 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 11, No. 1, January-March, 2012, pp. 52-57 Short Report Functional outcome of diaphyseal fractures of femur managed by closed intramedullary interlocking nailing in adults MK Deepak, Karun Jain, Kumardev A Rajamanya, Pratik R Gandhi, CS Rupakumar, R Ravishankar Department of Orthopaedics, JSSMC, Mysore - 570 004, India Code Number: am12013 PMID: 22199051 Abstract
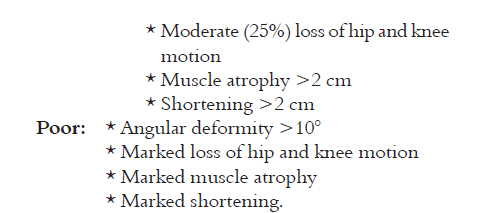
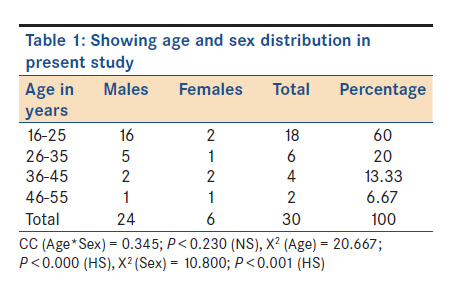
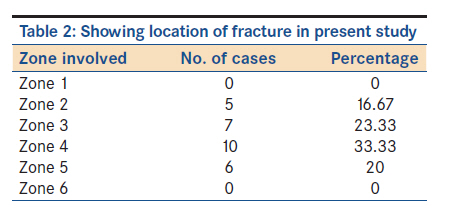
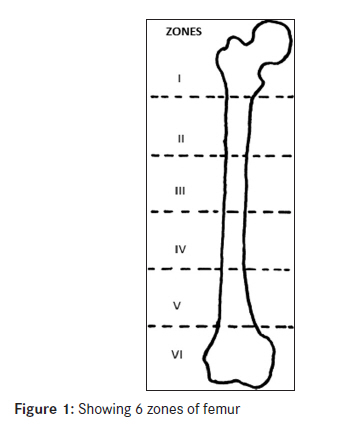
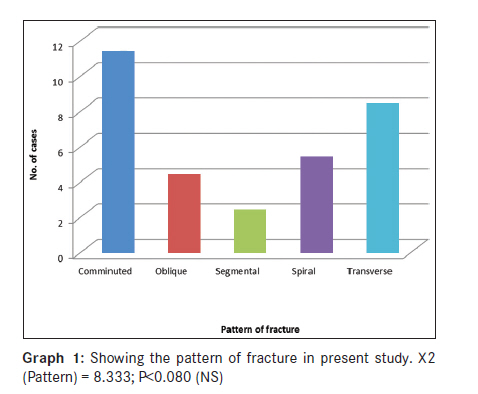
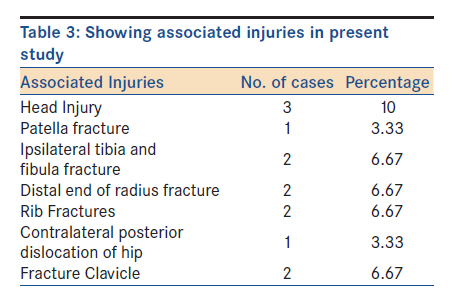
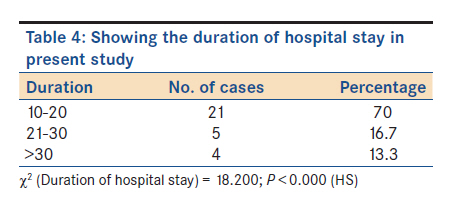
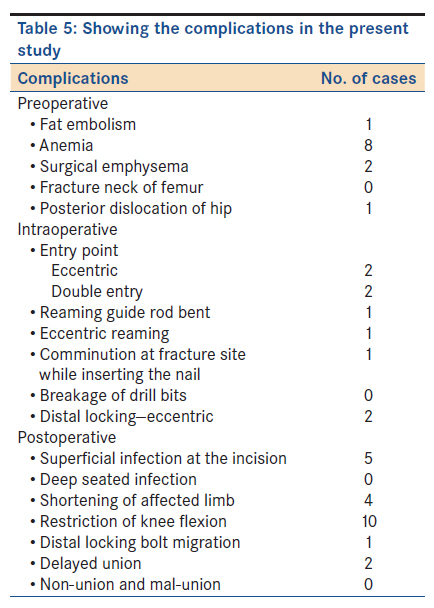
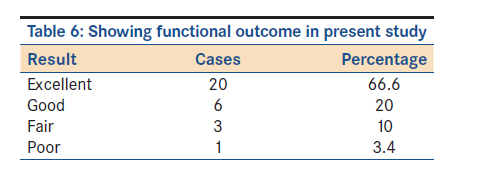
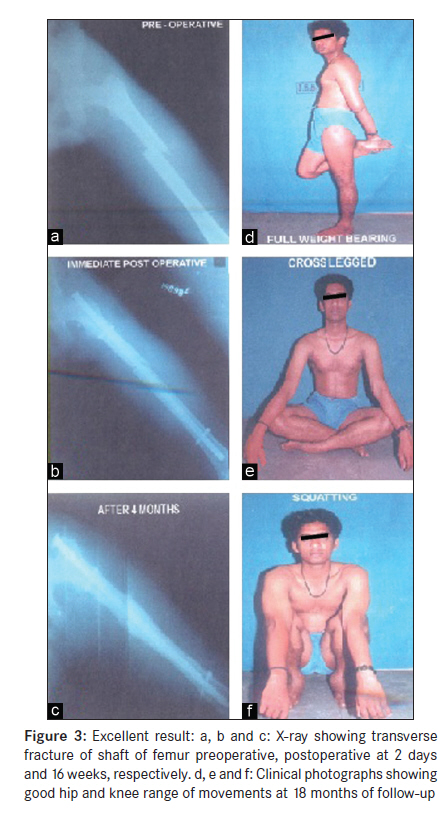
Objective: To study the effectiveness, advantages, disadvantages and failure rates of closed intramedullary interlocking nailing of daiphyseal fractures of the femur in adults. Keywords: Closed interlocking nailing, diaphyseal fractures of femur, modified Klaus and Klemm criteria Introduction Fractures of femoral shaft are among the most common fractures that orthopedic surgeons encounter. Advances in mechanization and acceleration of travel have been accompanied by an increase in the number and severity of fractures. Since the femur is the largest bone of the body and one of the principal load-bearing bones in the lower extremity, femoral shaft fractures are associated with considerable mortality and morbidity whether they are caused by high- or low-energy trauma. Femoral shaft fractures resulting from high-energy trauma are often associated with concomitant injury of internal organs. [1] The treatment of femoral shaft fractures has evolved from the historical nonoperative management to the most recent methods of intramedullary nail fixation. Interlocking nails have greatly expanded the indications for closed intramedullary nailing of femoral fractures. Early mobilization following fractures of the femoral shaft has been shown to have a significant advantage in terms of both joint mobility and economic impact, which are very well attained by the use of interlocking nails. [1],[2],[3],[4] Materials and Methods A prospective case series study of 30 cases of closed and Gustilo Anderson type I [1] open diaphyseal fractures of femur was done during the period between 2008 and 2010. Patients of age above 18 years and both the sexes were included in the study. Pathological and Gustilo Anderson type II and III open fractures [1] were excluded from the study. Institutional ethical committee approval was taken. After a careful history and examination of the injured limb, anteroposterior and lateral radiographs were obtained. Closed reduction and Thomas′s splint immobilization were done in all cases. The operative procedure and its advantages were explained in detail to each patient and an informed consent was obtained. All patients were operated as early as possible after improving the general condition and considering their medical comorbidities and management as directed by physicians. Most of the femoral shaft fractures in our study resulted from high-velocity injuries. Associated injuries were also extremely common and played an important role in the initial treatment of fracture and rehabilitation of the patient. Special attention was given to the complications followed by trauma and were managed accordingly. All patients were operated using standard operative guidelines [1],[2],[4] and all fractures were fixed with standard AO femoral intramedullary interlocking nail using closed technique [1],[2],[5] under image intensifier. All patients were encouraged to do static quadriceps exercises and straight leg lifting from first postoperative day with active and passive knee exercises within 48 hours or as tolerated by the patient. Partial weight bearing was started for all cases with the help of crutches or walker frame by the time of suture removal or once the acute pain subsided. Full weight bearing was started within 2 weeks postoperatively in case of stable fractures, but in unstable fractures (comminution >50%), it was delayed till radiographically visible callus was seen or around 6 weeks′ time. Sutures were removed on 10 th postoperative day and the patient was discharged on the following day. Follow up Review of the patient was done for every 2 weeks for first 2 months, and thereby monthly for next 4 months to document clinical and radiological union of fracture and to assess the hip and knee range of movements. Partial weight bearing was started once the acute pain has subsided in stable fractures, but was delayed until adequate callus is seen radiographically at the end of 6 weeks and full weight bearing by the end of 4 months. We considered a fracture to be united, if there was no pain on palpation or attempted motion at fracture site, no increase in warmth at the fracture site, no discomfort on full weight bearing and serial radiograph demonstrates bony trabeculae across the fracture site. Results of the treatment were evaluated using modified Klaus and Klemm criteria. [6] [Criteria A and Criteria B] Statistical analysis The frequencies and crosstabs procedure were used to create two-way and multiway tables. Statistics and graphical displays (values in ascending or descending order) were used for describing variables, chart, and graphs. After tabulation, P value was determined by applying standard Chi-square and Gaussian test. P value less than 0.05 was considered to be significant. All the statistical methods were carried out through the SPSS for Windows (version 16.0) and Minitab (version 11.0) for windows. Results A total of 30 cases of diaphyseal fracture femur were seen in the study. Most common age group involved was between 18 and 25 years, with mean age of 27.4 years. Males significantly had a higher frequency (24) compared with females (6) [Table - 1]. Right side (60%) was affected more commonly than left side (40%). RTA (83.34%) was the most common mode of injury followed by fall from height (13.33%). Most common location of fracture was the middle third of the diaphysis [Table - 2], [Figure - 1]. Most common pattern of fracture was comminuted and transverse fractures [Graph 1]. 56.67% of patients had only femur fracture and the remaining (43.33%) had associated injuries, which were treated accordingly [Table - 3]. Twenty-two patients (73.3%) came to the hospital within 24 hours after injury, while six patients (20.0%) came in between 24 and 48 hours, and two patients (6.7%) after 48 hours. The surgery was done on an average of 6 days (range, 2-15 days) after patient′s admission. Spinal anesthesia was used in 27 patients and general anesthesia in three patients. Average duration of surgery was 120 minutes (range, 90-150 minutes). Duration of hospital stay ranged from 11 to 33 days [Table - 4]. Average duration of follow up was 2 years, with a range of 12 to 30 months. Delayed union was seen in two cases (6.6%), but one case united at the end of 7 months without any further surgical intervention, and the remaining one case needed dynamization. The shortening of the limb was seen in four cases (13.33%), of which two had 2 cm shortening and other two cases had 1 to 1.5 cm shortening. Five patients had superficial infection at incision site and there was one case of refracture with broken nail in situ, where exchange nailing was done [Table - 5]. Mean time of bony union was 16.5 weeks and the union rate in our series was 96.6%. Functional outcome was assessed based on modified Klaus and Klemm criteria. [4],[6],[7] Excellent results were obtained in 20 cases (66.6%), good results in six cases (20%), fair in three cases (10%), and poor in one case (3.4%) [Table - 6] [Figure - 2], [Figure - 3], [Figure - 4] and [Figure - 5]. Discussion The art and science of fracture management has tremendously advanced over the years. From the use of external splints in the Hippocratic age to the recent sophisticated instrumentation, treatment of fractures has made an impact in the surgical field. The intramedullary techniques that are in common use today are derived mainly from the work of Sir Gerhard Kuntscher [7] in Germany and the Rush family in USA. Kuntscher is no doubt the father of reamed intramedullary nailing. Intramedullary nailing has become the gold standard for the treatment of femoral shaft fractures. [1],[7],[8],[9],[10] At the beginning of intramedullary nail era, this type of fixation gained wide popularity in the fixation of transverse fractures of the middle third of the femur due to no disturbances of periosteal blood supply, fracture hematoma, and rapid healing of fracture with lesser risk of complications like infection, nonunion, and shortening. A shortcoming of this technique in the fixation of comminuted diaphyseal fractures was the failure to provide rotational stability and axial length. The advent of interlocking nailing has widened the spectrum of femoral shaft injuries that can be stabilized by intramedullary technique. Use of interlocking nailing minimizes the incidence of leg length discrepancies, rotational and angular deformities. The intramedullary nail, with its location close to center of femur, can tolerate bending and torsional loads better than plates and the locking mechanism provides less tensile and shear stress than plates. The intramedullary interlocking nail is a load-sharing device. It is less loaded than plates causing less cortical osteopenia of stress shielding, which is a feature of the load-bearing plates. Closed nailing technique is preferred because no damage to extraperiosteal soft tissue occurs and the biological environment around the fracture is minimally disturbed. Another important feature of the closed intramedullary interlocking nail is the chance of early ambulation of the patient which reduces the complications of prolonged bed confinement. [1],[2],[10],[11] The mean patient′s age (27.4 years), mode of injury (road traffic accident, 83.34%), side involved (right > left), level of fracture shaft of femur (middle third, 56.66%), average duration of surgery (120 minutes), [12] postoperative complications like infections, incidence of delayed union (6.6%), and shortening (13.33% cases) are each comparable with literature reports. [1],[2],[3],[11],[13],[14],[15] Our study had M : F ratio of 4: 1. In authors′ opinion, administration of antibiotic for a period of 10 days (5 days intravenous followed by 5 days orally) drastically reduces the incidence of deep-seated infections. The average diameter of nail used in our study was 10 mm, which was less comparable with other series. [13],[16],[17] The skeletal framework of Indian population is on the lower side compared with the western population. In authors′ opinion, this is probably the reason of using a smaller diameter nail in the study. The percentage of associated injuries (43.33%) in our study was consistent with other series. [5],[12],[13],[18] Head injury cases were managed with neurosurgeons. Most of the associated fractures which required operative intervention were fixed during the same operative setting. The average time taken for bony union in our study was 16.5 weeks with union rate of 96.6%, which is comparable with other series. [3],[6],[8],[11] The high union rate in our study can be attributed to the preservation of fracture hematoma, using closed technique, early surgical intervention, early mobilization, and early weight bearing. The incidence of femoral fracture due to road traffic accident is on the increase. With our study, we recommend and re-establish the fact that closed intramedullary interlocking nailing is the current treatment of choice for closed diaphyseal fractures of femur in adults, especially those with significant comminution, long spiral fractures, and segmental fractures. Intramedullary nails have added advantages over plating in these cases, like restoration of anatomical length and alignment of comminuted fractures, biological fixation resulting in high union rates, less likely to fail in fatigue, strength for femoral shaft fracture in all three planes of loading-bending, compression, and torsion, early joint mobilization, early muscle rehabilitation, shortened hospital stay, reduces the incidence of complications like infection, cortical osteopenia, malunion, and nonunion, and most importantly early return to work and prefracture state. Moreover, the anatomy of femur and the loading conditions by gravitational, muscular, and ligamentous forces are in favor for intramedullary nail fixation. There is no significant change in union rate when compared with age, gender, level, and pattern of fracture. References
Copyright 2012 - Annals of African Medicine The following images related to this document are available:Photo images[am12013inlinea.jpg] [am12013f3.jpg] [am12013t6.jpg] [am12013inlineb.jpg] [am12013t5.jpg] [am12013t1.jpg] [am12013g1.jpg] [am12013t4.jpg] [am12013f4.jpg] [am12013f2.jpg] [am12013t2.jpg] [am12013f1.jpg] [am12013f5.jpg] [am12013t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}