 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 10, No. 4, October-December, 2011, pp. 305-309 Original Article Maternal and fetal outcome in patients with eclampsia at Murtala Muhammad specialist Hospital Kano, Nigeria Ibrahim A Yakasai, Sule A Gaya Department of Obstetrics and Gynaecology, Aminu Kano Teaching Hospital Kano, Nigeria Code Number: am11064 PMID: 22064258 Abstract Background/Objectives: Eclampsia is a major contributor to maternal and perinatal mortality worldwide. It is much more common in developing countries like Nigeria where presentation is usually late and resources are scarce. The staggering figures of maternal death (46%) reported by the Society of Obstetricians and Gynaecologists of Nigeria (SOGON) in 2004 moved the Kano State government to initiate programs that will reduce maternal mortality in the state. The objectives of this report were; 1) to determine the prevalence of eclampsia at Murtala Muhammad Specialist hospital (MMSH) Kano between April 2008 and May 2009; 2) to determine maternal and fetal outcome in eclamptic patients admitted to MMSH Kano between April 2008 and May 2009.
Keywords: Eclampsia, maternal, fetal, outcome Introduction Eclampsia is a disease that continues to be of significant concern, and hypertensive complications of pregnancy including eclampsia remain a leading cause of maternal death. [1] It is a major contributor to maternal and perinatal morbidity and mortality worldwide and this is more so in developing countries like Nigeria where presentation is usually late and facilities for resuscitation are scarce. [1],[2] It contributed up to 31.3% by a population-based survey of maternal mortality by Adamu et al. [3] and also 46% of maternal death in Kano according to Society of Obstetricians and Gynaecologists Of Nigeria (SOGON) NEEDS assessment survey in 2004. [4] The incidence varied worldwide ranging from 1 in 100 to 1 in 3 448 pregnancies. [5] In Nigeria, rates varies between 0.3/100 deliveries in Calabar, Southern Nigeria, to as high as 9/100 deliveries in Birnin Kudu, Northern Nigeria, and in general, the rates are higher in the North than in the South. [6],[7],[8][,9],[10],[11] Eclampsia usually develop following pre-eclampsia that can be detected and managed before the onset of convulsion, except in a few cases where convulsion occur without the onset of detectable pre-eclampsia. [11] The staggering figure of maternal mortality reported in 2004 by SOGON moved the Kano state government to initiate programs that will reduce maternal mortality in the state. Among these programs are expanding the ongoing free maternity services to include free Mgso 4 for eclamptic patients and intensive manpower recruitment posted to man strategic hospitals in the state, in order to reduce the delays in reaching the specialist hospital. This research is intended to find out the impact of these programs in terms of maternal and perinatal outcome among eclamptic patients in one of the largest maternity section in West African subregion, with average of more than 10 000 deliveries per annum and close to 1 000 cases of eclampsia per annum. The hospital receives referrals from all the local governments of the state and also from neighboring states like Jigawa, Bauchi, and parts of Katsina states. All the patients were managed using Mgso 4 . Patients with antepartum eclampsia were induced using misoprostol, except in patients with obvious indication for Caesarean section like those with cephalopelvic disproportion, fetal distress, or patients with previous scar and unfavorable cervix. There were no initial published data to compare the findings from this study, but attempt will be made to compare the findings with available figures within and outside Nigeria. Aim / objectives
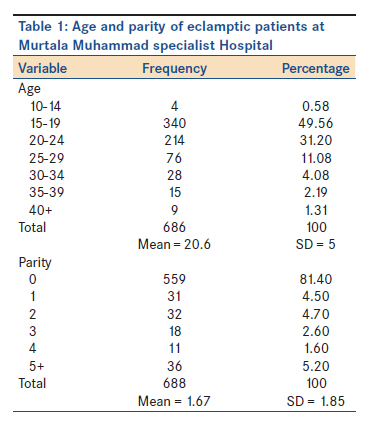
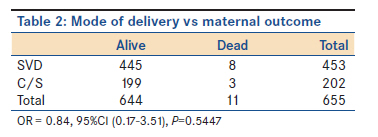
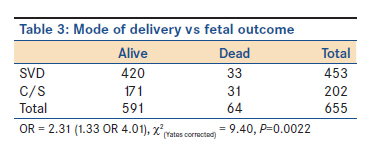
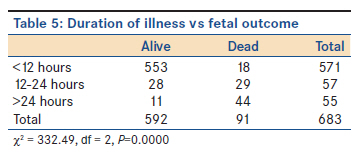
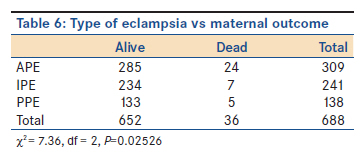
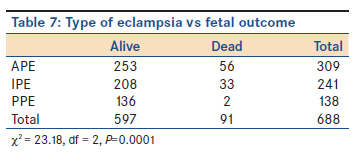
Materials and Methods All the cases of eclampsia admitted at the Hospital between May 2008 and April 2009 were identified and their case notes retrieved from the medical records. Information extracted include age, parity, booking status, gestational age, type of pregnancy, duration of illness before presentation, mode of delivery, maternal outcome, and fetal outcome. The data were analyzed using Epi info version 3.2.2 April, 2004 (CDC Atlanta, USA). The data were presented using tables and descriptive statistics were used as absolute numbers, measures of central tendencies, and measures of dispersion. The Chi-square test was used to test significant association. A P value of less than 0.05 was considered significant. Results There were 688 eclamptic patients admitted during the study period and there were 13 943 deliveries during the same period, giving an incidence of 5% of total deliveries. There were 126 maternal death during the study period, giving an MMR of 904/100 000 deliveries, and eclampsia accounted for 36 maternal death among them, thus contributing 28.57% of the maternal death and a case fatality rate of 5.2%. The perinatal mortality rate for the eclamptics was 132/1 000 eclamptic deliveries. Among them, 6.2% were fresh stillbirth, 3.5% were macerated stillbirth (MSB), and 3.5% were not delivered. Majority of the patients were teenagers (50.14%); mean age, 20.6 years; and standard deviation (SD) of 5. Primigravidae accounted for 81.4%, mean parity of about 2, and SD of about 2. These are shown in [Table - 1]. Up to 48.5% of the patients had some form of antenatal care, mostly at primary health centers. Majority of the patients (82.3%) were at term, 17.6% were preterm, and only one patient (0.1%) convulsed before fetal viability. Nearly half of the patients (44.9%) had their convulsion before the onset of labor, 35% were intrapartum, while 20.1% were postpartum. About 83.3% of the patients presented before 12 hours, while 8.5% and 8.2% presented between 12-24 hours and >24 hours, respectively.Up to 65.8% achieved vaginal delivery, 29.4% had Caesarean section, while 0.3% and 0.9% had forceps and vacuum deliveries, respectively. Twenty-five mothers (3.6%) died undelivered. Of the 11 mothers who died after delivery, eight had spontaneous vaginal delivery (1.8%), while three had Caesarean section (1.5). There is no significant difference in maternal outcome between those who delivered through spontaneous vaginal delivery and those who had Caesarean section (OR = 0.84, 95%CI = 0.17-3.51, P=0.5447), [Table - 2]. On the other hand, of the 64 stillbirths, 33 (7.9) were delivered through spontaneous vaginal delivery, while 31 (18.1%) were delivered through Caesarean section. There was significantly higher fetal loss among those delivered by Caesarean section than those delivered by spontaneous vaginal delivery (OR = 2.31, 95%CI = 1.33-4.01, χ2 = 9.40, P=0.0022), [Table - 3]. There were 51% males, 44.2% females, while sex has not been stated in the rest. There were 98.4% singleton pregnancies and 1.6% set of twins. No higher order pregnancy was reported. Maternal death due to eclampsia is shown to worsen when presented after 12 hours from the onset of convulsion (OR = 34.45, 95%CI = 13.16-95.36, χ2 = 119.10, P=0.000), [Table - 4], and similarly with perinatal mortality (OR = 57.51, 95%CI = 30.07-111.22, χ2 = 306.59, P=0.0000), [Table - 5]. Maternal mortality is worst with antepartum eclampsia (OR = 0.39, 95%CI = 0.18-0.83, χ2 = 6.37, P=0.0116), but there is no significant difference in terms of maternal outcome between intrapartum eclampsia and postpartum eclampsia (OR = 1.26, 95%CI = 0.34-4.51, χ2 = 0.01, P=0.9365), [Table - 6]. The fetal outcome is best with postpartum eclampsia compared with either intrapartum eclampsia (OR = 10.79, 95%CI, 2.47-66.12, χ2 = 14.27, P=0.0002) or antepartum eclampsia (OR = 15.05, 95%CI = 3.53-90.56, χ2 = 22.03, P=0.0000), but there is no significant difference between antepartum eclampsia and intrapartum eclampsia in terms of fetal outcome (OR = 072, 95%CI = 0.4-1.17, χ2 = 1.65, P=0.1995), [Table - 7]. Discussion Eclampsia is one of the most dangerous conditions which those caring for pregnant woman and her fetus must deal with, especially because its onset can be dramatic, abrupt, and in many women without any warning. [12] The incidence of 5% is lower than the incidence quoted at Birnin Kudu, [10] near the study area, and Abuja [11] (all in Northern Nigeria) but higher than the figures quoted in the Southern part of the country. [4],[6],[7],[8],[9] The lower incidence of eclampsia in this study may be attributed to the availability of competent staff at strategic general hospitals around the state, thus intercepting most of the referrals from these areas. This is commendable as it showed clearly how commitment by government can affect the incidence of fatal conditions like eclampsia. The contribution of eclampsia to maternal mortality (28.57%) has also declined considerably, compared with 46% reported in 2004 by the SOGON. [4] This decline may be due to the use of MgSO 4 in the treatment of the eclamptic patient, as shown in the Abuja study [11] and the MAGPIE Trial, a randomized controlled trial that clearly demonstrated the efficacy of MgSO4 in the control of eclamptic seizures. [13],[14],[15] The age and parity distributions were similar to other findings in Nigeria. [6],[7],[8],[9],[10],[11] The booked patient accounting for up to 48.5% is higher than most of the studies across Nigeria. This may be explained by the fact that most of the patients were within Kano metropolis and many of them might have booked at primary health centers. Most of these primary health centers do not have sphygmomanometer to measure blood pressure as such preeclampsia will go undetected. Delay was only established in 8.2% (presentation after 24 hours). This is in contrast to the finding at Birnin Kudu where delay was established in up to 56% of the patients. [10] This may be due to ongoing health campaign, especially about eclampsia and other causes of maternal death, as well as majority of the patients came from the city as mentioned earlier. The Caesarean section rate of 29.4% is much lower than the rates reported in many centers in Nigeria, but similar to some centers in the United Kingdom. [16] Most of the rates in Nigeria are more than 50%. [8],[9],[10],[11] This is because most of our patients had induction of labor with misoprostol while awaiting surgery and many progress satisfactorily and had spontaneous vaginal delivery. The long period taken before the surgery was due to very high patient-doctor ratio in the hospital. This was also noted by Jamilu tukur at Birnin kudu. [10] Multifetal pregnancy accounts for only 1.6% of the cases, which is much lower than 15.8% reported by Itam at Calabar [6] and 3.5% in the western world. [5] Case fatality rate of 5.2% is much lower than that reported by Efetie and Okafor at Abuja (28.3%), [11] Olatunji and Sule-odu (20%) [8] and Tukur et al. at Birnin Kudu (10.6) [10] but is higher than that reported by Umezuike et al. at Aba (2.5%) [7] where MgSO 4 was used in the treatment of the eclampsia. Case fatality rate of not more than 1% is needed to achieve MDG 5. This study showed gross reduction in overall MMR during the study period (904/100 000 births Vs >3 000/100 000 births recorded in 2004 by the SOGON NEEDS ASSESSMENT SURVEY). This may be explained by the gross reduction in the contribution of MM by eclampsia. The PNMR of 132/1 000 deliveries is similar to that found by Tukur et al. at Birnin Kudu and by Emen et al. at Uyo (130 and 137/1 000 deliveries, respectively) [9],[10] but lower than that reported from Gombe, [17] Kaduna, [14] and Aba [7] (368, 409, and 552/1 000 deliveries, respectively). The fetal outcome in this study was found to be significantly higher in intrapartum eclampsia/antepartum eclampsia compared with postpartum eclampsia; this is similar to what was found by Sinai and Anderson in America where they found the perinatal mortality remains between 75 and 85% in eclamptic patients with either antepartum/intrapartum eclampsia. [18] From this study, it is noted that maternal outcome is made worst when patients present after 12 hours from the onset of convulsion and when they have antepartum eclampsia. This emphasizes the importance of effective antenatal care, especially at primary health centers, where early onset pre-eclampsia will be detected and managed appropriately, so that these women do not go on and develop eclampsia. According to Royal College of Obstetricians and Gynaecologists (RCOG) guidelines, it is the most effective way to prevent eclampsia. [19] There was no significant relationship between maternal mortality and mode of delivery as such; it is worth trying vaginal delivery by induction of labor using misoprostol than to rush for Caesarean section. This will also reduce our Caesarean section rate. Similarly, fetal outcome in terms of survival is made worse by late presentation (>12 hours), antepartum eclampsia, and Caesarean section. The unfavorable outcome with Caesarean section may be explained by the fact that most of those that underwent Caesarean section had other complication that necessitated the Caesarean section (cephalo pelvic disproportion or fetal distress) and there was also delay in performing the Caesarean section due to inadequate man power. Olatunji and Sule-odu also noted no significant association between mode of delivery and maternal mortality, but noted a decrease in perinatal mortality with Caesarean section. [8] Conclusion The incidence of eclampsia at MMSH, Kano, was 5% of total deliveries. There was obvious decrease in the contribution of eclampsia to MM during the study period. Majority of the patients had successful vaginal delivery following induction of labor. Delay in presentation (after 12 hours) and antepartum eclampsia were associated with poor outcome in eclamptic patients. Mode of delivery had no effect on the outcome of the eclamptics. Remarkable reduction in maternal mortality to achieve MDG 5 is possible once Government is committed in providing proper antenatal care, especially at primary health centers. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11064t5.jpg] [am11064t1.jpg] [am11064t4.jpg] [am11064t3.jpg] [am11064t6.jpg] [am11064t2.jpg] [am11064t7.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}