 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 10, No. 4, October-December, 2011, pp. 310-313 Case Report Disseminated Langerhan's cell histiocytosis: A case report and review of the literature Abdullahi Mohammed, Kabir Abdullahi, Umar Mohammed, Halima O Aliyu, Almustapha A Liman, Shehu Abdullahi, Halima M Bello, Nasiru Abubakar, M Abubakar, Karo C Akpobi, Usman B Mafara Department of Pathology, Ahmadu Bello University Teaching Hospital Zaria, Nigeria Code Number: am11065 PMID: 22064259 Abstract Langerhan's cell histiocytosis is characterized by the presence of large mononucleated cells associated with inflammatory cells. We describe the clinical presentation, histopathology and some immunohistochemistry findings, in an eight-year-old female patient.Keywords: Disseminated, langerhan′s cell histiocytosis, rare
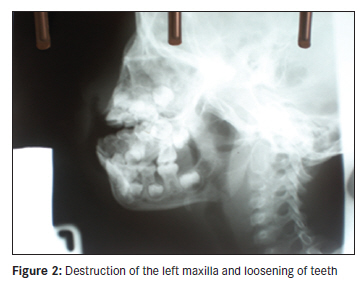
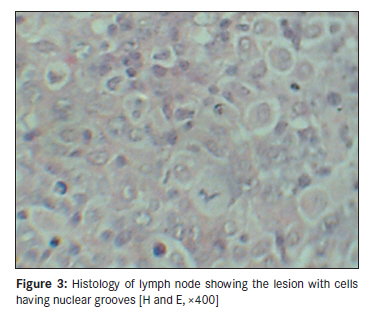
Introduction Langerhan′s cell histiocytosis (LCH) is characterized by the presence of large mononucleated cells, but occasional ones contain several nuclei, associated with inflammatory cells. Their nuclei are highly characteristic, irregular, usually elongated with prominent grooves and folds that traverse in all directions. The cytoplasm is abundant and acidophilic, sometimes to the point that an embryonal rhabdomyosarcoma is simulated. [1],[2] LCH embraces several previous eponyms, including histiocytosis X, Letterer-Siwe disease, Hand-Schuller-Christian disease, eosinophilic granuloma, and Hashimoto-Pritzker syndrome. [1],[3] It may involve the skin, bone, or may be disseminated to any organ. Hence extremely variable manifestations and an erratic course have made systemic study difficult. Many basic questions concerning the natural history, treatment, response to therapy, and prognosis remain unanswered. [4],[5],[6],[7] Although LCH was described a century ago [8] the prevailing opinion is that LCH is a reactive disorder rather than a neoplastic process, [9] although the possibility that LCH has a viral pathogenesis is of considerable interest. McClain et al., using molecular methods to detect the genomes of the Epstein-Barr Virus, human herpes virus Type 6, and seven other viruses, found no trace of viral DNA in 50 cases of LCH. [4],[10] Leahy et al., have implicated human herpes virus Type 6, but their study requires confirmation. [4],[11] Recent ultra-structural studies also found no evidence of the virus. [4],[12] However, the remote possibility remains that LCH could result from a virally induced clonal proliferation of dendritic Langerhan′s cells. [4] Case Report An eight-year-old girl presented with a four-month history of left maxillary swelling which was increasing gradually in size, there was associated toothache and palatal swelling which increased gradually and later ulcerated. There was associated history of fever, however, no trauma, chronic cough, loss of tooth or weight loss. Past medical and family history were not contributory. When examined patient was ill-looking, mildly pale, had finger clubbing and peripheral lymphadenopathy. On maxillofacial examination there was halitosis, asymmetrical facial swelling with an oral swelling extending from the left side of the face to the right side which was firm, tender, attached to the underlying tissue. There was gross disfigurement of the nose, areas of pus collection and almost complete occlusion of the right nose [Figure - 1]. Internal oral examination revealed areas of necrosis on the hard palate with soft palate involvement. There was gingival inflammation. Other systemic examination revealed liver and spleen enlargement (4 cm each). Laboratory investigations showed: Pack cell volume [PCV] 21%, White blood cell count [WBC]- 2.9 x 10 9 / L, platelet 145 x 10 9 / L , poikilocytosis +++, anisocytosis ++, neutrophils 63%, eosinophils 0.7%, lymphocytes 30%, and monocyte 2%.
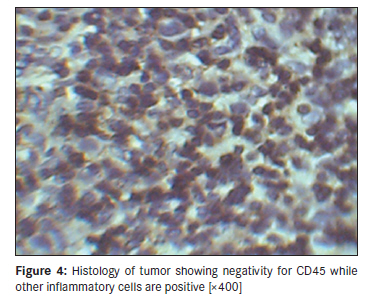
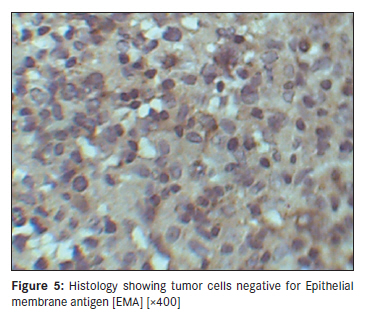
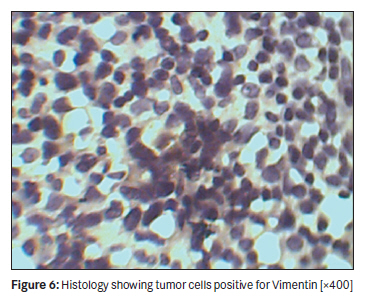
Outcome The patient was placed on medical treatment (ceproxin, prednisolone) for infections before being placed on a single course of vincristine (due to her poor clinical state). Three weeks post diagnosis, she had an accidental fall which led to profuse hemorrhage with thrombocytopenia, and her subsequent death from hypovolemic shock. Discussion LCH, an enigmatic disorder, has been variously classified as a neoplastic process, a reactive disorder, or an aberrant immune response. [4],[13] A wide spectrum of diseases and variable clinical behavior are characteristic. Although histopathological examination cannot predict clinical outcome, recent studies have shown that Langerhan′s cells within the lesions of LCH are intrinsically proliferative. [4],[14] There was an initial delay in diagnosis as she was being managed as a case of gangrenous stomatitis (Cancrum Oris). Following poor response to management, biopsy of a cervical lymph node and her bone marrow was done. This is a common occurrence as the varied presentation may mimic Rosai-Dorfman disease (RDD), parasitic infections, Kimura′s disease and some types of malignant lymphomas (Hodgkin′s lymphoma, peripheral T-cell lymphoma). Light microscopy of both tissues showed features of a malignant histiocytic tumor on Hematoxylin and Eosin-stained paraffin section. Although the most useful formalin-resistant epitopes for LCH are S-100 protein and CD1a, [2] these were not available in this centre, hence we performed immunohistochemical studies of the case using four clonal antibodies (cytokeratin, EMA, CD45 and vimentin) to differentiate the cell type. The tumor cells were found to be negative for CD45, EMA and cytokeratin. They, however, showed positivity for vimentin. [2] Considering her age and the generalized nature of her condition, our result confirmed disseminated LCH. Multisystem disease should be treated with systemic multi-agent chemotherapy. Several different regimens have been proposed, but a central element is the inclusion of either vinblastine or etoposide. [15] In this case, due to the frail condition of the patient and the unavailability of the recommended key drugs, vincristine was substituted. The response rate to therapy may be high, especially if the diagnosis is accurately and expeditiously ascertained. [15] Our patient, however, had many poor prognostic factors, ranging from delay in diagnosis to poor supportive therapy. Young patients with multisystem disease and poor response to initial therapy may benefit from immunosuppressive therapy, certain new agents (2-chlorodeoxyadenosine) and bone marrow transplantation. [15] Acknowledgment We acknowledge the assistance of the following people for their contribution in arranging the final manuscript: Dr. Tunde Talib Sholadoye, Registrar, Department of Surgery, ABUTH, Zaria, Nigeria and Mr. Lucky I. Aghemunu, Department of Histopathology, ABUTH, Zaria, Nigeria. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11065f3.jpg] [am11065f4.jpg] [am11065f5.jpg] [am11065f1.jpg] [am11065f6.jpg] [am11065f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}