 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
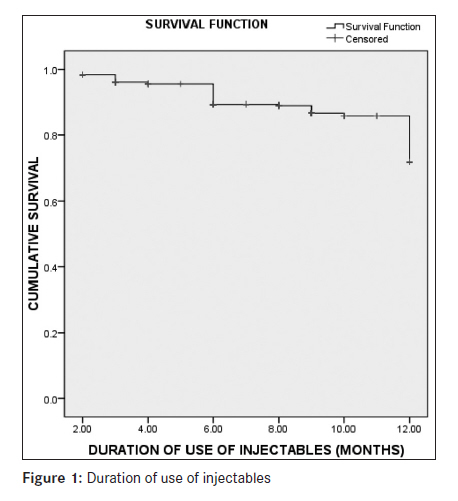
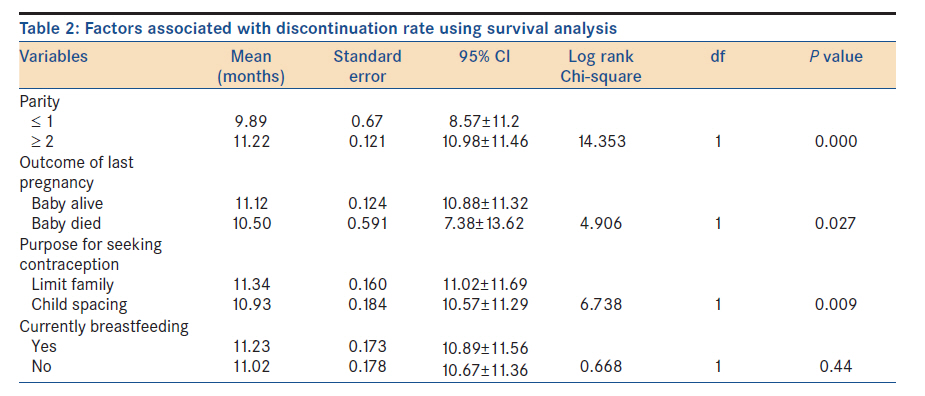
Annals of African Medicine, Vol. 11, No. 1, January-March, 2012, pp. 27-31 Original Article Progestogen-only injectable contraceptive: Experience of women in Osogbo, southwestern Nigeria AS Adeyemi, DA Adekanle Department of Obstetrics and Gynaecology, Ladoke Akintola University of Technology Teaching Hospital, Osogbo, Osun State, Nigeria Code Number: am12006 PMID: 22199044 Abstract Background: Progestogen-only injectable contraceptive is a long-acting contraceptive given intramuscularly to give protection against unwanted pregnancy for a period of 2 or 3 months, depending on the type. Alterations in menstrual pattern are a well known side effect of this effective contraceptive method.Objectives: To determine the characteristics of women accepting the method, complications and indications for discontinuation. Materials and Methods: This was a retrospective review of clients using progestogen-only injectable contraceptive between 1 st January, 2001 and 31 st December, 2009. Relevant information extracted from the case notes was analyzed. Survival analysis was carried out using Log-Rank Chi-square test to measure association over 12-month period of usage. Level of significance was set at P value less than 0.05. Results: A total of 1,967 women used contraception during the study period and 433 (22.1%) made progestogen-only injectable their method of choice. 199(45.96%) used NET-EN, while DMPA was used by234 (54.04%) women. Many of the women (197, 45.5%) used the method for terminal fertility control. Menstrual abnormality was the commonest (264, 71.4%) complaint about progestogen-only injectable contraceptive, of which amenorrhea was experienced by constituted 176(66.7%). Eighty-three (22.4%) women had discontinued the contraceptive, and menstrual abnormality was the commonest reason for the discontinuation (68, 81.9%). No pregnancy was reported among the women that came for follow up while on the method. Conclusion: Short duration of POIC use that is within 12 months is still high. However the main reason for discontinuation was found to be due to menstrual irregularities, hence the need for effective education of the women about this side effect, thus increasing the acceptance and continuation rate of the contraceptive method. Keywords: Complications, discontinuation, progestogen Introduction Progestogen-only injectable contraceptive (POIC) is a long acting contraceptive given intramuscularly to give protection against unwanted pregnancy for a period of 2 or 3 months, depending on the type. There are two commonly used injectable progestogen-only contraceptives that have been available in many countries in the world since 1983. [1] These are depot medroxyprogesterone acetate (DMPA) and norethisterone enanthate (NET-EN). DMPA is a synthetic progesterone derived from progesterone, administered at the dose of 150mg every 90 days. The mechanism of action is centrally exerted at the hypothalamic level, with complete block of ovulation. [1] NET-EN is administered at the dose of 200mg every 60 days, and inhibits fertility through a mixed, two-phase mechanism: during the first portion of the drug′s half-life span the contraceptive effect is exerted at the hypothalamic level, whereas later on when ovulation is restored, the action is likely to be peripheral on the cervical mucus and/or the endometrium. [1],[2] Both the progestogens are extremely effective in preventing pregnancy, with a pregnancy rate close to zero. [3],[4] Injectable progestogen only contraceptive is associated with multiple side effects, with secondary amenorrhea being the most common; others are hypertension, and weight gain. [4],[5],[6] For most teenagers requesting contraceptive, injectable could be a good option. They are independent of intercourse and of the user′s memory (and thus of continuing motivation), other than remembering the 8- or 12- weekly appointments. [7] Injectables offer the advantage of not requiring storage (making them suitable for use in the tropical countries like Nigeria) and not being obvious in use, enabling women to maintain secrecy about their use of contraception, because members of their families may oppose the concept of birth control. [8] POIC is associated with early discontinuation, and there is paucity of information on factors associated with this, thus this study was to evaluate these factors. Materials and Methods Ladoke Akintola University of Technology teaching hospital serves Osun state, and the neighbouring Oyo, Ekiti, Ondo and Kwara states. The family planning method services available in the hospital are: intrauterine contraceptive device (copper-T), injectable contraceptives, barrier methods, oral contraceptive pills, subdermal implants, male and female surgical sterilization. Counseling services is also available at the family planning clinic which is run Monday to Friday. Women pay for the commodity received. DMPA and NET-EN, cost one hundred naira (less than 1 US dollars) for a dose, while IUCD cost one hundred and fifty naira for an insertion, and the combined oral contraceptive pills is being sold for fifty naira per sachet. This study was a retrospective review of the case notes of all the women using progestogen only injectable contraceptive between 1 st January, 2001 and 31 st December, 2009. Information retrieved from the case notes includes socio-demographic status of patient, complications in the last pregnancy before the injectable contraceptive, duration of use, complaints about the contraceptive, and reasons for discontinuation. These were entered into SPSS work sheet and data was analyzed using statistical package for social sciences version 15(SPSS 15.0). Categorical variables were summarized using proportion and percentages while continuous variables were summarized using mean and standard deviation. Survival analysis was carried out using Log-Rank Chi-square test to measure association over a 12-month period of usage. Level of significance was set at P value less than 0.05. Results One thousand nine hundred and sixty-seven women accepted a modern method of contraceptive at the institution family planning clinic during the study period. Most of the women (1,376,70.2%) chose intrauterine contraceptive device (IUCD), while 433 (22.1%) made progestogen-only injectable their method of choice [NET-EN-199(45.96%), DMPA-234 (54.04%)]; 85 (4. 3%) accepted oral pills, while 37(1.9%), 21(1.1%), 14(0.7%), and 1(0.1%) chose monthly injectable, subdermal implanon, condom and tubal sterilization respectively. The age of the women who accepted progestogen-only injectable contraceptive ranged between 20 and 55 years with a mean of 34.04years (SD±5.68), their parity ranged between 1 and 9 with a mean of 3.54(SD±1.52), and their weight was between 38 and 98kg with a mean of 60.74kg (SD±9.87). Most of the women (370, 85.4%) who accepted the method had secondary and tertiary level of education, while only 9 (2.1%) had no formal education [Table - 1]. One hundred and ninety-seven (45.5%) of the women used the method for terminal fertility control, and 192(44.3%) for child spacing, while 44(10.2%) were not sure if they wanted more children. Two hundred and fifty-four (58.7%) of the women who accepted POIC had previously used a form of contraceptive, while 179(41.3%) had never used any form of contraceptive; only 80(31.5%) had previously used injectable, while the rest (174, 68.5%) had used other methods. At the time of this review, 370(85.5%) of the women were on regular follow-up, while 63(14.5%) had been lost to follow-up; ninety-eight (26.5%) of the women on regular follow-up had no complaint about the method. Menstrual abnormality was the commonest (264, 71.4%) complaint about progestogen-only injectable contraceptive, of which amenorrhea constituted 176(66.7%); other complaints were painful nipple (2, 0.5%), weight gain (5, 1.4%), and abnormal vaginal discharge (1, 0.3%). At the time of analysis of this data 83(22.4%) women had discontinued the contraceptive, and menstrual abnormality was the commonest reason for the discontinuation (68, 81.9%); other reasons for discontinuation of the POIC were: excessive weight gain (5, 6.0%), ready for another pregnancy (4, 4.8%), attainment of menopausal age (3, 3.6%), nipple pain (2, 2.4%), and inability to keep appointment (1, 1.2%). None of the women that came for follow up got pregnant while on the method. [Figure - 1] shows the survival analysis of the women using the POIC over a 12-month period. At 12-month period more than 20% of the women had discontinued the use of the injectable contraceptive. [Table - 2] shows the factors associated with the discontinuation of the contraceptive using survival analysis. Women with lower parity had significantly (P < 0.001) lower duration of use than those of higher parity. Similarly, women who had stillbirth as antecedent delivery significantly (P< 0.01) discontinued the method earlier than those who had live baby. Women who used the method to limit their families significantly (P < 0.01) stayed longer than those using the method for child spacing. Those who had no complaint significantly (P < 0.05) stayed longer on the method than those with complaints. There was no significant association between those breastfeeding and not breastfeeding. Discussion Progestogen-only injectable contraceptive is a widely used method of contraception among the women attending LAUTECH Teaching hospital family planning clinic, and it is the second commonly accepted method, only next to the IUCD. [9] The use prevalence of this widely accepted contraceptive method among our women was 22.1%; this figure is comparable to the 21.9% reported from Ilorin (north central Nigeria), [3] but higher than the 7.9% and 14.2% reported from Ibadan(southwestern Nigeria) [10] and Jos (north central Nigeria), [11] respectively. The use prevalence in this study is lower than the 71.8% and 50.7% reported from Aba (southeastern Nigeria) [12] and Zaria (north western Nigeria), [13] respectively. In general, there seems to be regional variation in the use prevalence of progestogen-only injectable contraceptive. While it is the second commonly used method in this study and at Lagos, [14] it is the most accepted method at Zaria, [13] Porthacourt, [4] and Aba, [12] but the third commonly used method at Ibadan [10] and Ilorin. [3] This regional variation may be as a result of cultural and religious beliefs, and individual client′s perception of the contraceptive method. Contraceptive use had been said to be determined by the individual′s perception of their religious′ standpoint. [14] This same reason may explain why intrauterine IUCD is the most used contraceptive method among the studied population. Providers′ bias may also be another reason why IUCD is the commonest method among our women. [10] Women in the present study preferred the 3-monthly DMPA injection to the 2- monthly NET-EN injection. This is consistent with previous reports from other parts of Nigeria. [3],[4] Preference for the 3-monthly injection may be due to the reduced frequency to the provider; frequent appointment may be perceived economic loss from transportation and man hours. The age range 22-55 years with a mean of 34.04±5.68 years of the women in the present study is not different from the age range of contraceptive users in general. [9],[12] The young adolescents (age: 19 years and below) did not make progestogen-only injectable their method of choice as they did for IUCD, [9] this may not be unconnected with its effect on the bone mineral density. [7] This study revealed that injectable contraceptive was being used by both nulliparous and multiparous women, and this is in agreement with a previous study which reported that the use of the method cut across all parities. [3] Terminal fertility control was the commonest reason for choosing the method. This may be attributable to the belief that DMPA persists in the body for several months in women who have used it for long-term contraception, and return to fertility may be delayed. [15] In a large study, however, 70% of former users desiring pregnancy conceived within 12 months, and 90% conceived within 24 months. [16] Menstrual abnormality was the commonest complaint of the women in this study, and it accounted for 71.4% of the complaints. The menstrual abnormalities experienced by the women were: intermenstrual bleeding, menorrhagia, hypomenorrhea, menstrual cycle irregularity, and amenorrhea, which is the commonest, accounting for 66.7%. Menstrual abnormality was the commonest reason for the discontinuation of this effective method of contraception by our women, and this was similar to previous studies reporting that menstrual abnormality is the commonest side effect and the reason for the discontinuation of progestogen-only injectable contraceptive. [3],[4],[15],[17] This study shows that there is good continuation rate of the contraceptive method, as more than 70% of the women were still on the method at 12 months. Women of low parity, those whose antecedent pregnancy was stillborn, and those who experienced side effects of the method discontinued the method earlier, while those without complication and those using the method for terminal fertility control stayed longer on the method. There was no report of accidental pregnancy while on the method among the women that came for follow up, and this supports the previous reports of its effectiveness with pregnancy rate close to zero. [3],[4],[8] In conclusion, short duration of POIC use that is within 12 months is still high. However the main reason for discontinuation was found to be due to menstrual irregularities, hence the need for effective education of the women about this side effect, thus increasing the acceptance and continuation rate of the contraceptive method. References
Copyright 2012 - Annals of African Medicine The following images related to this document are available:Photo images[am12006t2.jpg] [am12006t1.jpg] [am12006f1.jpg] |
| |||||||||


![[Table - 1]](/showimage?am/photo/am12006t1.jpg){kind=link}
{kind=link}
{kind=link}