 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 11, No. 1, January-March, 2012, pp. 42-45 Original Article An audit of basic practical skills acquisition of final year medical students in a Nigerian medical school NJ Jebbin, JM Adotey Department of Surgery, University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria Code Number: am12009 PMID: 22199047 Abstract
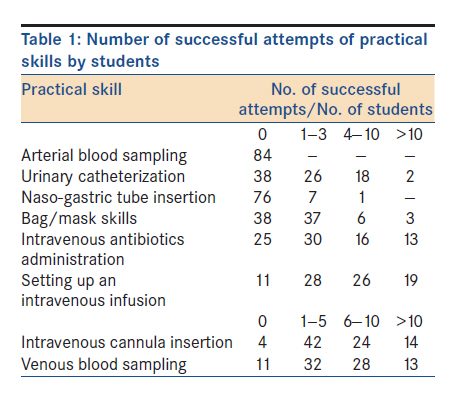
Background/Objective: Young medical graduates undertaking their housemanship are naturally expected to demonstrate reasonable competence in basic practical skills. Failure to do this may not only be a source of anxiety to the doctor but also potentially dangerous to the patient. The objective was to assess the level of exposure of final year medical students of a Nigerian medical school to basic practical skills. Keywords: Acquisition, basic practical skills, medical students Introduction Skillful performance of practical skills (such as phlebotomy, intravenous cannula insertion, and arterial blood gas sampling) by physicians is fundamental to the delivery of quality service to patients. Final year medical students often express some anxiety with regard to their competence in some basic practical skills as they look forward to their preregistration house job. [1] Surveys carried out in developed countries revealed obvious deficiencies in the teaching and acquisition of basic skills in the medical curriculum. In the UK over a decade ago, Calman and Donaldson [2] expressed concern about the lack of basic clinical skills in newly qualified medical graduates. A survey of interns on their experience in surgical procedures as students suggested that many interns had not performed some basic procedures by the time they entered residency training. [3] Another report by Goodfellow and Clayton [1] noted that training in skills could be improved. A similar concern has been expressed by Nelson and Traub in the United States. [4] These findings have led to a change of medical curriculum in some countries with a view to correcting these deficiencies. [5] There is no doubt that conscientious medical students can acquire a lot of skills from preregistration house officers. As Nganginieme and Ihekwaba [6] noted, this will not be possible if students are absent when house officers carry out patient care on their own at the bed side or if house officers do not perform enough patient care. Schwartz et al. [7] in the United States had asserted that coincident with emphasis on research and publication, and expanded resident patient care duties, teaching, particularly, medical student teaching had assumed a very low priority. We sought to assess the extent to which a set of final year students of the University of Port Harcourt medical school had been exposed to the skills required for the preregistration year and compare the findings with those of the developed world. Materials and Methods A structured questionnaire was self-administered to final year medical students of the University of Port Harcourt medical school, Nigeria, during their final posting in medicine and surgery. This was done immediately after their last didactic lecture in the posting and after obtaining formal informed consent and ethical approval from the hospital′s Ethical Committee. Students were told before distribution of the questionnaire that the study had nothing to do with their forthcoming Final professional examination and that the responses were to be anonymous. The questionnaire asked the students to indicate approximately the number of times they had successfully performed the following practical skills:
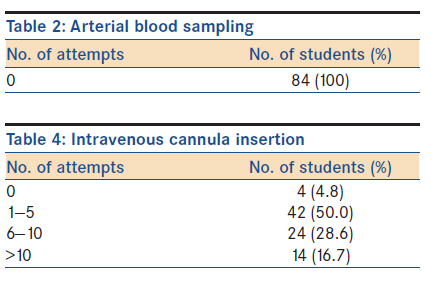
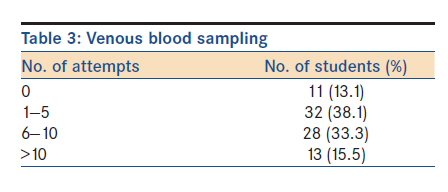
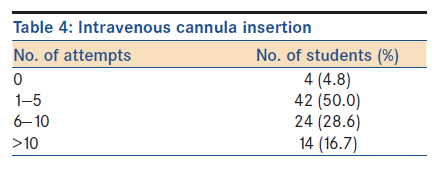
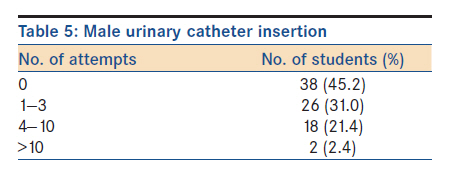
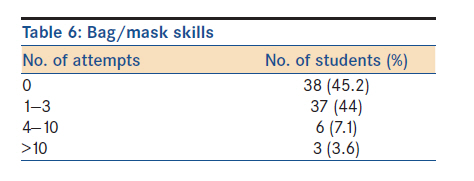
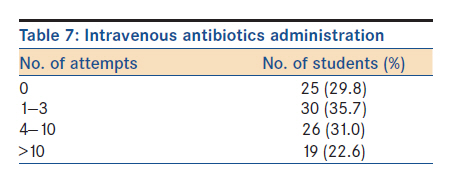
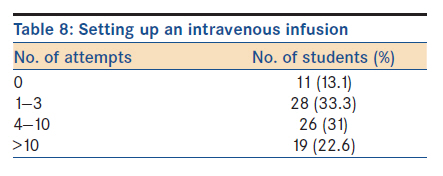
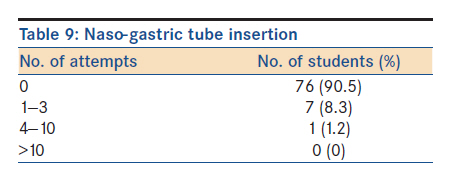
They were asked to fill the questionnaire and return the same before leaving the lecture hall. The responses were collated and analyzed using simple descriptive statistics. Results Of 86 students in the class, 84 completed the questionnaire, giving a 97.7% response rate. No student had ever performed arterial puncture for blood samples. The results are presented in [Table - 1], [Table - 2], [Table - 3], [Table - 4], [Table - 5], [Table - 6], [Table - 7], [Table - 8] and [Table - 9]. Forty-one (48.7%) students had 6 or more successful attempts at venous blood sampling (phlebotomy) while only 24 (28.6%) had successfully inserted more than 10 intravenous canulae. A significant number, 38 (45.2%) had never inserted a urinary catheter nor had any experience with bag/mask skills. Majority of the students (70.2% and 86.9%) had had varying experiences with intravenous antibiotics administration and setting up intravenous fluid infusion, respectively, while 76 (90.5%) had never inserted a naso-gastric tube. Only 4 (4.8%) students had never had any attempt with intravenous canulation. Discussion The very high response rate may have been a reflection of the simplicity of the questionnaire format, the condition of anonymity and the usual increased enthusiasm towards assignments among students close to examination periods. The explanation that the findings from the study would have no part to play in their forthcoming examination might also have contributed to the high response rate. As reported in a UK study, [1] at completion of training in the University of Port Harcourt medical school, a sizeable number of students were not familiar with many tasks that would become part of their day to day activities as preregistration house officers. Medical school training is expected to lay the foundation for a life-long career in medicine and to equip potential doctors for the first stage in their working lives. [8] In a survey of basic practical skills in another UK medical school, [9] it was found that not all skills had been mastered to the same degree as venous blood sampling and intravenous canula insertion. This is similar to the findings in this study. Naso-gastric tube insertion has been regarded as a nursing procedure. [9] In our centre, however, this is in practice not the case as nurses often shy away from it. Apart from arterial puncture, this is one basic skill that majority of respondents in this study had poor exposure to. In a survey by Jolly and MacDonald, [10] only 24% of respondents had undertaken placement of two or more naso-gastric tubes, whereas 96% had sited two or more intravenous canulae. Board and Mercer [9] reported a similar finding in their study and suggested that the first thing the student should do was to watch the nurse have one more attempt so that one who had never seen it done would have some idea of where to start. The total inexperience of all respondents in arterial puncture is a matter for real concern. Apart from venous blood sampling and intravenous canula insertion, this was one skill that a good percentage of students in one UK study [9] were very proficient in. Arterial punctures are mainly for blood gas analysis and blood culture studies. These services are currently unavailable in the UPTH. In one study [8] where house officers were asked to comment on how well the medical school had prepared them for the job, only 4.3% strongly agreed that their training had prepared them well. Specific comments included "medical school provided excellent factual preparation for pre-registration house officer jobs but was limited in basic problems found on the wards," "not enough emphasis on real life situations," "felt inadequately prepared for surgical house jobs." We did not include this aspect in our study but the experience would probably have been the same. To improve on these experiences, Goldacre et al. [8] suggested that log books and skills laboratories for undergraduates, and induction courses for house officers could help. These suggestions are useful. Skills laboratories provide an environment for structured learning and feedback. [11] Though they do not offer "real patient" experience, they are useful. [11] In recent times, there has been extensive use of mannequins for simulation to enhance skills acquisition among students, resident doctors, and even doctors. This is a very plausible tool, especially in a resource-poor country such as Nigeria. The work-based skills course in surgery described by McMahon et al. [12] has strong merit as a possible remedy for students′ ill-preparedness for surgical house jobs. A curriculum review to include the posting of final year students to rural hospitals with close supervision by senior colleagues may also help. In a study in Australia by Culhane et al., [13] over 50% of students were competent in 57 procedures after a 4-month rural attachment compared with 37 procedures before it. There were 26 procedures in which more than 20% of students increased their competence. Some authors in developed countries have cited the increasing level of medico legal cases as contributing to the deficiency of skills among final year students. [9] Nigerian patients are beginning to be increasingly litigation conscious (personal communication) and it is believed that the scenario abroad may soon replicate itself in our environment. It is in this regard that the suggestion by Board and Mercer [9] to teach some of these skills while the patient is under anesthesia may be worth some attention. The anxiety and discomfort associated with the procedures are thus eliminated. In conclusion, the exposure of students to basic practical skills in the University of Port Harcourt medical school is deficient. We recommend a curriculum review that will emphasize the acquisition of these skills early in their training. References
Copyright 2012 - Annals of African Medicine The following images related to this document are available:Photo images[am12009t5.jpg] [am12009t4.jpg] [am12009t1.jpg] [am12009t7.jpg] [am12009t3.jpg] [am12009t2.jpg] [am12009t9.jpg] [am12009t6.jpg] [am12009t8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}