic during pregnancy, 95.7% of whom live in developing countries. [1] In Africa, the prevalence of anemia in pregnancy has been estimated to be 35-75%. [1] It continues to be a topical issue in many developing countries because of its association with adverse pregnancy outcome such as increased rates of maternal and perinatal mortality, premature delivery, low birth weight, etc. [2],[3] In Nigeria, where a conservative maternal mortality ratio of 1,000-1,500/100,000 live births is reported, anemia has been estimated to contribute to 11.0% of these deaths. [3],[4] Anemia may worsen the sequelae of postpartum hemorrhage and predispose to puerperal infection-both important causes of maternal mortality in developing countries. [3] In the infant, it is a risk factor for iron deficiency anemia which if un-corrected, can be associated with adverse behavioral and cognitive development. [5] The etiological factors for anemia in pregnancy are multiple and their relative contributions vary by geographical area and by season. [5],[6] In West Africa, the most common cause is nutritional deficiency especially of iron and folic acid. [3],[5] Other causes include parasitic infestations such as malaria and hookworm; infections like HIV and hemoglobinopathies. [2],[7] The predisposing factors are grand-multiparity, young age, low socioeconomic status, and illiteracy. [5],[8] Others include inter-pregnancy spacing of <1 year and late booking among others. [8],[9] These factors abound among pregnant women in Nigeria, making anemia in pregnancy an important reproductive health problem. [5],[8] With the attainment of the MDGs becoming increasingly distant, it is important to constantly examine factors such as anemia in pregnancy, which contributes to adverse maternal and infant health outcomes. Thus, the objectives of this study were to examine the prevalence of anemia at two levels of health care in the Ibadan metropolis and examine some factors associated with this problem. Materials and Methods This was a retrospective study of normal pregnant women who registered with the antenatal units of the University College Hospital (UCH) and the Adeoyo Maternity Hospital (AMH) both in the city of Ibadan between September 1, 2008 and December 31, 2008. While UCH is a tertiary health institution offering both primary health services and serving as a major referral center for the people of Ibadan and its environment, AMH serves as a secondary maternity referral center and as a primary facility for the people of Ibadan and environs. The case records of women registering for care at both institutions during the period under review were retrieved from the medical records department of the hospital. Data were obtained with respect to age, parity, gestational age at booking, and packed cell volume at booking. To qualify for this study, the case must be a singleton pregnancy with no complaint of vaginal bleeding and no known chronic illness such as sickle cell disease. In both hospitals to determine packed cell volume (PCV), blood is taken by finger prick into a capillary tube. After centrifugation with the microhematocrit centrifuge for 5 min at 3000 rpm, the PCV was measured using a Hewkley microhematocrit reader. PCV less than 30% (or hemoglobin less than 10.0 g/ dL) was considered to be anemia in pregnancy. The severity of anemia was classified as follows: mild (PCV 27-29%), moderate (PCV 19-26%), and severe (PCV below 19%). [10] Data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 11 (SPSS Inc; 2001). There was cross-tabulation of various variables against PCV. Proportions were compared using the Chi-square test and Fisher exact test, where appropriate. Means were compared by the t-test. A P value of <0.05 was considered significant. Ethical permission for the study was obtained from the joint UI/UCH institutional review board. Results During the study period, 507 patients presented for care at UCH. One hundred and twenty-three women (123, 24.3%) either had chronic illnesses as determined by the history they gave or did not have adequate data and so were excluded from further analysis. At Adeoyo maternity hospital, 2698 women presented for care of whom 380 (14.1%) either had chronic illnesses as determined by the history they gave or did not have adequate data and so were excluded from further analysis. The data from a total of 2702 women, 384(75.7%) and 2318 (85.9%) from UCH and Adeoyo, respectively, were available for analysis. [Table - 1] shows the distribution of selected maternal characteristics at booking. While over half of the patients presented in the 2 nd trimester and beyond, almost half of the patients were primigravidae. The patients in UCH were older, with higher mean PCV and booked at lower GA compared to the women in AMH. These differences were statistically significant. While UCH had a higher proportion of patients older than 35 years, booking in the 1 st trimester of pregnancy and being primigravids, the contrast was seen in Adeoyo. About 30% of patients overall were anemic. Severe anemia was seen in 0.4%. A higher proportion of anemia was seen in patients presenting in Adeoyo. [Table - 2] shows the characteristics of the women with PCV less than 30%. The anemic women were younger and booked later. A higher proportion of anemia was observed in women less than 20 years, women booking in the 2 nd /3 rd trimesters of pregnancy and in primigravidae. These differences were statistically different. [Table - 3] shows the differences between the anemic women booked in UCH and Adeoyo. Similar to the general profiles of patients seen in these hospitals, the anemic patients in UCH were older and booked at lower GA compared to the women in AMH. These differences were statistically significant. In addition, the anemic patients in UCH had a higher proportion of patients older than 35 years, booking in the 1 st trimester of pregnancy and were primigravidae. Discussion The 30% prevalence of anemia reported in this study is slightly higher than the value of 25.0% reported by Aimakhu et al., [11] working in the same city, earlier in the decade, and the rate of 15.0% reported by Akeredolu and Fakeye [12] from Ilorin in the same region. It is however slightly lower than the rate of 35.3% reported by Anorlu et al., [3] working in the same south west region, 51.8% reported by Bukar et al., [5] working in northern Nigerian, and 40.4% reported by Dim and Onah [2] working in south east Nigeria. When the World Health Organization [1] criterion for the diagnosis of anemia in pregnancy, i.e. hemoglobin <11.0 g/dl (PCV <33%) is applied, 60.8% of the women were anemic. A range of 35-75% has been reported for developing countries. [10],[13] The definition of what constitutes anemia in pregnancy has been the subject of lively debate for several years. If this definition were to be applied in Nigeria, more than two thirds of women attending antenatal clinics in the country will require to be investigated for anemia. [13] In practice, it has been found that a large number of pregnant Nigerian women with hematocrit values between 30% and 33% get through pregnancy without any apparent ill effects to themselves or their offspring. Thus, in practice, only anemia with hematocrit lower than 30% is deemed worthy of further investigation and treatment in this environment. [13] While most cases of anemia were either mild or moderate, some women still presented with severe anemia. The proportion of 0.4% with severe anemia is similar to the value of 0.7% reported from Sagamu [14] but lower than 2.1% by Bukar et al. [5] Mild to moderate anemia, although generally well-tolerated, clearly adversely affects the sense of well-being, resulting in fatigue and a decrease in work capacity. Women in sub- Saharan Africa are the "hewers of wood and the drawers of water," therefore the decreased work capacity as a result of the anemia will have economic consequences on the family in particular and on society at large. [5] In this study, we found that being younger was associated with higher proportion of anemia. This is similar to the finding of Hoque et al., [15] working in Greytown south Africa, and Idowu et al., [16] working in Abeokuta. However, it is at odd with the finding of Dim and Onah, [2] Aimakhu et al., [11] and Bukar et al. [5] It must however be noted that the influence of age is often closely intertwined with that of parity. In this study, we found that anemia was significantly higher in the primigravidae and in women booking in the 2 nd /3 rd trimesters of pregnancy. Generally, anemia is more common in the primigravidae than in the multigravidae in sub-Saharan Africa. [1] Although one might expect that anemia in pregnancy would tend to increase with rising parity owing to repeated drain on iron stores, [5],[8] various workers have observed a progressive decline in iron stores but increasing mean Hb levels with increasing parity and attributed these differences to a greater risk of malaria in the primigravida. [3],[8],[17] The effect of gestational age in both facilities is similar to the findings of other workers. [3],[5] This has been attributed to the expected drop in hematocrit as a result of plasma volume expansion. [5],[18] In addition, in malarious areas, the nadir in Hb levels in pregnancy occurs between 16 and 25 weeks′ gestation and is an indication of a malaria-induced hemolytic anemia. [3] Other reasons that have been attributed for this are that as a result of fetal demand and underlying maternal disease, untreated anemia in early pregnancy is likely to get worse with advancing pregnancy. [5],[9] In addition, deficient or absent antenatal care and not receiving any iron/folic acid supplements and malaria chemoprophylaxis, both of which are routinely used for the prevention of anemia in pregnancy in Nigeria maybe other contributing factors. [3] A disaggregation of the data reveals a striking difference in the proportion of anemia in both hospitals. The rate in the UCH population is closer to the rate reported by Akerodolu and Fakeye [12] who worked in a tertiary hospital while the Adeoyo value is similar to the value reported by Bukar et al. [5] AMH is a secondary level health institution with a not-for-profit policy. Thus, it tends to attract clientele of lower socioeconomic status. The University College Hospital on the other hand is the apex referral center in the state. It operates on a fee paying mandate and tends to attract a more educated clientele of higher socio-economic status. Facility type in a broad sense may thus be a proxy for the socio-economic status of the clientele. The reason for the low prevalence rates of anemia from the tertiary hospital may thus be due to the population studied, mostly women of higher socioeconomic status. The higher proportion of anemia in AMH may not be unrelated to the low socioeconomic status of the women who seek care in this facility. Bukar et al. [5] also attributed the high incidence of anemia in the women he studied to the low socioeconomic status of that obstetric population. The higher rates in women in the low socioeconomic class have been attributed to the consumption of diets low in animal protein and high in carbohydrates and phytates that may interfere with intestinal uptake of iron and other trace minerals. [5],[19] In addition, these economically disadvantaged women may not be able to access good health services and therefore suffer the deleterious effects of poor nutrition, chronic infestations, and infections. Indeed, a woman who is of low socioeconomic status may have chronic iron deficiency anemia even before pregnancy and the demands of the fetus in pregnancy may worsen it [3] [Table - 4]. Limitations of this study include the fact that it was a hospital-based study. In addition, it was a retrospective study with the challenge of missing data. The study was not able to examine the contribution of risk factors such as malaria infection, menstrual blood loss, and poor nutritional intake. This will require better funding and give better insight to the role of these factors. In conclusion, anemia in pregnancy is still a common condition in this obstetric population. Governments at all levels need to see it as an important health problem and tackle it accordingly. In the short-term, the provision of affordable and accessible services in the pre-conceptional period with provision of fe/folic acid supplementation and antenatal services geared towards the early detection and treatment of anemia before delivery has been advocated. In the long-term, empowering these women economically and educationally will improve their earning powers and lead to increased awareness and better utilization of antenatal services. All of these efforts would ensure safe motherhood and achievement of relevant MDG targets. Acknowledgement We express our sincere appreciation to the management of the two institutions for allowing the study and the women who allowed their data to be used in this study. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11057t1.jpg] [am11057t2.jpg] [am11057t4.jpg] [am11057t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}