 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 10, No. 4, October-December, 2011, pp. 290-293 Original Article Should non acute and recurrent headaches have neuroimaging before review by a Neurologist?- A review in a Southern Nigerian Tertiary Hospital Frank Aiwansoba Imarhiagbe1, Ehi Ogbeide2 1 Department of Medicine, University of Benin, Benin City, Nigeria Code Number: am11061 PMID: 22064255 Abstract Background: Headache is a common complaint in general practice and it is known that most headaches are primary and that the yield of neuroimaging like cranial computed tomography (CT) in headache is generally low. In this study, we were able to demonstrate that the yield of neuroimaging in non-acute and recurrent headache could be higher if cases are reviewed first by a specialist Neurologist before cranial CT.
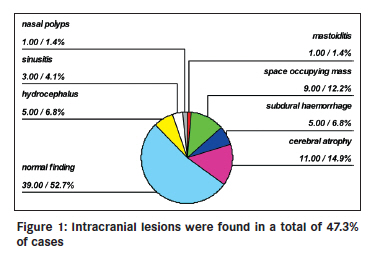
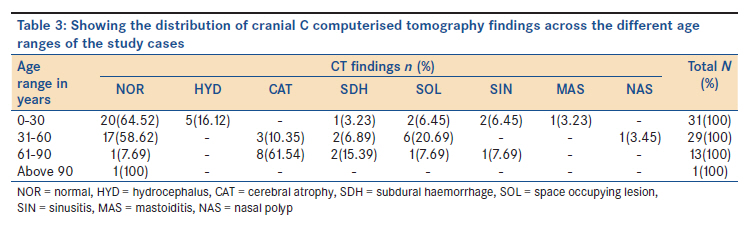
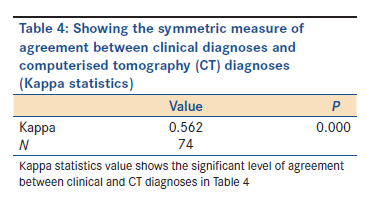
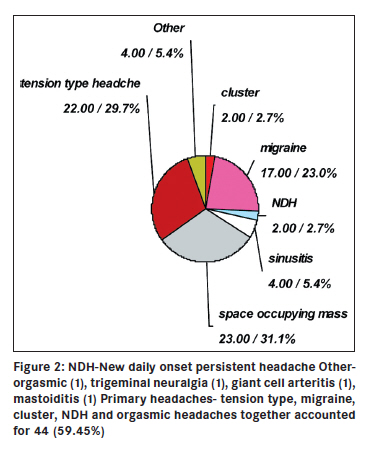
Keywords: Headaches, neurologist, tomography Introduction Headache is the commonest complaint in medical practice and it is known that most headaches are primary, but the fear of missing a potentially sinister secondary cause of headache among other reasons prompts the investigation of headaches with neuroimaging modalities like computerized tomography (CT) scan. The yield of neuroimaging in headaches is generally low particularly in cases of non traumatic, non focal, chronic headaches without neurological deficit. It is pertinent to note, however, that more often than not, the referrals for neuroimaging have been at the primary level of care. While it is standard practice to investigate acute and severe headaches promptly with neuroimaging to exclude potentially sinister causes, it is our opinion that less emergent, non acute, and recurrent headaches without clear cut diagnostic consideration by the International classification of Headache Disorders (ICHD) guidelines should be evaluated first by a specialist Neurologist before requests for neuroimaging. This may considerably increase the yield and also whittle down such requests with its corresponding cost implications particularly in resource-constrained settings. In this study, we were able to demonstrate that the yield for secondary causes of chronic headaches with cranial CT was considerably high after evaluation by a Neurologist. Materials and Methods Seventy-four (74) cases that were referred to the specialist Neurology clinic with complaints of chronic and recurrent headaches without focal neurological deficit that had CT scan were reviewed consecutively after their demographics of age, sex, and domiciliary were captured, to find out the proportion and characteristics of study cases that had identifiable cranial lesions on cranial CT scan. All cases were reviewed first by a specialist Neurologist using the short form of the ICHD 2 classification criteria for headaches before CT scan and CT was done with a two slice Siemens® 1994 third generation CT machine in the Radiology department of the hospital and all CT films were reviewed by a Specialist Radiologist. Exclusion - Cases with manifest focal neurological signs or manifest cognitive decline and established cases of headache following traumatic head injury. Study was approved by the Institutional Review Board (Ethics committee) of the hospital. Statistics - Demographic data of age and sex and the distribution of CT findings were described from a frequency table and mean age of study cases with and without identifiable lesions on CT were compared with an independent t-test for any significant difference and the effect of gender on the presence of identifiable lesions was also tested with chi square, clinical, and CT diagnoses were compared with Cohen′s kappa statistics for symmetric measure of agreement; P≤0.05 was taken as significant for all tests. Analyses were done with SPSS® version 16. Resulta The age range of study participants was 5-98 years with a mean age of 37.55(22.06) years. The female male ratio was 1:1.05 as shown in [Table - 1]. The effect of gender on the presence of identifiable lesions was not significant on a chi square test (χ2= 892, P=0.345) and identifiable intracranial lesions were found in 47.3% of cases while cases with normal CT findings accounted for 52.7%. as shown in [Table - 2] and [Figure - 1]. Intracranial lesions were more frequent in study participants with higher age range as shown in [Table - 3]. Clinical diagnoses and CT findings agreed in 56.2% of cases on kappa statistics as shown in [Table - 4] and [Figure - 2]. Discussion Headache is one of the commonest symptoms in general medical practice and it virtually affects all persons at some point. [1],[2] Primary headaches are by far commoner than secondary headaches. [3] The differential diagnoses of secondary headaches could be a legion and are very likely more numerous than for any other symptom. [3] The fear of missing a potentially sinister but treatable cause of headaches, coupled with patients′ anxiety and medicolegal reasons are usually what prompts the investigation of headaches with neuroimaging modalities like computerized tomography scan (CT). [4] Though neuroimaging has revolutionized the investigation of headache and headache syndromes in general, the low yield in non traumatic, non focal, chronic and recurrent headaches and the cost implication particularly in resource poor settings are well known. [5],[6],[7] Similar trends of low yield have also been reported in the emergency evaluation of acute non focal headaches in the emergency department and in one large series only 1.02% had clinically significant findings requiring a change of management on neuroimaging. [8] Criteria in headaches that are associated with intracranial pathology and serve as red flags for neuroimaging include presence of focal neurological symptoms or findings, abrupt onset, alteration of headache characteristics, increasing intensity and frequency, persistence despite analgesics and headaches that never alternates sides, among others. [9],[10],[11] The United States headache consortium- a group of acknowledged expert Neurologists and the European Federation of Neurological Societies′ (EFNS) Task Force on use of instrumentation in the diagnosis of headaches recommend neuroimaging in ambulatory (non emergency) patients with migraine only in the presence of persistent focal neurological findings or a history of seizures. [12],[13],[14] While cases of severe acute headaches should expectedly have emergency CT scan to exclude sinister causes like subarachnoid hemorrhage and space occupying lesions, in chronic and recurrent headaches and where the clinical signs are not clearly defined or are difficult to elucidate, the opinion of a Neurologist should advisedly be sought. [15] In this review, the mean age of cases was 37.55 (22.06) years, with a slight male sex preponderance and there was no significant effect of gender on the presence of identifiable cranial lesions [Table - 1]. We noted the preponderance of cases with normal CT findings (52.7%), and the mean age was significantly lower compared to cases with identifiable cranial lesions, (P=0.019) [Table - 2], [Table - 3] and [Figure - 1], suggesting that advancing age may be an indication for neuroimaging in chronic headaches. A related study found that identifiable lesions were commoner in those above 40 years of age. [16] Of the cases with demonstrable cranial lesions (47.3%), relatively benign conditions like mastoiditis, sinusitis, nasal polyps, and cerebral atrophy accounted for 21.7% while surgically correctable causes of headaches like space occupying lesions, subdural hematoma, and hydrocephalus accounted for 25.6% [Figure - 1]. We consider the proportion of cases with cerebral atrophy alone (14.9%) as the only finding on cranial CT remarkably high in a subset of cases without manifest cognitive decline. Though this has been reported previously, its clinical significance in chronic non traumatic headaches remains to be determined. [16] The relatively high yield of cases with identifiable cranial lesions (47.3%) may have been influenced by the method of selection, in which all the cases reviewed were referred for CT after assessment by a specialist Neurologist. The cases with normal CT findings were dominantly cases of primary headaches-migraine, tension type, new onset daily persistent headaches and trigeminal autonomic cephalgias like cluster headaches that either became more severe in intensity or less responsive to previous medications which prompted neuroimaging. Clinical diagnoses agreed with cranial CT findings significantly in 56.2% of cases, P=0.000 [Table - 4] and [Figure - 2], this again may largely derive from the method of selection of cases for CT. We therefore conclude that in chronic and recurrent headaches without focal neurological deficit, normal cranial CT findings predominate and more importantly the yield for identifiable intracranial lesions may be higher if cases without clear cut diagnoses are reviewed first by a specialist Neurologist before cranial CT scan is requested. It is our opinion that this may considerably whittle down the request for neuroimaging and the corresponding cost implication particularly in resource-constrained settings. [17] Acknowledgement We appreciate the contributions of supporting staff of the department of Radiology, University of Benin Teaching Hospital, Benin City, Nigeria. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11061f1.jpg] [am11061t1.jpg] [am11061t3.jpg] [am11061t4.jpg] [am11061f2.jpg] [am11061t2.jpg] |
| |||||||||

{kind=link}
![Table - 2]](/showimage?am/photo/am11061t2.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}