 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
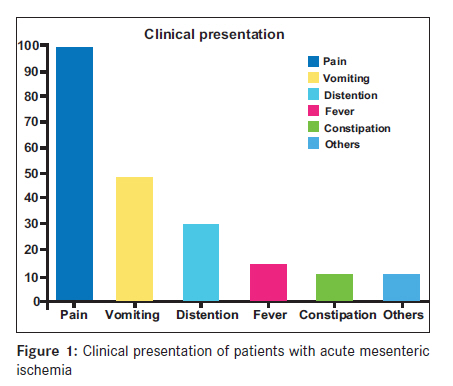
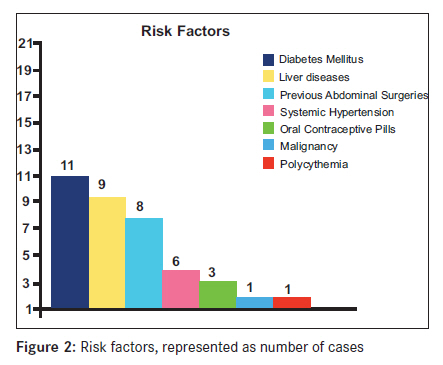
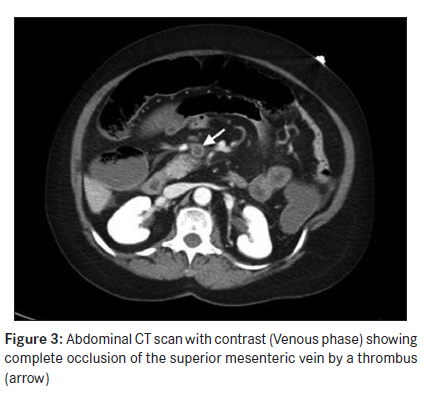
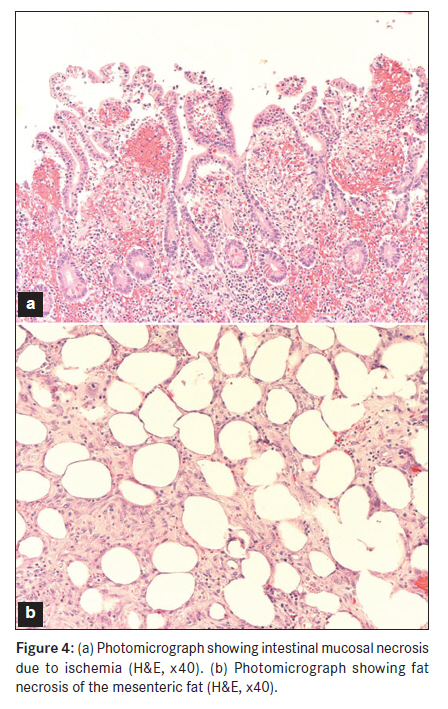
Annals of African Medicine, Vol. 11, No. 1, January-March, 2012, pp. 5-10 Original Article Acute occlusive mesenteric ischemia in high altitude of southwestern region of Saudi Arabia Mubarak M Al-Shraim1, Mubarak H Zafer2, Ganiyu A Rahman3 1 Department of Pathology, College of Medicine, King Khalid University, Abha, Kingdom of Saudi Arabia Code Number: am12002 PMID: 22199040 Abstract Background and Objectives : Mesenteric ischemia which can be acute or chronic depending on the rapidity of compromised blood flow produces bowel ischemia, infarction, bacterial transmigration, endotoxemia, multisystem organ failure and death. High altitude can precipitate thrombosis because of hypobaric hypoxia and its effect on coagulation system. The objectives of this study are to determine the risk factors, clinical presentation, type and pattern of acute occlusive mesenteric ischemia in high-altitude of southwestern region of Saudi Arabia.Materials and Methods: We reviewed the records of all the patients with acute occlusive mesenteric ischemia admitted to the Armed Forces Hospital, southern region, Kingdom of Saudi Arabia during the period of 2005 to 2010, and compiled data including demographics, clinical presentation, risk factors, preoperative investigations, management, histopathological examination, and complications. The cases of mesenteric ischemia resulting from conditions such as volvulus and strangulated hernias were excluded. Results: Our study included 21 patients, 10 (48%) men and 11 (52%) women with a mean age of 56 years (SD 14). Abdominal pain was the most common presenting symptoms. CT angiography depicted occlusive arterial disease in 8 patients (38%) and venous thrombosis in 13 patients (62%). Diabetes mellitus was the most frequent risk factor for arterial mesenteric ischemia. Chronic liver disease particularly liver cirrhosis was the most prominent risk factor for venous mesenteric thrombosis. Intestinal ischemia was confirmed by histopathological examination. Conclusion: Acute occlusive mesenteric ischemia can mimic other more common intra-abdominal diseases clinically; therefore a high index of suspicion is required particularly for patients with relevant risk factors to prompt early diagnosis and intervention. Venous mesenteric thrombosis was more common than arterial mesenteric ischemia in our region. Keywords: Acute mesenteric ischemia, high altitude, Saudi Arabia Introduction Acute mesenteric ischemia (AMI) results from sudden hypoperfusion of the intestines leading eventually to bowel necrosis. AMI can result from occlusive or nonocclusive obstruction of venous or arterial blood flow. AMI can be classified generally as arterial or venous disease. Arterial disease can be subdivided into nonocclusive mesenteric ischemia (NOMI), and occlusive mesenteric arterial ischemia (OMAI). [1] AMI is divided into 4 different primary clinical entities: acute mesenteric arterial embolus (AMAE), acute mesenteric arterial thrombosis (AMAT), NOMI, and mesenteric venous thrombosis (MVT). OMAI includes both AMAE and AMAT. [2],[3] NOMI is said to occur as a result of splanchnic hypoperfusion and vasoconctriction. [4] The common end point in both acute arterial or venous mesenteric ischemia is a pathophysiological derangement that results in intestinal necrosis. AMI is a potentially lethal disease due to delay in establishing the diagnosis by virtue of its nonspecific clinical presentation which varies greatly. Patients can present with symptoms and signs compatible with and mimicking other diseases such as pancreatitis, perforated peptic ulcer or peritonitis. As intestinal ischemia progresses from reversible to irreversible cell injury, metabolic disturbances ensue, therefore late diagnosis can lead to multiple organ dysfunction and death. The Aseer region (population of 1,200,000) lies in the southwestern part of Saudi Arabia, extending over an area of more than 80,000 km 2 . The area extends from the high mountains of Sarawat with an altitude of about 3200 m above sea level westwards to the Red sea, and southwards to the border of neighboring Yemen. [5] High altitude can precipitate thrombosis because of hypobaric hypoxia and its effect on coagulation system. [6],[7] The objective of this study is to determine the risk factors, clinical presentation and pattern of acute occlusive mesenteric ischemia in high altitude of southwestern region of Saudi Arabia. Materials and Methods In this retrospective descriptive study, we reviewed the hospital records of all patients with acute occlusive mesenteric ischemia admitted to the Armed Forces Hospital, southern region over a period of 5 years, from June 2005 to June 2010. Armed Forces Hospital of the Southern Region is a 334-bed tertiary health institution located in Khamis mushyte affiliated to the College of Medicine of King Khalid University, Abha and caters for all patients needing tertiary health care services not only the military personnel. Asir Central Hospital Abha (600-bed) also in the region is another tertiary health institution affiliated to the University and providing tertiary health care to the populace in the region. Khamis mushyte is about 25 kms from Abha. We excluded cases of AMI caused by conditions such as strangulated hernia, volvulus, or intestinal adhesions. Data extraction was achieved using a standardized form. The data included age, gender, clinical presentation, risk factors, initial laboratory investigations, mesenteric CT angiography with contrast, histopathology result, management and complications arising within 30 days of patient′s presentation. Laboratory data that were taken into account included hemoglobin level, red and white cell counts, platelets, and coagulation profile performed at the presentation of symptoms. The statistical analysis of the data was performed using SPSS® for Windows (Version 17.0). This study was approved by the Research Ethics Committee of College of Medicine- King Khalid University and by the Research Ethics Committee of Armed Forces Hospital, southern region. Results A total of 21 patients with acute occlusive mesenteric ischemia were included. The age ranged from 38 to 74 years with a mean age of 56 [SD 14] years, with 10 males and 11 females (male female ratio of 1:1.1). The presenting symptoms and their frequency summarized in [Figure - 1]. The most frequent presenting symptom was abdominal pain which was recorded in all cases, followed by vomiting in 12/21 (57%), abdominal distension in 8/21 (38%), fever (Temperature > 38.3 0 C) in 4/21 (19%), constipation in 3/21 (14%) and melena in 3/21 (14%) patients. The pain was epigastric in 11/21 (52%) and generalized in 10/21 (48%) of patients. [Figure - 2] summarizes the presence of risk factors found in this series. Many combined risk factors were detected from the patients′ medical records. These risk factors included diabetes mellitus in 11/21 (52%), liver diseases in 9/21 (43%), previous abdominal surgeries (caesarian section, hysterectomy) in 8/21 (38%), systemic hypertension in 6/21 (29%), oral contraceptive pills in 3/21 (14%, the patients on oral contraceptives were aged 38, 40 and 43 years), malignancy in 1/21 (4.7%), and secondary polycythemia to chronic obstructive pulmonary disease in 1/21 (4.7%). The malignant case was hepatocellular carcinoma. Laboratory investigations that were analyzed included the initial results on admission; the mean hemoglobin was 11.8 g/dl (SD 3.6), white cell count of 10.5x10 3 (SD 6.9), platelets of 194x10 3 (SD72.6), prothrombin time (PT) was 21 second (SD 15.3), partial thromboplastin time (PTT) of 34 second (SD 15.3) and INR of 1.4 (SD 0.5). All the patients had abdominal CT angiography with contrast and revealed mesenteric venous thrombosis in 13/21 (62%) patients, and mesenteric artery thrombosis in 8/21 (38%) patients [Figure - 3]. There were no cases in the categories AMAE and NOMI. There was no patient with previous ischemic cardiac disease or atrial fibrillation or peripheral vascular disease. One of the patients with cirrhosis of the liver had a history of portal hypertension. Overall, 18/21 (85%) of patients underwent surgery for resection of the affected bowel segment. Most of the patient received postoperative heparin followed up by warfarin anticoagulation therapy. All of our patients received intravenous antibiotics, a regime of metronidazole and third generation cephalosporin. All the resected bowel segments were examined histopathologically and the bowel ischemia and necrosis were confirmed [Figure - 4]a and b. The complications that were recognized within 30 days of patient′s presentation included short bowel syndrome in 12/21 (57%) patients, septicemia in 6/21 (29%) of cases, and enterocutaneous fistula was detected in two cases. The fistulas were from anastomotic leak and they closed spontaneously. One patient died within 1 month after the establishment of the diagnosis due to multiorgan failure. Discussion AMI was seen in less than 1 in every 1,000 hospitalized patients in the United State of America. [3],[8] It affected female more slightly than male in our study, and we found mesenteric venous thrombosis was more common in female patients than in male patients. Other studies showed that females were usually affected three times more than male. [9] Interesting for mesenteric venous thrombosis (MVT) in some studies, [10],[11] males were reported to be affected more than females, and this was considered as unusual as the realm of MVT was usually of a female predominance which was the case in our series. The usual affected age was reported to be 60-70 years. [8] However in our study the affected age ranged from 38 to 73 (mean age of 56 years) and this could be related the difference in the regional risk factors. The overwhelming risk factor for MVT was liver cirrhosis (9/21). All the patients with liver cirrhosis resulted from chronic viral hepatitis. This is similar to a previous study by Al Salamah and Mirza. [12] On the other hand diabetes mellitus was the most frequent risk factor for arterial mesenteric thrombosis. Diabetic mellitus is a high risk factor for the development of atherosclerosis and therefore ischaemic vascular disorder. On closer examination of our data it was interesting to notice that the patients with MVT were the younger group and usually had multiple risk factors. In one case of MVT the patient had liver cirrhosis, portal hypertension, in addition to previous hysterectomy for ruptured uterus, in another case of MVT the risk factors were use of oral contraceptive pills and two previous Cesarean sections. Expansion of our knowledge about the regional risk factors for AMI can enhance the understanding of the pathophysiologic changes which results ultimately in bowel ischemia and necrosis [Figure - 4]. The effect of living in high altitude was investigated in southwestern region of Saudi Arabia for many diseases such as stroke, [13] deep venous thrombosis, [14] hypertension, [15] sick cell disease, [16] and gallstone; [5] The frequency of thrombotic stroke at high altitude was 93.4% as compared to 79.3% at low altitude. The odd ratios (OR) for the different risk factors at high and low altitude, respectively, were hypertension 4.4 and 2.1; diabetes mellitus 2.7 and 1.9; and ischemic heart disease (IHD) 2.4 and 1.9. [13] The effect of high altitude on AMI is not yet fully investigated in our region, and the published data even was limited. [17] AMI is caused by arterial thrombosis more than venous thrombosis in many parts of the world, [18],[19],[20],[21] while MVT was a more common cause of AMI in our region than arterial thrombosis, this can be related to the different regional risk factors. Most high altitude-associated diseases occur above 8000 ft (2400 m). 2 In southwestern region of Saudi Arabia with an altitude of about 3200 m above sea level, high altitude may precipitate thrombosis because of hypobaric hypoxia and its effect on coagulation system--- in particular, increased factor VIIa activity. [6],[7] Dehydration, polycythemia and vascular spasms may also be involved in the increased tendency to mesenteric thrombosis at high-altitude area. [7] The clinical presentation in our cases included abdominal pain, vomiting, distension, constipation, fever and others such as melena. These symptoms varied greatly by duration, and severity in each case. Clinically these symptoms can mimic the presentation of more common diseases such as cholecystitis, appendicitis, and peptic ulcer disease; therefore the index of suspicion for these uncommon disorders should be high. AMI should be included in the differential diagnosis of any patient older than 50 years who presented with abdominal pain and had a relevant risk factor. The diagnosis can be difficult as the routine laboratory investigations are nonspecific with the most common abnormalities including leucocytosis, acidosis which reflected the metabolic derangement associated with bowel ischemia. [22] More recent study [23] showed that intestinal fatty acid binding protein (I-FABP) was characteristically high in cases of AMI and could be used as a diagnostic test; however, the practical clinical experience of this test is still lacking. All our cases were investigated using abdominal biphasic CT with mesenteric angiography. The overall sensitivity for the diagnosis of VMT was near 90%, [18] while the sensitivity for the other types of AMI is usually less, furthermore radiologic evaluation of the smaller distal mesenteric vessels remains a challenge and difficult to identify. The management of each case was dictated by the patient′s clinical presentation and the attending surgeon′s decision. Resection and anastomosis was the most common performed surgical procedure in our series. It was difficult to use the site of pain to identify the extent of the pathology but patient with generalized pain had more extensive ischemia. Almost all of our patients received heparin followed by long-term warfarin. Suggested treatment for MVT include thrombectomy, [24] mechanical and pharmacologic percutaneous clot lysis. [25],[26] None of these was used in our patients. In spite of use of the standard antibiotics therapy, six cases developed septicemia and one case died within 30 days due to septic shock and multiorgan failure. Short bowel syndrome was the most common postsurgical complication and recognized in 12/21 (57%) of patients, while only two cases developed enterocutaneous fistula (9%). This is similar to findings in the literature. [10],[27] The mortality in AMI is usually high though the mortality in MVT is usually less than in MAT. Mortality in this study is 8%; this is similar to 7% reported by Warshauer et al., in 2001. [28] The low mortality in this study is probably as a result of the fact that patients that died before the diagnosis was established or definitive treatment instituted were not included. Conclusions AMI remains a potentially lethal disease due to its nonspecific clinical presentation leading to late diagnosis and treatment. Thus diagnosis is triggered based on high index of suspicion. Searching for the relevant risk factors can help to predict the diagnosis. Abdominal CT with contrast can be diagnostic for AMI and is useful to exclude other causes of abdominal pain. Knowing the risk factors is not only important in diagnostic work up, but also for prevention. Some risk factors can be avoided such as use of oral contraceptive pills for patients at increased risk of thrombosis. Diabetes mellitus is the most common risk factor for arterial thrombosis while liver disease, particularly cirrhosis, is the most common risk factor for MVT in this study. Acknowledgment We gratefully acknowledge the support of the administrative staff in College of Medicine, King Khalid University, and Armed Forces Hospital - Southern Region (AFH-SR), and the help of medical record staff in AFH-SR. References
Copyright 2012 - Annals of African Medicine The following images related to this document are available:Photo images[12002f1.jpg] [12002f2.jpg] [12002f3.jpg] [12002f4.jpg]The following images related to this document are available:Photo images[am12002f3.jpg] [am12002f2.jpg] [am12002f1.jpg] [am12002f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}