 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 11, No. 1, January-March, 2012, pp. 36-41 Original Article Injection safety practices among nursing staff of mission hospitals in Benin City, Nigeria Vincent E Omorogbe, Vivian O Omuemu, Alphonsus R Isara Department of Community Health, University of Benin Teaching Hospital, Benin City, Edo State, Nigeria Code Number: am12008 PMID: 22199046 Abstract
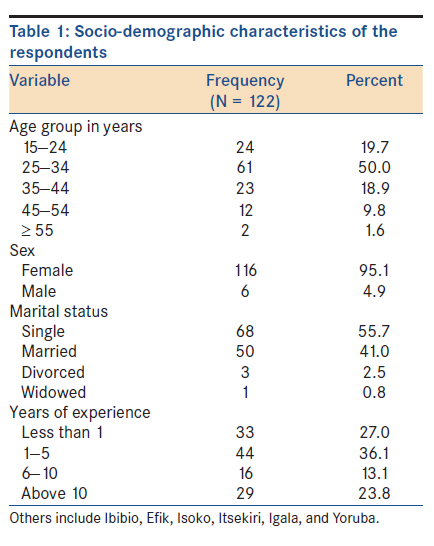
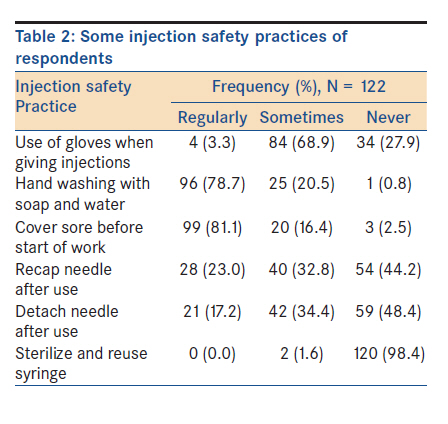
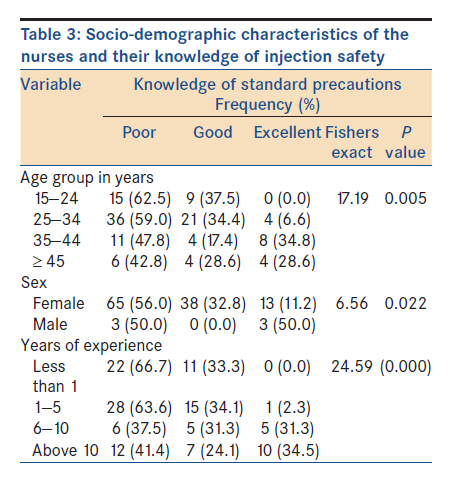
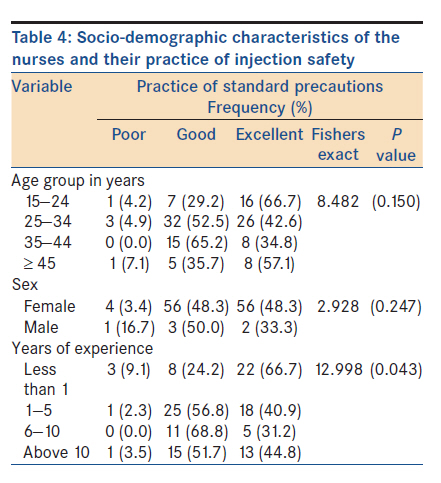
Background/Objective of the study: Injection safety has over the years become important in view of the many diseases that are transmitted through unsafe injection practice. The objective was to assess the knowledge and practice of injection safety by nurses in mission hospitals in Benin City, Nigeria. Keywords: Injection safety, mission hospitals, nurses Introduction Injection safety which is an integral component of infection prevention and control has over the years become important in view of the many diseases that are transmitted through unsafe injection practice. The WHO defined a safe injection as one that is given using appropriate equipment and does not harm the recipient, does not expose the provider to any avoidable risks and does not result in waste that is dangerous for other people. [1],[2] WHO estimates that annually 16 billion injections are given in developing and transitional countries, with an annual mean of 1.5 injections per person per year. [2] However, institutionalized children, persons who are ill or hospitalized, including those infected with HIV, are often exposed to 10-100 times as many injections. [3] About 90-95% of injections are therapeutic while 5-10% is given for immunization. [4] It has been shown that between 70% and 99% of these injections are unnecessary, while at least 50% are unsafe in 14 of 19 countries in five developing world regions with data. [3],[4],[5],[6] Injuries from sharp devices have been associated with the transmission of more than 40 pathogens, including hepatitis B virus (HBV), hepatitis C virus (HCV), human immunodeficiency virus (HIV), hemorrhagic fevers, malaria, and tetanus, thereby increasing the risk and burden of infectious diseases. [1],[7],[8],[9] The burden of unsafe injection practices is borne by the injection providers (health care workers), the patients, and the community at large. Injection providers are exposed to hazards of needle stick injuries from inadequate supply of appropriate sharp containers, unsafe practices such as recapping of needles, manipulating used sharps (bending, braking, or cutting hypodermic needles), passing of sharps from one health care worker to another, sharps carelessly left in unexpected places like dirty linen. Patients are exposed to the hazards of unsafe injection practices from excessive use of injectable medications especially when there are other suitable alternatives, reuse of injection equipment, self medication, sharps carelessly left in unexpected places like linen, when aseptic technique is not observed by healthcare workers and administration of drug at incorrect anatomical sites. The community is exposed to hazards of unsafe injections by unsafe waste disposal practices such as improperly placed disposal sites, improper disposal methods like the use of shallow pits, open dumping, unsecured pits, and easy access of the disposal site. Unsafe injections also carry socio-economic and psychological consequences on the individual and the health system of a country. Each year, the annual global burden of indirect medical cost due to HBV, HCV, and HIV/AIDS is estimated to be US$535 million. [10] Globally in the year 2000, unsafe injection was responsible for an estimated 21 million cases of HBV infection, 2 million cases of HCV infection, and 260,000 cases of HIV infection, making up 32%, 40%, and 5% of infections due to unsafe injection practices respectively. [11] It is estimated that 9.18 million disability life adjusted years (DALYs) would be lost between the years 2000 and 2030. However, interventions implemented in the year 2000 for the safe and appropriate use of injections could reduce the burden of injection associated infections by as much as 96.5% (8.86 million DALYs) for an average annual costs of 905 million dollars. [1],[11],[12] The WHO estimates that 501,000 deaths have occurred because of unsafe injection practices. [11] These deaths could have been prevented by injection safety practices which includes reduction of injections, ensuring safe injection practices using the "nine rights," availability of appropriate injection devices and proper disposal of sharps and other healthcare wastes. The "nine rights" of injection safety ensures that the right patient is given the right drug in the right dosage and right formulation using the right injection equipment at the right time and right route with right storage and the right method of disposal. [1],[7] Proper disposal of sharp will not only protect the healthcare worker from accidental injuries, but will also protect the community. This is even more so bearing in mind the practice of scavenging that is very prevalent in our communities. Mission hospitals play an integral role in healthcare provisions for the people. In such settings, the nurses are exposed to a lot of sharps as they are primarily responsible for the administration of parenteral medications including some intravenous drugs as well as minor surgical procedures like wound suturing and episiotomies. This study was therefore set out to assess the injection safety practices of the nurses in these hospitals to provide background data on their knowledge and practice of injection safety as well as provide a basis for planning necessary interventions that will help to promote and strengthen injection safety practices in the hospitals and hosting communities. Materials and Methods This descriptive, cross-sectional study was carried out in all the six mission hospitals in Benin City, the capital of Edo State, Nigeria. The mission hospitals complement the tertiary and secondary health facilities in rendering healthcare services to the people of Edo State. The study population comprised all the nurses employed in these hospitals who engaged in administration of parenteral medications. The minimum sample size required for the study calculated using the simplified formula [13] for sample size determination for an infinite population in a descriptive study was 114. Out of the 139 nurses working in these hospitals, 122 agreed to participate in the study giving a response rate of 88%. Permission to conduct this study was obtained from the medical directors of the respective hospitals while individual informed consent was sought from the respondents with full assurance of confidentiality. Only the respondents who gave their consent participated in the study. A structured interviewer-administered questionnaire adapted from the WHO injection safety assessment tool [6] was used to collect both quantitative and qualitative information such as socio-demographic data of the nurses and their knowledge and practice of injection safety. At the end of the interview, the respondents were educated on safe injection practices. An observational checklist was used to assess the safety of the hospital and their waste management particularly with regard to used sharps. Completed questionnaires were screened by the researcher for completeness after which they were coded and entered into the computer. SPSS version 13 computer software was used for analysis of data obtained from respondents. Four questions were used to assess the respondent′s knowledge while six questions were used to assess their practice of injection safety. The questions were graded as correct or incorrect and points were allocated to each correct answer. For knowledge of injection safety, each correct answer was scored 2 points while an incorrect answer was scored zero giving a maximum point that a respondent can obtain to be 8, while for practice of injection safety, respondents who practice it all the time were scored 2 points, those who practice it sometimes were scored 1 point while those who do not practice it or those who practice it wrongly were scored zero. Thus the maximum point for practice was 12. The maximum points obtained by a respondent were converted to percentages and used to categorize them as follows: poor knowledge = 0-49%, good knowledge = 50-69%, excellent knowledge = 70% and above, poor practice = 0-49%, good practice = 50-69%, and excellent practice = 70% and above. The chi-square statistical test and Fishers exact test were carried out where applicable and the level of significance was set at a P value of less than 0.05. Results A total of 122 nurses in the mission hospitals were interviewed and their socio-demographic characteristics are shown in [Table - 1]. The mean age of the respondents was 32.0 ± 8.9 years with half of them (50.0%) in the age group 25-34 years. Only 2 (1.6%) were aged 55 years and above. Most 116 (95.1%) of the respondents were females while the males constituted the remaining 4.9%. A higher proportion 44 (36.1%) of the nurses have been practicing nursing for 1-5 years, 33 (27.0%) for less than 1 year, 18 (14.8%) for more than 15 years, 16 (13.1%) for between 6 and 10 years while 11 (9.0%) have been practicing nursing for 11-15 years. The mean duration of practice was 2.5 ± 1.4 years. Sixty-eight (55.7%) respondents had poor knowledge of injection safety, 38 (31.1%) had good knowledge while only 16 (13.1%) had excellent knowledge of injection safety. Up to 59 (48.4%) respondents had good practice of injection safety while 58 (47.5%) of them had excellent practice. Only 5 (4.1%) practiced injection safety poorly. The respondent′s knowledge of the specific hazards and infections associated with unsafe injection practices showed HIV/AIDS 81 (86.2%), HBV 52 (55.3%), HCV 36 (38.3%), and tetanus infection 15 (16.0%). Other hazards mentioned were paralysis 43 (45.7%), drug reaction 40 (42.6%), abscesses 35 (37.2%), needle prick 21 (22.3%), and drug overdose 3 (3.2%). Some specific injection safety practices of the respondents are shown in [Table - 2]. Majority 84 (68.9%) of the respondents use disposable gloves sometimes when administering injections to patients while only 4 (3.3%) use gloves regularly. Majority (96 [78.7%]) of them wash their hands with soap and water after attending to a patient while 25 (20.5%) do not. Similarly, 99 (81.1%) cover any sore or injury they have before starting work while 20 (16.4%) do so sometimes and 3 (2.5%) do not cover their injuries before starting work. Only 54 (44.2%) of the respondents revealed that they never recap needles after use while 28 (23.0%) and 40 (32.8%) respondents revealed that they recap used needles regularly and sometimes respectively. A cross-tabulation of the socio-demographic characteristics of the respondents and their knowledge and practice of injection safety [Table - 3] and [Table - 4] revealed that there was a statistically significant association between the age (P = 0.005), sex (P = 0.022) and years of experience (P = 0.000) of the respondents and their knowledge of injection safety. The knowledge increased with increasing age and years of experience when those with poor knowledge were compared with a combination of those with good and excellent practice. More females had a better knowledge than their male counterparts. The association between the age (P = 0.150) and sex (P = 0.247) of the respondents and their practice of injection safety was not statistically significant; however, the association between years of experience and practice of injection safety was statistically significant (P = 0.043). Majority (71 [58.2%]) of the respondents had reported needle stick injuries compared with 43 (35.2%) who have not. Eight (6.6%) respondents could not remember having sustained any needle stick injury in the past. Among respondents who reported needle stick injuries, 17 (13.9%) did so in the last 6 months, 24 (19.7%) between 6 and 12 months, while 30 (24.6%) sustained needle stick injuries over 12 months preceding the study. Following needle stick injuries, 7 (9.9%) respondents wash the site with water only, 11 (15.5%) washed with soap and water only, 15 (21.1%) washed with water/soap and applied methylated spirit, 22 (31.0%) applied liquid bleach to the site, 12 (16.9%) applied both methylated spirit and liquid bleach. while only 4 (0.6%) respondents had postexposure prophylaxis. Discussion The mean age of the respondents was 32.0 ± 8.9 years with majority of them in the age group 25-34 years. This is expected considering the mean duration of training as a nurse and the fact that older nurses would probably be working in a government-owned health facility with better remuneration. This finding was similar to that from a study of health workers in static immunization centers in Ilorin, [14] which found the mean age to be 33 ± 6.0 years, but different from another study in Morocco [15] which reported a mean age of 41.4±7.0 years. Female constituted overwhelming majority of respondents because nursing has remained predominantly a female dominated profession with very limited male involvement. A similar finding was obtained in both the Ilorin [14] and Moroccan [15] studies. The short mean duration of practice seen in this study could be the result of the drive for better remuneration and job security in most nurses working in nongovernment owned health facilities who do not hesitate to leave when they have better job offers especially in government hospitals. This invariably means that there may be some gap in experience due to the highly mobile work force in the health facilities. The knowledge of injection safety was found to be poor in this study. However, the specific knowledge of infections that could result from unsafe injection practices especially HIV and HBV infections was high. This is consistent with another study in Ilorin, Nigeria in which 58.3% had knowledge of diseases transmissible by needle stick injury. [16] The high level of awareness about the mode of transmission of HIV infection and the ingrained fear of the disease in the society may be responsible for this. Similar studies in Cambodia and China also found that most prescribers and injection providers were aware that HIV, HBV, and HCV were transmitted through unsafe injection practices. [17],[18] It is not surprising that the knowledge of injection safety was significantly associated with the age, sex, and years of experience of the respondents. The older nurses having better knowledge of injection safety may be attributed to the fact they are more likely to have attended workshop and training seminars compared to the younger. The respondents had a better degree of practice of injection safety with 59 (48.4%) and 58 (47.5%) of them having good and excellent practice of injection safety respectively. Although a better knowledge is a major contributor to the practice of injection safety, it is likely that the incurable nature of HIV/AIDS and its attendant stigma may force health workers to be more careful when handling sharps without necessarily having detail knowledge of the definition of injection safety which formed the basis for determining the knowledge of injection safety. This may also explain the fact that there was no statistically significant association between the socio-demographic characteristics of the nurses and their practice of injection safety. The practice of regular hand washing with water and soap by majority (78.7%) of the nurses was quite encouraging. However, it is worrisome to note that only 4.0% of them use hand gloves regularly when administering injections. This finding is consistent with the Ilorin study where none of the respondents were observed wearing gloves during immunization sessions, but was different from the study in Morocco which reported that 34.5% of the respondents wear single use gloves during service provision. [15] The availability of hospital consumables such as disposable gloves may limit the use of such by the respondents especially in developing countries like Nigeria. It is alarming that 23.0% of the respondents still recap needles all the time after use while 32.8% do so sometimes. A similar situation was observed in other studies in Nigeria [14],[19],[20] and in southern Africa. [21] This practice of recapping and detaching of needles by some of the respondents increase the risk of needle stick injuries among the nurses. It is therefore not surprising that more than half (58.2%) of the nurses in this study had sustained needle stick injuries. Also worrisome is the fact that following a needle stick injury, only 4 (5.6%) of the respondents had postexposure prophylaxis while majority of them only washed the site with soap and water and applied either liquid bleach or methylated spirit. Thus there was a high risk of blood borne infections among the nurses in this study. This study revealed that the knowledge of injection safety was poor among the nurses in mission hospitals in Benin City but their practice of injection safety was quite encouraging. It is therefore recommended that regular training workshops on injection safety should be organized by the mission hospital to improve the knowledge of injection safety among their nurses. Also, the hospitals should develop facility protocol on postexposure prophylaxis for their employees in line with the national policy on injection safety and the workers educated on the action to take following accidental needle stick injury. This will greatly minimize the risks to healthcare workers developing blood borne infections and other hazards associated with needle stick injuries. References
Copyright 2012 - Annals of African Medicine The following images related to this document are available:Photo images[am12008t3.jpg] [am12008t1.jpg] [am12008t4.jpg] [am12008t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}