 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 11, No. 1, January-March, 2012, pp. 12-20 Original Article Social network as a determinant of pathway to mental health service utilization among psychotic patients in a Nigerian hospital Victor O Lasebikan1, Eme T Owoaje2, Michael C Asuzu2 1 Department of Psychiatry, University College Hospital, Ibadan, Nigeria Keywords: Alternative sources of care, psychotics, service utilization, social networks
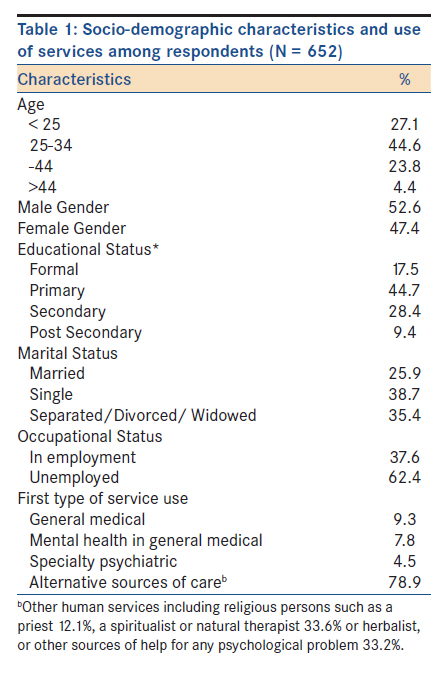
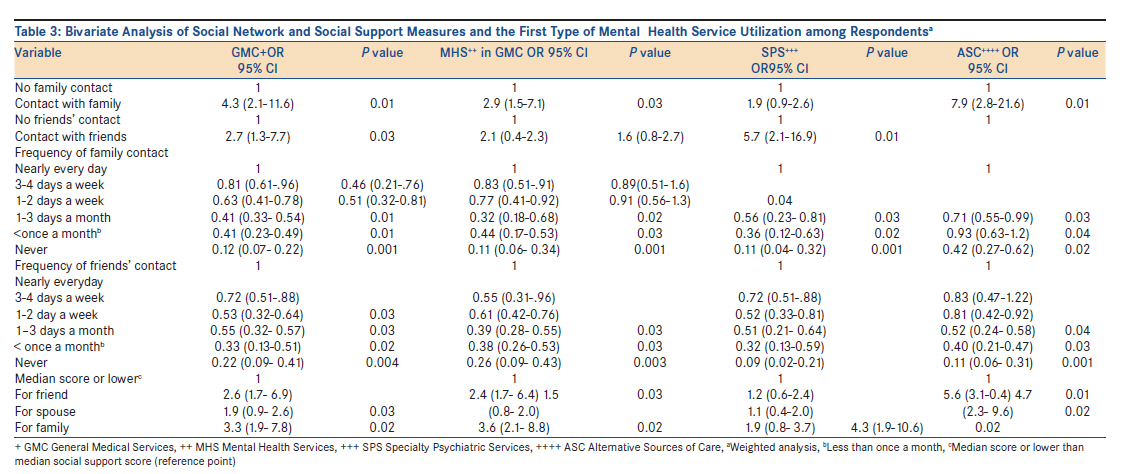
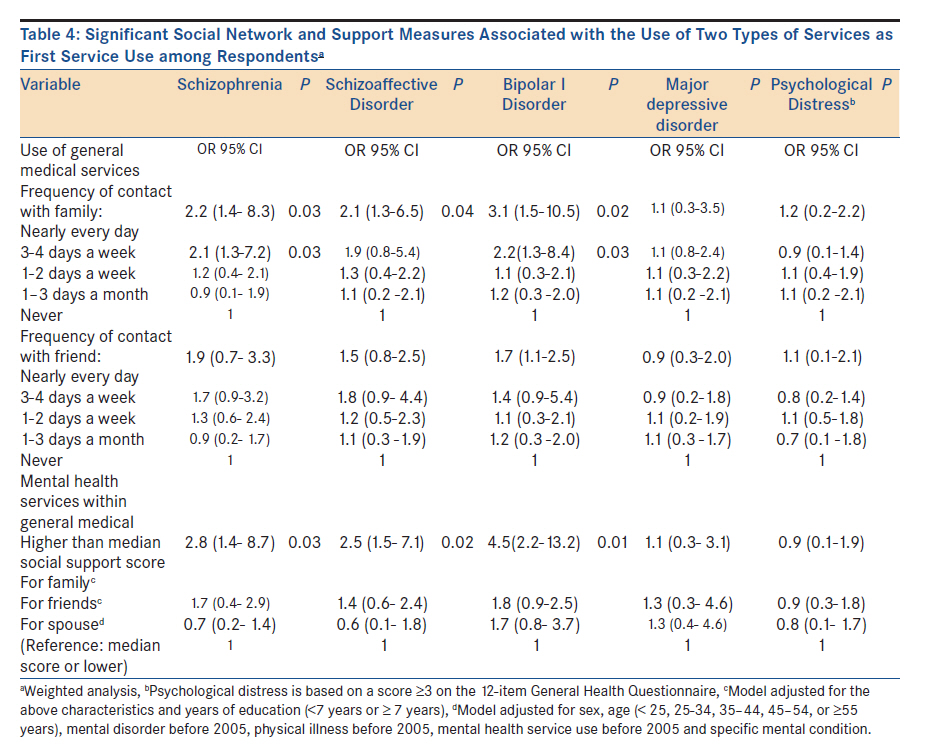
Introduction Studies have shown that only a minority of mentally unwell persons receive treatment in the healthcare system. [1],[2],[3],[4],[5] Recently, Pescosolido and Boyer [6] developed a model which influences the decision to use or continue with mental health services. The decision to utilize mental health service is determined by factors including symptom profile, severity and duration, nature of the mental disorder, [7],[8],[9] social network and support, health beliefs, perceptions of need of service, [10] attitudes as regards etiology, stigma, [4],[11],[12],[13] difficulty in discussing mental health problems, [14],[15] and the perceived or actual reactions of one′s family and friends. [16] The roles of social network and support in relation to mental disorders, stress, and mental health service utilization have been studied extensively. [17],[18] Social network is an important determinant of duration of untreated psychosis and entry into mental health service. [19] While social network is an objective concept corresponding to the number and frequency of contacts with support networks, social support is a more subjective concept of perceived support. Both network and support can act as coping resources. [20],[21] While some researchers opined that social support has a buffering effect on service utilization in stressful situations, [22],[23] others have found that a large number of close friends or relatives reduced service use as a direct effect. [9] In Nigeria, there is generally a high level of unmet need for mental health services. [24] However, there is a dearth of information on the extent to which social network contributes to utilization of mental health services in Nigeria. Objective: The objective of the study was to determine the influence of social network on the pathway to formal mental health service use among psychotic patients in a general hospital in a major city in South Western Nigeria. Hypothesis: Increased social network and social support from family would be associated with increased service use. Materials and Methods Setting The study was carried out at the outpatients′ department of the Psychiatric Unit of the State Specialists Hospital Ring Road Ibadan, Oyo State, Nigeria between January and December 2008. The catchment area of the study site was all the 33 Local Government Areas of Oyo State, Nigeria. This was because it is the only psychiatric unit in that state. However, patients from other surrounding states in the South West zone also utilize the resources. Sample Patients were selected based on the confirmation of a diagnosis of psychosis using the Structured Clinical Interview of DSM-IV Axis I disorder (SCID) [25] after an initial psychosis screening using psychosis screening questionnaire [26] administered to 980 consecutive patients who accessed the facility during the study period. Trained resident doctors administered the SCID which allowed a diagnosis to be made in accordance with DSM-IV criteria. Those with diagnoses of schizophrenia (368), schizoaffective disorder (70), mania with psychosis (137), and severe depression with psychosis (77) proceeded to the following stage, in which other instruments of data collection were administered to them. Effort was made not to duplicate respondents by endorsing their hospital attendance cards as they were interviewed. All patients were also quickly physically examined. Psychological Distress The 12-item General Health Questionnaire [27] was administered. A score of ≥3 was included in the statistical models to adjust for psychological distress within the past few weeks of the interview. Demographic characteristics and health status Information was collected from the sample regarding demographic characteristics. This included age, sex, marital status, years of education and presence of physical illnesses (for example, diabetes mellitus, heart trouble, hypertension, or arthritis) before 2008. Exclusion criteria A threshold of three years was set and any patient whose illness was over three years was excluded. Also excluded were patients with severe physical illnesses. Measures The interviews were carried out by resident doctors in the specialty of psychiatry who assessed the following constructs as detailed below. Interview was conducted in English language. For non-English-speaking respondents, questionnaires were translated to Yoruba (the language of instruction in the majority of respondents) and back translated into English to ascertain that the original meaning was maintained. Information obtained from the patients was corroborated by that obtained from whoever accompanied the patient to the hospital. Whenever it was suspected that such a person could not give reliable information either, another relative or the principal person that dominated such a patient′s social network was interviewed at a later date in order to obtain additional information. Social network Social network was assessed by using the Social Network section of the World Mental Health (WMH) CIDI. [28] The social network section of the WMH CIDI asked questions about the frequency of the patient′s contact with family members, who were not living with him/her including visits, phone calls, letters or electronic mail messages, and frequency of patient′s contact with friends. The social network section of the WMH CIDI also received information on the respondents′ perceived quality of support from relatives, friends, spouse/partner and any other person in the past six months. Possible summary scores range from 6 to 30, with lower scores indicating better quality of perceived support. Mental health service use Information was sought on care-seeking behavior in the six months prior to first contact with this psychiatric facility and on current multiple service use This consisted of four sections: (i) general medical services (any care from a health professional), (ii) mental health services within the general medical system (use of a medical doctor or hospital emergency room for emotional, mental health, or drug- or alcohol-related problems), (iii) specialty psychiatric services (use of a mental health specialist in either a private practice, mental health center, psychiatric outpatient clinic in either a general or psychiatric hospital), and (iv) alternative sources of care (consulting a religious person such as a priest, family or social service, a spiritualist or natural therapist or herbalist, or other sources of help for any psychological problem). The questions asked about pathway to care and first type of service use before contact with the current facility. Although the study was designed to assess the influence of the social network on the pathway to mental health service, subjects recruited for the study were not limited to first-episode psychosis in order to determine those who currently utilize multiple mental health services. Ethical Issues Participants provided written informed consent and the construct of the study duly explained to the them that the study was not part of routine clinical consultation. All data collection procedures were approved by the Epidemiological and Ethical Review Committee of the Ministry of Health, Oyo State, Nigeria. Analysis Analyses were performed with the SPSS Version 13.0. [29] Data were weighted to adjust for the probability of selection into the sample and non-response rates. During bivariate analyses, the association between specific measures of social network and social support and use of any of the above four groups of mental health services as first choice before the study period was assessed. For multivariate analyses, the relationship between specific measures of social network and social support and use of first choice of service were assessed for the four mental disorders and for psychological distress for variables showing significant association P < 0.05 during bivariate analysis. All models showing significant results for the predictors of primary interest (social network and support) were re-entered to determine the most parsimonious model. Models were adjusted for sex, age years of education, mental disorder before 2008, physical disorder before 2008. Results Mental disorders The presence of a psychotic disorder was determined among the 982 respondents after an initial psychosis screen, giving an unweighted prevalence of 66.4.0% (652 respondents). The cases included 368 who were diagnosed from SCID as suffering from schizophrenia of whom 305 (83.6%) reported past treatment for mental illness and 63 (17.1%) gave reports of past treatment for mental health problems, evidenced by the use of antipsychotics. Other DSM-IV diagnoses were schizoaffective disorder 70 (10.7), mania with psychosis 137 (21.0), severe depression with psychosis 77 (11.8), [Table - 1]. Sociodemographic Characteristics The mean age of the 652 respondents with psychotic disorders was 29.0 ± 7.5 years, range 14-58 years. Males constituted 52.6% of the sample. The mean number of years of education was 7.3 ± 2.5 years and only (25.9%) were married, the majority (62.4%) were unemployed [Table - 1]. Service use The pathway to mental health service was such that 78.9% of patients first utilized alternative sources of care (priests, spiritualists, natural therapists or herbalists) or other sources of help for any psychological problem. Ten percent currently use such alternative sources in conjunction with any formal mental health service. Less than a tenth (9.3%) of respondents utilized general medical service use as first type of service, 7.8% utilized mental health service within general medical setting as first type of service while only 4.5% utilized specialist psychiatric service as first type of service [Table - 1]. Social Network A little over half of patients (51.1%) reported contact with family nearly every day, a little over a third (34.7%) patients had contact with their friends nearly every day. Relatively fewer proportions of patients (11.8%) relied on family and friends or opened up to family and friends (10.7%) a lot. A lower proportion, (7.2%) relied on their spouses or partners or opened up a lot to spouses or partners (1.7%). Specifically, only 6.7% reported that husband/wife always knew their problems, [Table - 2]. Social network and social support measures and service use Factors associated with mental health services′ utilization were contact with either family or friends in general, conversely, a reduced frequency of contact with either family or friends was associated with reduced odds of accessing services across different mental health conditions. Furthermore, a higher than median level of social support from a relative, friend or spouse was associated with increased odds of utilizing any of the four services, most especially alternative sources [Table - 3]. Multivariate analyses [Table - 4] Contact with family nearly every day was significantly associated with increased odds of general medical service use for patients with schizophrenia OR = 2.2, 95% CI (1.4-8.3, P = 0.03), schizoaffective disorder OR = 2.1, 95% CI (1.3-6.5), P = 0.03, and bipolar I disorder, OR = 3.1, 95% CI (1.5-10.5), P = 0.02, but not with major depression and symptoms of psychological distress. Contact with family three to four days a week was significantly associated with general medical service use for patients with schizophrenia OR = 2.1, 95% CI (1.3-7.2, P = 0.03) and bipolar I disorder OR = 2.2, 95%CI (1.3-8.4), P = 0.03, but not with major depression and symptoms of psychological distress. Frequency of contact with friends was not significantly associated with any of the four services as first port of service. Also, higher than median social support score for family was significantly associated with increased odds of utilization of mental health services within general medical services for patients with schizophrenia, OR = 2.8, 95% CI (1.4-8.7) P = 0.03, schizoaffective disorder, OR = 2.5, 95% CI (1.5-7.1) P = 0.02, and bipolar I disorder, OR = 4.5, 95% CI (2.2-13.3) P = 0.01, but not with major depression and symptoms of psychological distress. Discussion The main objectives of the study were to determine the relationship between social network and pathway to service utilization among psychotic patients. We found that the majority of those who required services for psychotic disorders, irrespective of social network, sought treatment from alternative sources before any formal mental health setting. Although family constituted the strongest tie to patients in the study, the association between social network and social support and use of different types of health services was also found to vary across different mental health conditions as the presence of some social network and social support structures was significantly associated with the use of general medical and specialty psychiatric services for patients with schizophrenia, schizoaffective disorder, bipolar I disorder, but not with major depression and symptoms of psychological distress. Our findings supported the hypothesis that the association between service use and social network and social support varied across friends, relatives, and spouse, but contrary to previous studies [30],[31] the association between increased social network and social support and type of mental disorder varied. Specifically, these findings indicated that social network measures (for example, frequency of meeting relatives) were directly related to service use, such that less frequent contact was associated with reduced odds of accessing services. This finding contradicts that of Albert et al.,[23] which found that less social network or social support was generally associated with increased service use. However, our findings support more recent research that indicated that higher scores on a composite social network index (especially for contacts with relatives and friends) were associated with use of inpatient psychiatric services in local hospitals. [32] It is possible that for the alternative sources of services, one′s social networks and social support are more likely to suggest such services for early consultation because it carries fewer stigmas, and a supernatural cause is commonly believed within this society, which could require an alternative approach to its treatment. The location of such services within the community is more accessible than formal psychiatric services. This is also the case for general medical services which suggests that when symptoms first appear, the cause of illness is often unclear and one typically assumes physical rather than psychological factors as the causal agent. However, once the cause is identified as related to mental health, the use of even general medical services to discuss the problem is reduced and the services of "alternative practitioners" are sought. It is hypothesized that this might be a reflection of the stigma associated with more formal mental health services and mental health in general. [33],[34] Consistent with previous research, [23],[35] increased social network (that is, contact with more relatives and greater social support from friends and relatives) was associated with relatively less use of specialty psychiatric services compared with other forms of services (mental health service in a general setting and use of other human services), a result probably reflective of stigma on the one hand and preference for "alternatives sources of care" for the treatment, on the other hand. Generally, a network dominated by friends may offer lower social support compared with relatives; however, such a large number of contacts tend to provide more information about available services, thus encouraging help-seeking. [35] Although friends constitute weak ties, weak ties result in sharing of general information about multiple services and strong ties result in sharing of detailed information about fewer specific services. [36] The poor social support reported by spouses may be a reflection of unstable marriages and mere co-habiting in the absence of a legal marriage as observed in the course of the study, perhaps also due to the strain the psychotic illness had on the marriage. This study has also indicated that increased social support was associated with increased use of alternative sources of care irrespective of the type of social network, as seen in the unadjusted results. Weak ties (friends and spouses) were also strongly associated with utilizing non-formal care, a finding previously reported. [37] The findings that higher than median social support score for family was significantly associated with mental health services for patients with schizophrenia, schizoaffective disorder and bipolar I disorder but not with depression or symptoms of psychological distress indicate that having contact with a relative did not equate with seeking mental health attention for patients with depression or symptoms of psychological distress. The potential explanation being that depression is poorly recognized and under-diagnosed even among primary care practitioners [38],[39] and symptoms of psychological distress could be misinterpreted as those of physical illnesses. Our adjusted results also indicate that receiving social support from friends and spouses did not equate with seeking mental health service attention, for any type of mental health problem irrespective of the type of mental health problem suggesting that biological relatives still constitute the strongest ties in this environment. This study has illustrated the pathway to formal mental healthcare services in Nigeria in which irrespective of patient′s type of social network, alternative practitioners significantly constituted first contact with any mental health delivery. This underscores the need for their integration into mental health service delivery. A new finding in this study is that some individuals combine both formal mental health services with other alternative sources, an issue that is reflective of the level of relationship between such individuals and the alternative practitioners on the one hand and which constitutes the inability to determine the effectiveness of either approach on the other hand. It is important to consider some limitations when interpreting these findings. Reports on service use were self-reported, and respondents, in view of perceived failure of previously utilized services could have given false responses. Barriers to care and stigma were also not assessed. This could be explored in future research. It might also be difficult to generalize these findings to other populations across other cultures or countries. Our findings corroborate existing theories and suggest a need for further investigation of social support and outcomes. More research is needed on the impact of attitudes and knowledge regarding mental health, stigma, access to services, and religious beliefs, in combination with social support measures, to better understand the complex set of factors that influence service use. Although we adjusted for a number of factors, future research should also examine the buffering effect of factors such as gender, age, and out of pocket payment system for health services, on service use. References
Copyright 2012 - Annals of African Medicine The following images related to this document are available:Photo images[am12004t4.jpg] [am12004t3.jpg] [am12004t2.jpg] [am12004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}