 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
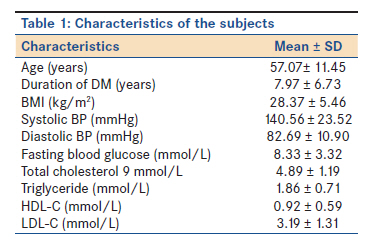
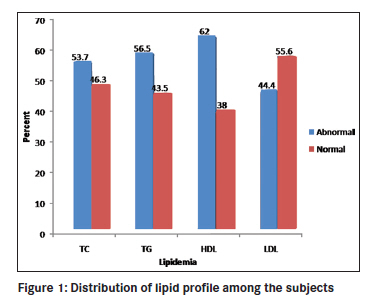
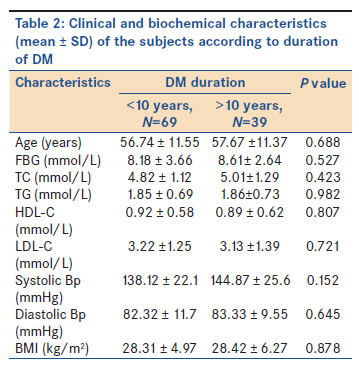
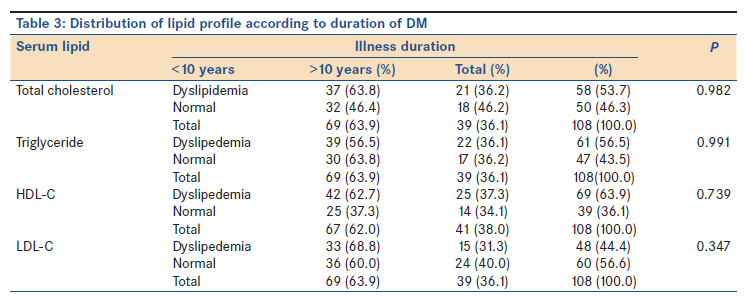
Annals of African Medicine, Vol. 10, No. 4, October-December, 2011, pp. 285-289 Original Article Dyslipidemias in type 2 diabetes mellitus patients in Nnewi South-East Nigeria NN Jisieike-Onuigbo1, EI Unuigbe2, CO Oguejiofor1 1 Department of Medicine, Nnamdi Azikiwe University Teaching Hospital Nnewi, P.M.B 5025 Nnewi, Nigeria Code Number: am11060 PMID: 22064254 Abstract Background: Dyslipidemia has been noted to play an integral role in the pathogenesis and progression of micro and macrovascular complications in diabetes mellitus patients. The complications exemplified by renal vascular and cardiovascular disease cause the most morbidity and mortality in this group of patients.Objective: This study is aimed at understanding the pattern of dyslipidemia among type 2 diabetic patients. Materials and Methods: A total of 108 consenting adult type 2 diabetic patients seen in the medical unit of the Nnamdi Azikiwe University Teaching Hospital Nnewi were evaluated in this crosssectional study. Their fasting lipid profile, fasting blood glucose, weight, height and blood pressure were evaluated. Result: The prevalence of dyslipidemia (at least one abnormal lipid profile) was 90.7%. The 24.1% had single dyslipidemia while 66.6% had combined dyslipidemia. Reduced HDL constituted the highest single abnormality (62%) followed by hypertriglyceridemia (56.5%), hypercholesterolemia (53.7%) and high LDL in (44.4%). The duration of DM was not significantly associated with dyslipidemia (P >0.05). Conclusion: Dyslipidemia is highly prevalent among type 2 diabetic patients in Nigeria with the majority of the patients having combined dyslipidemia. We recommend that aggressive treatment of lipidemia and hyperglycemia can be instituted to reduce the risk of macro and microvascular complications. Keywords: Dyslipidemias, type 2 diabetes mellitus, Nigeria Introduction Type 2 diabetes mellitus is associated with various patterns of dyslipidemia. The Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III, or ATP III) made diabetes mellitus a coronary heart disease (CHD) equivalent, thereby elevating it to the highest risk category. [1] Moderate hypertriglyceridemia and a lower level of high density lipoprotein (HDL) characterize most type 2 diabetic patients, with hypertriglyceridemia being an independent risk factor for coronary heart disease. [2] The impact of coronary heart disease in industrialized countries as the leading cause of death in men and women is well documented [3],[4] and in the developing world it is now becoming an increasing cause of death. [5] The current environmental adaptation toward urbanization and changes in lifestyle could be responsible for the rising prevalence of obesity which has been linked with lipid abnormalities in Africans [6] these two being important criteria in the diagnosis of the metabolic syndrome. Dyslipidemias occur as a result of metabolic derangement which in type 2 diabetic patients is basically due to insulin resistance leading to defect in lipid handling. Insulin resistance, relative insulin deficiency, and obesity are associated with hypertriglyceridemia, low serum HDL cholesterol concentrations, and occasionally high serum low density lipoprotein (LDL) cholesterol and lipoprotein(a) values. [7],[8] The very high risk of atherogenicity associated with the small dense LDL particles has resulted in emphasis on aggressive lowering of LDLC to therapeutic targets among patients with diabetes mellitus more so since this pattern of lipid abnormalities can be detected before the onset of overt hyperglycemia. [9] In this study, the serum lipid abnormalities in type 2 diabetic patients seen in the medical unit of the Nnamdi Azikiwe University Teaching Hospital Nnewi were examined with the aim of determining the type of lipoprotein disorders associated with the patients. Data on this are scanty in this part of the country and our findings will help to make a case for or against the need to aggressively manage dyslipidemia among diabetic patients. Materials and Methods This study was conducted at Nnamdi Azikiwe University Teaching Hospital Nnewi, a tertiary health institution in SouthEast Nigeria which receives referrals from states within and beyond the South East region of Nigeria. This was a hospital-based cross-sectional study. A total of 108 consecutive adult type 2 diabetic patients attending the medical outpatients clinics, diabetic clinic or admitted into the medical wards of the hospital were recruited over a period of 12 months. They were 40 years and above and managed with either oral hypoglycemic agents alone or in combination with insulinor only on insulin as a result of secondary failure of oral hypoglycemic agents. All those who were type 1 diabetics or aged below 40 years and managed only with insulin injection were excluded. Similarly patients on lipid lowering agents, lipid altering diseases such as nephrotic syndrome hypothyroidism and hepatobiliary diseases were also excluded. The study design was explained to each patient and informed consent obtained in each case and then a researcher administered questionnaire defining the patient′s demographics and relevant medical history was completed,blood samples for fasting blood glucose and lipid profile were collected after an overnight fast of at least 14 h. Their weights were measured in kilograms using hospital health scale ZT120 from Hangzhou Tianheng Technology Co.Ltd. Room 124102,Nandu Huayuan 3 rd part, Xihu district, Hangzhou,China P.C.: 310012 with patients putting on light clothing without foot wears. Their heights were measured in meters using the same scale. The body mass index BMI defined as weight in kilogram divided by the square of patient′s height in meters was then calculated. Blood pressure was measured twice for each patient after 5 min interval, and the mean of the two taken as the final record. This was done using Accuson mercury sphygmomanometer A.C.Cosor and Sons (Surgical) LTD, Accoson works, Vale Road London N4 1PS.Diabetes mellitus, hypertension, obesity using BMI measurement and dyslipidemia were defined using WHO criteria. [10],[12] The fasting lipid profile (duration of fasting of at least 14 h) was measured for the subjects using the kit from Biosystems S.A. Costa Brava, 30 Barcelona (Spain). Samples were assayed at the chemical pathology laboratory of NAUTH Nnewi. The lipid assays were done using already standardized and well established methodology. [13] Dyslipidemia was taken as total cholesterol >5.2 mmol/L, low density lipoprotein >3.5 mmol/L, triglyceride >1.7 mmol/L high density lipoprotein <0.9 mmol/L for males and <1.0 mmol/L for females. [12] Data entry and analysis were done using SPSS statistical software version 13. Continuous variables such as age, BMI, blood pressure, fasting blood glucosewere analyzed using descriptive statistics and results were expressed as mean ± SD. Comparisons of means and tests of association were done using independent ttest and χ tests respectively. P value <0.05 was regarded as statistically significant. Results The study population comprised of 108 type 2 diabetics with a male:female ratio of 1.121 (males 52.8%, females 47.2%) and age range 4880 years. The characteristics of subjects are shown in [Table - 1]. Sixty-nine (63.9%) were diagnosed diabetic for ≥10 years and 39 (36.1%) for <10 years. Dyslipidemia was observed with each of the lipid profile [Figure - 1]. Reduced HDL constituted the highest single abnormality (62%) followed by hypertriglyceridemia in 56.5%, hypercholestrolemia in 53.7% and elevated LDL in 44.4%. The prevalence of dyslipidemia at least one abnormal lipid fraction) was 90.7%. Ten diabetics (9.3%) had no dyslipidemia, 26 (24%) had single dyslipidemia and 72 (66.6%) had multiple dyslipidemia.Obesity was found to be common among the patients with dyslipidemia, 65.7% of the patients with dyslipidemia were obese or overweight. Although obesity was more prevalent in diabetics with dyslipidemia, this difference was not statistically significant (P=0.787). Females were found to be more obese than males 59.5% and 40.5% respectively. A total of 71.4% were hypertensives while 29.6% were normotensives. Characteristics of diabetics with duration of DM ≥10 years and <10 years are shown in [Table - 2]. Mean age, BMI, FBC, systolic BP, and diastolic BP were all higher in diabetics with duration ≥10 years but the differences were not significant (P>0.05 in all instances). Mean TC and TG were higher while mean LDLC and HDLC were lower in diabetics with duration of DM ≥ 10 years.These differences werehowever not significant. The distribution of dyslipidemia in the two groups of diabetics is shown in [Table - 3]; there were no significant differences in the lipid profiles in these groups. Discussion Dyslipidemia was found to be highly prevalent in this study (90.7%). This was similar to the observation in South Africa where a prevalence of 90.3% was reported. [14] Our results appeared relatively higher compared with earlier reports from Nigeria by AgbolaAbu et al.[15] They noted an overall prevalence of dyslipidemia of 60.5% among subjects of high socioeconomic class attending Igbinedion Hospital and Medical Research Centre Okada in Edo State, Southern Nigeria.Studies from JUTH North central Nigeria reported significantly elevated levels of lipids in diabetics compared to non-diabetics. [16] Our result however agree with Okafor et al. (82.6%) [17] whose study population was similar to oursadult type 2 DM patients in a tertiary health institution. Our subjects were not classified on socioeconomic class but being a referral tertiary center with a mixed category of social status, the increasing difference may be attributed to the underlying metabolic derangement marking diabetes mellitus.Diabetes mellitus has been associated with abnormal lipid profiles, and the presence of diabetes either alone or in combination with other factors such as hypertension and obesity have been significantly associated with dyslipidemia. [18] The increasing prevalence of dyslipidemia in this study may also be attributed to the current trend toward urbanization and adoption of western diet and lifestyle which have inadvertently resulted in the higher incidence of type 2 diabetes mellitus with its attendant metabolic abnormalities. The commonest lipid abnormality noted in this study was low HDLC (62%) followed by hypertriglyceridemia (56.5%). This is the common trend in most type 2 DM patients, and has been associated with high risk of CHD morbidity and mortality in this group of patients. Low HDLC appears to be the most important marker of dyslipidemia in Blacks compared to Whites. [19] Odenigbo et al. noted that in apparently healthy Nigerians of middle and upper socioeconomic class, mean HDLC was much lower than local and Caucasian values suggesting that it may be a marker of cardiovascular risk in this subpopulation. [20] Most diabetic patients do not have marked elevations in LDLC but they do carry levels high enough to lead to atherosclerosis. [21] The Cholesterol and Recurrent Events (CARE) trial. [20] and the LongTerm Intervention with Pravastatin in Ischemic Disease (LIPID) [22] trials both showed a positive role of aggressive LDL lowering therapy on recurrent CHD events in diabetics. The predominance of combined dyslipidemia noted in this study is comparable with other studies. [14],[15],[18] It is an indication of the need to aggressively treat dyslipidemia as each of these derangements has been noted to be independently atherogenic. [18] The mean lipid levels when compared with the illness duration were not found to be significantly different in this study. This is in contrast to a study done in Pakistan where the duration of DM was associated with a higher incidence of dyslipidemia. [23] The reason for this may be attributed to the patient′s characteristics. The Pakistan patients had a poorer level of glycemic control, with mean FBGsignificantly higher in patients with a longer duration of DM. Our study showed that mean FBG in illness duration>10 years and illness duration <10 years were 8.61 ± 2.64 and 8.18 ± 3.66 mmol/L respectively. Even though this could not be defined as good glycemic control, the difference was not as marked as in the Pakistan study. Various reasons such as ignorance, socioeconomic and false belief of treatments were proffered for the poor lipid and glycemic control noted among the Indianpatients. [23] AgboolaAbu et al. reported similar findings but noted that better glycemic control helped improve dyslipidemia among his patients. [24] It has also been reported that controlling dyslipidemia and good glycemic control delays atherosclerosis and prevents CHD. [24] Obesity is a known determinant of abnormal lipid profile. [6] Its high prevalence in this study (65.7%) may have contributed to the increase in dyslipidemia seen in our patients but when compared with illness duration there was no significant difference between the two groups. Earlier reports noted similar findings and suggested that this could add to the other driving forces responsible for the increasing prevalence of cardiovascular risk factors. [17] The mean BMI of patients in this study (28.37 ± 5.45 kg/m 2 ) was comparable with other reports from Nigeria and showed that abnormalities of weight are not only common among diabetic patients but also among healthy Nigerians. [25] In conclusion this study has shown that dyslipidemia (especially combined dyslipidemia and reduced HDLC is highly prevalent amongtype 2 diabetic patients in SouthEast Nigeria. This pattern of combined dyslipidemia, no doubt, predisposes them to increased risk of cardiovascular morbidity and mortality. Efforts should therefore be intensified in the area of glycemic control, lipid lowering and lifestyle modifications among others to reduce the risk of CHD in diabetic patients. Indeed the very high prevalence of dyslipidemia among diabetic subjects irrespective of duration of DM makes a case for early commencement of lipid lowering therapy even in the absence of biochemically proven dyslipidemia. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11060t1.jpg] [am11060f1.jpg] [am11060t3.jpg] [am11060t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}