 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Biotecnología Aplicada, Volume 17, July-September 2000, pp. 161-165 Epidermal Growth Factor-mediated Prevention of Renal Ischemia/Reperfusion Injury Manuel E Caballero,1 José L Calunga, 2 Ernesto Barber,3 Eduardo Cruz,4 Pedro López-Saura,1 Eduardo Boix,5 @ Jorge Berlanga1 1Center for Genetic Engineering and Biotechnology. PO Box 6162, Havana 10600, Cuba. E-mail: jorge.berlanga@cigb.edu.cu 2Center for Ozone Therapy. Havana, Cuba. 3Renal Physiology Laboratory. Havana School of Medicine. 4Biochemistry Department. Center for Biological Control. Food and Drug Faculty. University of Havana. 5Department of Pathology. Pediatric Hospital "Juan M. Márquez". Received in January, 2000. Accepted for publication in May, 2000. Code Number: BA00049 ABSTRACT The potential benefit of the epidermal growth factor (EGF) intervention in preventing renal damages due to ischemia/reperfusion, has not been examined so far. Female Wistar rats were randomly assigned (N = 10/group) to receive EGF at 500 or 750 µg/kg, or saline solution by a catheter via the femoral vein. An additional sham ischemized was included. Thirty minutes after treatment, bilateral renal ischemia was established for the same time, followed by 3 h of reperfusion. Post-reperfusion renal functionality was examined by determining the clearance of inulin and aminohippuric acid. The urinary volume for 10 min after reperfusion time was registered. Blood and kidney samples were collected for biochemical and histopathological studies. Intrarenal levels of malondialdehyde (MDA), as well as the activity of the enzymes phospholipase A2 (PLA2) and catalase were determined. EGF showed to significantly enhance diuresis (P < 0.05) in a dose-dependent manner. Accordingly, EGF significantly reduced renal tissue damages (P < 0.01). Renal functionality was preserved (P < 0.01) in the animals treated with the highest EGF dose. Intrarenal levels of MDA and the activity of the enzymes PLA2 and catalase were reduced. EGF exerts a prophylactic nephroprotective effect against the deleterious consequences of the ischemia/reperfusion episode. EGF contributed to preserve the morphological and functional integrity of the organ in a dose-dependent manner. Protection seems to be at least partially mediated by an anti-lipoperoxidative mechanism. Keywords: EGF, ischemia, kidney, reperfusion RESUMEN El factor de crecimiento epidérmico previene los daños renales asociados al episodio de isquemia/reperfusión. Aún no se ha estudiado el efecto potencial del recimiento epidérmico (FCE) en la prevención de los daños renales que se producen por isquemia/reperfusión (I/R). Se asignaron aleatoriamente ratas hembras Wistar (N = 10/grupo) al tratamiento con dosis de 500, 750 µg/kg de FCE o a solución salina. Se incluyeron ratas laparatomizadas y no sometidas a isquemia. A los 30 min después del tratamiento, se provocó isquemia renal bilateral durante el mismo tiempo, seguido de 3 h de reperfusión. El funcionamiento renal se determinó mediante el cálculo del nivel de aclaramiento de marcadores administrados. Se regristró el nivel de diuresis espontánea durante 10 min después de la reperfusión. Se obtuvieron muestras sanguíneas y renales para estudios bioquímicos e histopatológicos. Se determinó la concentración renal de malondialdehído (MDA), así como la actividad de las enzimas fosfolipasa A2 (FLA2) y catalasa. El tratamiento con FCE estimuló la diuresis (P < 0,05) y redujo (P < 0,01) los daños estructurales. El funcionamiento renal se mantuvo en los rangos fisiológicos en los animales tratados con la dosis superior. Los niveles intrarrenales de MDA y la actividad de las enzimas fueron menores en los grupos tratados con FCE (P < 0,01). Una administración profiláctica de FCE ofrece protección renal en el episodio de I/R de una forma dependiente de la dosis. Este efecto parece estar mediado, al menos parcialmente, por un mecanismo anti-lipoperoxidante. Palabras claves: FCE, isquemia, reperfusión, riñón Introduction Central organ systems including heart, gut, brain, and kidney are particularly sensitive to ischemia followed by reperfusion (I/R). Renal I/R injury alone imposes a significant burden on the healthcare system, as it not only restricts function and availability of donor kidneys for transplantation, but also a serious clinical complication of circulatory shock in sepsis, burns, etc [1]. Epidermal growth factor (EGF) is a well-known mitogen for a variety of epithelial and mesenchymally-derived cells [2]. EGF is also a potent cytoprotective and reparative polypeptide growth factor for the gastrointestinal mucosa [3] and other tissues when they are exposed to injurious factors or necrogenic agents [4]. The salutary effects of the systemic administration of exogenous EGF on different experimentally reproduced renal injury models, have been previously documented. Humes et al. [5] first demonstrated that EGF accelerates the regenerative process and the renal functional recovery following induction of ischemic renal injury in rats. An independent group subsequently confirmed that the EGF intervention accelerated functional recovery in rats affected by ischemic tubular necrosis [6]. Further experiments also showed that EGF therapy reduced mortality in rats with ischemic renal injury [7]. Other experimental models based on the nephrotoxic effect of some chemicals confirmed that exogenously administered EGF promoted a rapid relining of the injured renal tubular epithelium, and shortened the recovery time of renal excretory function [8, 9]. Acute renal injury causes a reduced expression of pre-proEGF mRNA, while the concentration of biologically active EGF rises seven to tenfold in the proximal tubules at the site of injury. This increase in local EGF availability is followed by a burst of tubular cells proliferation, and seems to be crucial for their regeneration [10, 11]. Exogenously-administered EGF provokes renal cell protection and, thus, may act as a survival factor when it is applied prior or during damage induction [12]. Subcutaneously injected EGF showed to reduce to 50% the number of apoptotic epithelial tubular cells in rats subjected to bilateral ureteral obstruction [13]. We have demonstrated that a single systemic administration of EGF significantly reduces glomerular tuft collapse, and tubular and interstitial damages, while enhances the creatinin clearance in a chemically-induced multiple organ failure model [14]. We next obtained similar findings in severely scalded rodents (Berlanga J., submitted). In both experimental scenarios, I/R is acknowledged as an important pathophysiological event for the onset of kidneys and other internal organs deterioration. The present experiment is, therefore, an attempt to definitively elucidate if a single EGF intervention confers renal protection in morphological and functional terms, when applied prior the induction of a controlled I/R episode. Materials and Methods Animals Female Wistar rats (200–220 g of weight) were obtained from the National Center for Laboratory Animal Production (CENPALAB, Havana, Cuba). The animals were allocated in a certified room with controlled environmental conditions at the animal facility of the Center for Genetic Engineering and Biotechnology (CIGB, Cuba). Rats were fed with standard commercial diet and water ad libitum. This experiment was conducted in compliance with the standard guidelines of the Animal Ethics Committee of the CIGB. EGF and treatment Commercially available human recombinant EGF was obtained from Heber Biotec SA, Havana, Cuba. The peptide was reconstituted in normal saline solution (IMEFA, Havana, Cuba), filter-sterilized (0.22 µm; Sartorius, Goettingen, Germany) and kept at 4 °C until use. Rats were randomly assigned to four groups (N = 10). Animals from groups I and II received EGF at 500 or 750 µg/kg, respectively. Animals from group III received normal saline solution. A fourth non-treated sham ischemized group of rats was included. These animals were laparotomized, catheterized, but their kidneys were not subjected to ischemia. EGF and the normal saline solutions (1 mL total volume) were slowly administered via a catheter inserted in the right femoral vein. Thirty minutes later, the ischemic episode was initiated. A thermal pad was used to maintain animals’ temperature. Renal ischemia/reperfusion Once the animals were anesthetized (sodium pentobarbital, Roig-Farma, Spain), surgically instrumented and treated, bilateral renal ischemia was provoked by clamping the renal pedicles with non-traumatic microclamps, placed at the same time for 30 min as previously described [15]. Afterwards, spontaneous reperfusion was allowed for a controlled period of 3 h. Renal functional assessment Renal functionality was examined by determining the renal plasma blood flow (RPF) and the glomerular filtration rate (GFR) by means of plasma clearance of p-amino-hippurate (PAH) and inulin (In), respectively, as described [16]. Briefly, plasma was saturated with PAH (Merck, Germany) and In (BDH Chemicals, England). The solution of both substances (2 mg PAH + 20 mg In/100 mL of normal saline) was continuously infused during the reperfusion time by a peristaltic pump through the left femoral vein at a constant rate of 150 µL/min, after an initial loading with 800 µL containing 12 mg/mL PAH and 2 mg/mL In. After 15–20 min of reperfusion, blood was collected by cardiac puncture, whereas at the same time urine was directly collected from the bladder. The concentration of the PAH and In markers was determined in cadmium sulphate-deproteinated plasma and urine, using for PAH the photocolorimetric technique described by Smith and Tinkelstein [17]. Inulin was measured by the direct method of resorcinol without alkaline treatment [18]. Plasmatic markers (PM) clearance (C) was calculated as described [16] and shown: C = Uv(m) x [PM]u / [PM]p where, Urinary excretion Diuresis was studied according to a previous description of the model [16]. The volume of excreted urine during 10 min after the reperfusion time was collected via a bladder catheter once the meatum was ligated. Total urine volume is expressed in µL/10 min. Biochemical determinations Kidneys were excised during autopsy, and rapidly divided lengthways, so that one half was immediately frozen at -20 °C until use for biochemical analysis, and the other was formalin-fixed for histopathology. Frozen kidneys were homogenized (Janke and Kunkel GmbH and Co, Staufen, Germany) at 4 °C in 50 mM KCl/histidine buffer pH 7.4, 1:10 (w/v), and centrifuged (Hitachi, Japan) at 8500 x g for 30 min. The supernatants were used to determine the renal tissue concentrations of malondialdehyde (MDA) as one of the end products of ischemia-derived oxidative stress. MDA was determined by the thiobarbituric acid method [19] and the results were expressed as nmol/mg of protein. The activity of the enzymes catalase and phospholipase A2 (PLA2) was determined as described by León et al. [20] and Hotter et al., respectively [21]. Enzymatic activities were expressed as U/g of protein. The Coomassie blue method was used for protein quantitation [22]. Renal histopathology The kidneys were fixed in 10% buffered formalin, paraffin embedded, 5-µm sectioned and stained with hematoxiline and eosine. The blind examination of specimens allowed the identification of the most frequent histopathological changes, so that their incidence (expressed as %) was determined in every group. The parameters studied involved glomerular, tubular and interstitial changes, and were categorized as: (I) number of collapsed glomeruli (quantified on each section at a constant magnification x10), (II) presence of cortical and medullary hemorrhagic foci, (III) severe tubular damage (manifested by cellular detachment, apoptotic-like images given by chromatin condensation at the periphery of the nucleus, karyorrhexis, karyolysis, cellular coagulation), and (IV) severe interstitial damage (characterized by a marked edema, tubular distortion, eosinophilic deposits, and inflammatory infiltrate). The histopathological parameters used in this work are in line with those reported by other authors for similar models or clinical situations of renal I/R [15, 23]. Statistical analyses Firstly, normality of data distribution was analyzed by the Kolmogorov-Smirnov test. Post-reperfusion diuresis was compared by the non-parametric Mann-Whitney U test because data were not normally distributed. One-way ANOVA followed by the Duncan’s multiple rank test, were used to compare the GFR and the RPF indexes, as well as the intrarenal biochemical parameters (MDA, PLA2 and catalase). The incidence of each histopathological parameter of damage was also compared by ANOVA and Duncan’s test. A significance value of P < 0.05 was established for all the tests. Results Post-reperfusion diuresis The ischemic episode significantly impaired diuresis (P < 0.05) in the control group receiving saline solution, as compared to values registered in sham ischemized animals (Table 1). EGF intervention influenced diuresis in a dose-dependent manner. Animals receiving the first dose level increased the diuresis in relation to the control group, although this difference was not statistically demonstrated (P = 0.056). Rats receiving the highest EGF dose, however, preserved their diuresis (P = 0.02), which was noted slightly enhanced (not significantly) in relation to the sham ischemic group. Table 1. Post-reperfusion diuretic output.
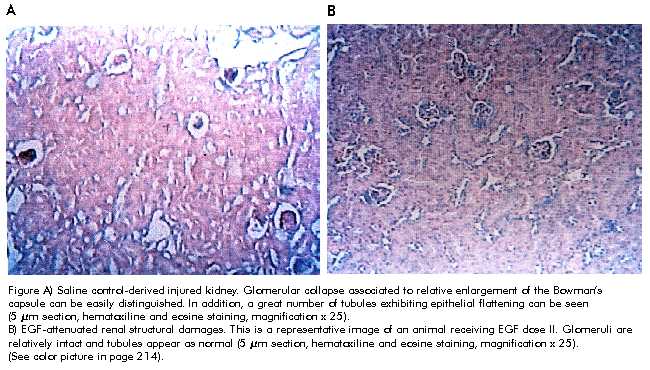
Mean values ± SD of urine volume per group (n = 10 rats). Diuresis was significantly reduced in ischemized control rats receiving saline solution as compared to sham ischemic animals, *P = 0.03. No difference was observed between control rats and EGF dose I, P = 0.056. EGF dose II stimulated diuresis in relation to control rats, **P = 0.02. Sham ischemic rats and EGF-treated groups were not statistically different (all P > 0.05). Mann-Whitney U test, P < 0.05 established significance value. Data are expressed in µL/10 min. Morphological renal changes The histopathological examination revealed clear differences among the groups, and they all involved the kidney’s structures. The main damage of the glomeruli consisted in tuft collapse (Figures A and B), accompanied by a relative enlargement of the Bowman’s capsule. Occasionally, the Bowman’s space appeared obliterated by an eosinophilic foamy material. Other glomeruli exhibited hemorrhagic content. Thus, the number of damaged glomeruli was quantified on each section. Exogenously administered EGF significantly reduced the number of collapsed glomeruli as compared to the control group (P = 0.04) (Table 2). The quantification of hemorrhagic foci on the cortical and medullary segments demonstrated that this damage was also significantly (P < 0.01) reduced by both EGF doses. Moreover, the second dose completely aborted the onset of cortical hemorrhages, and thus, no animal was detected exhibiting cortico-medullary hemorrhage. Lethal damages in tubular cells categorized here as irreversible changes, were always detected in the control group, although in a diffuse and rather individual tubular pattern, particularly involving the outer medulla tubuli. Again, EGF treatment reduced (P < 0.01) the incidence of this damage. Ischemia/reperfusion severely compromised the interstitial tissue in control rats. Edema with proteinaceous accumulation, hemorrhage, and tubuli walls distortions were frequently detected in that group. The incidence of this damage was reduced to more than a 75% in the animals treated with the first EGF dose level, whereas in the animals treated with the largest EGF dose, these changes were not detected (for both EGF does, P < 0.01). EGF treatment seemed to reduce the medullary inflammatory infiltrate and the recruitment of vessel luminal neutrophils. In general terms, the integrity of the renal tissue architecture was in relation to the magnitude of the EGF dose assayed. Figure A) Saline control-derived injured kidney.
Glomerular collapse associated to relative enlargement of the Bowman’s capsule
can be easily distinguished. In addition, a great number of tubules exhibiting
epithelial flattening can be seen (5 µm section, hematoxiline and eosine staining,
magnification x 25).
Table 2. Percent of animals with renal histopathological changes per group.
Data are expressed as mean ± SD, and were compared by a one-way
ANOVA and Duncan’s multiple rank test. *P < 0.01; **P <
0.05; both EGF doses vs. saline-treated control. Except for glomerular
collapse, significant differences were observed in the remaining parameters
when EGF doses were compared, Renal functional tests As previously described, renal functional assessment was based on the calculated clearance of PAH and In, as indicators of the RPF and of the GFR, respectively. Table 3 illustrates that ischemia/reperfusion impaired RPF although in a non-significant manner (P = 0.056) in animals receiving saline solution, whereas the intensity of the GFR was drastically reduced (more than twofold), as compared to the values calculated for sham ischemized rats (P < 0.01). The first EGF dose (500 µg/kg) was ineffective in preserving neither the RPF nor the GFR. In fact, the values registered in this group were undistinguished from those found in the saline control. The second EGF dose, however, significantly (P < 0.01) preserved the renal physiology, as the values obtained were within normal limits when compared to non-ischemic animals. Table 3. Renal functional tests.
Data are expressed as mean ± SD. *Significant reduction in glomerular
filtration rate (GFR) in the saline-treated control vs. the value obtained
from the sham ischemic animals, P = 0.002. **Difference between
rats treated with 750 µg/kg EGF vs. the saline control; (P = 0.0037
for renal plasma flow [RPF] and P = 0.005 for GFR). Comparisons
were performed by a one-way ANOVA and Duncan’s test. The significance established
was P < 0.05. Biochemical determinations As shown in table 4, as a consequence of the I/R episode the activity of the enzymes PLA2 and catalase was significantly elevated (3 and 1.5-fold respectively, P < 0.01) in control rats as compared to the sham ischemic group. In these animals the renal generation of the oxidative-stress metabolite MDA was also significantly increased (1.5-fold) with respect to non-ischemic rats (P < 0.01). With the EGF intervention, a significant reduction (P < 0.01) in the three parameters studied was detected as compared to the saline control group. Moreover, the most important reduction of the three biochemical parameters was found in the animals treated with the largest EGF dose, which supports the relevance of this dose in terms of morphologic and functional preservation. Table 4. Biochemical determinations in renal tissue.
Data are expressed as mean ± SD. Ischemia/reperfusion significantly
elevated the renal levels of malondialdehyde (MDA), and the activity of enzymes
catalase and PLA 2 in saline-treated vs. sham ischemic rats,
all *P = 0.0001. A significant reduction of the
markers was observed in animals receiving EGF, compared to saline control, all
**P = 0.001. Comparisons were performed by a one-way ANOVA
and Duncan’s test. The significance established was P < 0.05. MDA
is expressed in nmoL/mg of protein. Enzyme activity is expressed in U/g Discussion Different studies have repeatedly shown that the pharmacological use of EGF in the settings of ischemic or toxic acute renal injury accelerates regeneration and is therefore beneficial [for review see reference 24]. The potential benefits of the EGF prophylactic effects by virtue of its cytoprotective properties have remained much less explored, despite a tissue-protective intervention is frequently and urgently demanded in the therapeutic armamentarium [25]. This experiment has shown the prophylactic impact of a single instillation of exogenous EGF by affording renal protection and attenuating the consequences of the ischemic episode in a dose-dependent manner, when the growth factor was administered before creating an ischemic environment. Despite this model represents a mild ischemia time, kidney morphology and physiology were disrupted. Thus, in this context, renal damage may be explained by the fact that 30 min of ischemia is sufficient to deplete more than 90% of cellular ATP [26], and by the prolonged reperfusion allowed. The histological examination revealed the salutary effects of the EGF treatment, expressed by a more defined tissue architectural integrity and viability as compared to saline controls. EGF intervention ameliorated glomerular, tubular, and interstitial damages in a dose-dependent fashion. The effect of the second EGF dose was particularly relevant because it prevented the onset of cortical hemorrhages in all the animals studied. Hemorrhage prevention by EGF in this context may theoretically represent the attenuation of endothelial damage and dysfunction in response to locally generated free radicals, or the contribution of EGF to maintenance of the RPF autoregulation mechanisms. In correspondence with the morphological findings, rats treated with 750 µg/kg EGF exhibited a normal renal functioning as judged by the RPF and GFR indexes. In saline controls, however, GFR was reduced to more than 60%. In other words, in these animals ARF was prevented by extrapolating the definition that ARF is a rapid deterioration of kidney function with at least a 50% decrease in GFR [27]. Failure in regaining a normal RPF after ischemia has been attributed to the prevalence of the vasoconstrictor mediator endothelins, which also regulates the GFR [27]. In theory, EGF could preserve GFR by interfering with the endothelins-mediated vasoconstrictor mechanism, or alternatively, by favoring the production of vasodilator agents such as nitric oxide (NO) by endothelial cells [28]. Other lines of evidence show that mucosal hyperemia sustains the EGF-mediated gastroprotection [for review see 29], whereas an increased mucosal blood flow is induced and controlled by locally synthesized NO [30]. As aforementioned, the 500 µg/kg EGF dose did not show to attenuate renal functional failure, even when the kidney morphology appeared relatively well preserved. This disparity is not surprising and has been extensively recognized in humans affected by ARF. An explanation for this states that many sublethally injured tubular cells, while appearing intact, can still contribute to tubular leakiness and obstruction in the process of injury [31]. In the plethoric pathophysiology of ischemic renal injury, the generation of reactive oxygen species (ROS) by vascular, inflammatory and epithelial cells plays a critical role [32], whereas these cells are also the primary target of ROS toxicity [33]. ROS generation is particularly relevant in renal pathology since the medulla physiologically remains in a markedly hypoxic state rendering the organ very prone and vulnerable to hypoperfusion [34]. In this experiment, I/R provoked a significant intrarenal accumulation of the reactive by-product MDA as an increase in the enzymatic activity of catalase and PLA2. A global interpretation of the data obtained from the EGF-treated animals indicates that EGF contributed to reduce the generation of ROS and lipoperoxidative metabolites in a dose-dependent manner. The twofold reduction in catalase and PLA2 activity in animals receiving the highest EGF dose, suggests that EGF somehow prevented the formation or facilitated the neutralization of hydrogen peroxide, and that also prevented the over-production of inflammatory mediators (i.e., platelet-activating factor [PAF]), which may derive from free fatty acids and lysophospholipids released by PLA2 [35]. In other experimental systems, EGF has shown a marked antioxidant activity by stimulating the production of superoxide dismutase (SOD) [36]. Our group is currently investigating if SOD overexpression is part of the EGF-triggered protective mechanisms in renal I/R. In vitro and in vivo evidences converge to support our findings that the cytoprotective ability of EGF is expressed in reducing lethal tissue damages and the lipid peroxidation process. These findings include gastric stress ulcers [37], ozone cytotoxicity on airway epithelial cells [38], carbon tetrachloride-mediated liver necrosis [39], apoptosis by hyperoxia in cultured neurons [40], and cerebral injury by ischemia [41]. Finally, the absence of EGF in the culture medium of tubular epithelial cells results in apoptosis emphasizing the survival and renotrophic qualities of this polypeptide [42]. This work is possibly the first experimental demonstration of the beneficial effects of using exogenous EGF as a prophylactic resource in ischemic renal damage. Clinical experience has considered that prophylactic interventions with cytoprotective drugs are an urgent imperative need, particularly for those processes involved in the slippery slope of multiple organ dysfunction. Meanwhile, the systemic use of EGF alone or in combination with other polypeptide growth factor awaits clinical assessment in subjects prone to clinical or surgical ischemic episodes. References 1. Daemen M, van’t Veer C, Denecker G, Heemskerk VH, Wolf T, Clauss M, et al. Inhibition of apoptosis induced by ischemia-reperfusion prevents inflammation. J Clin Invest 1999;104:541–9. 2. Boonstra J, Rijken P, Humbel B, Cremers F, Verkleij A, en Henegouwen PvB. The epidermal growth factor. Cell Biol Int 1995; 413–30. 3. Goodlad RA, Wright N. Epidermal growth factor and transforming growth factor-a actions on the gut. Eur J Gastroenterol Hepatol 1995;7:928–35. 4. Berlanga J, Caballero M, Prats P, López-Saura P, Playford RJ. Reflexiones acerca del efecto citoprotector del factor de crecimiento epidérmico. Medicina Clínica 1999;113:222–30. 5. Humes HD, Cieslinski DA, Coimbra TM, Messana JM, Glavao C. Epidermal growth factor enhances renal tubule cell regeneration and repair and accelerates the recovery of renal failure. J Clin Invest 1989;84:1757–61. 6. Norman J, Tsau Y-K, Becay A, Fine LG. Epidermal growth factor accelerates functional recovery from ischemic acute tubular necrosis in the rat: role of the epidermal growth factor receptor. Clinical Science 1990;78:445–50. 7. Miller SB, Martin DR, Kissane J, Hammerman MR. Insulin-like growth factor I accelerates recovery from ischemic acute tubular necrosis in the rat. Proc Natl Acad Sci USA 1992;89:11876–80. 8. Coimbra TM, Ceilinsky DA, Humes HD. Epidermal growth factor accelerates renal repair in mercuric chloride nephrotoxicity. Am J Physiol 1990;59:F438–43. 9. Morin NL, Laurent G, Nonclercq D, Toubeau G, Heuson-Steinnon JA, Bergeron MG, et al. Epidermal growth factor accelerates renal tissue repair in a model of gentamicin nephrotoxicity in rats. Am J Physiol 1992;263:F806–11. 10. Schaudies RP, Johnson PJ. Multiple EGF containing proteins in rat kidney: increased soluble EGF following ischemia is accompanied by a decrease in membrane-associated EGF. Am J Physiol 1993;264: F523–31. 11. Hammerman MR. Potential role of growth factors in the prophylaxis and treatment of acute renal failure. Kidney International 1998;53 Suppl 64:S19–22. 12. Harris RC. Growth factors and cytokines in acute renal failure. Advances in Renal Replacement Therapy 1997;4:43–53. 13. Kennedy WA, Buttyan R, Garcia Montes E, D Agati V, Olsson CA. Epidermal growth factor suppresses renal tubular apoptosis following ureteral obstruction. Urology 1997;49(6):973–80. 14. Berlanga J, Caballero E, Lodos J, López-Saura P, Ramírez D, Playford RJ. Epidermal growth factor prevents multi-organ failure induced by thioacetamide. Gut 1999;44 Suppl 1:W280. 15. Fervenza FC, Tanny T, Rabkin R. Response to the intrerenal insulin-like growth factor-I axis to acute ischemic injury and treatment with growth hormone and epidermal growth factor. Kidney International 1996;49:344–54. 16. Barber E, Menéndez S, León OS, Barber MO, Merino N, Calunga JL, et al. Prevention of renal injury after induction of ozone tolerance in rats submitted to warm ischemia. Mediators of Inflammation 1999;8:37–41. 17. Smith HW, Tinkelstein N. The renal clearance of substituted hipuric acid derivatives and other aromatic acids in dog and man. J Clin Invest 1945;24: 388–91. 18. Schreiner G. Determination of inulin by means of resorcinol. Proc Soc exp Biol Med 1950;70:726–30. 19. Satoh K. Serum lipid peroxidation in cerebrovascular disorders determined by a new colorimetric method. Clin Chim Acta 1978;90:37–43. 20. León OS, Menéndez S, Merino N. Ozone oxidative preconditioning a protection against cellular damage by free radicals. Mediators of Inflammation 1998;7:289–94. 21. Hotter G, León OS, Catafú-Roselló J. Tissular prostanoid release phospholipase A2 activity and lipid peroxidation in pancreas transplantation. Transplantation 1991;51:987–90. 22. Spector T. Refinement of the coomasie blue method of protein quantification. Anal Biochem 1978;86:142–6. 23. Racusen LC. The histopathology of acute renal failure. In: Ronco C, Bellomo R, editors. Critical Care Nephrology. The Netherlands: Kluwer Academic Publishers; 1998. p.623–30. 24. Schena F. Role of growth factors in acute renal failure. Kidney International 1998; 53:S11–5. 25. Bukowski R. Cytoprotection in the treatment of pediatric cancer: review of current strategies in adults and their application to children. Medical Pediatric Oncology 1999;32(2):124–34. 26. De Vechi E, Lubatti L, Beretta C, Ferrero S, Rinaldi P, Galli Kinele M, et al. Protection from renal ischemia-reperfusion injury by the 2-mathylaminochroman U83836E. Kidney International 1998;54:857–63. 27. Agarwal A, Raij L. Endothelial dysfunction in acute renal failure. In: Ronco C, Bellomo R, editors. Critical Care Nephrology. The Netherlands: Kluwer Academic Publishers; 1998. p. 527–50. 28. Wang Y, Marsden PA. Nitric oxide synthases: biochemical and molecular regulation. Curr Opin Neprol and Hyperten 1995;4:12–22. 29. Uribe J, Barrett K. Nonmitogenic actions of growth factors: An integrated view of their role in intestinal physiology and pathophysiology. Gastroenterology 1997; 112:255–68. 30. Holzer P. Neural emergency system in the stomach. Gastroenterology 1998; 114:823–39. 31. Kroshian VM, Sheridan A, Lieberthal W. Functional and cytoskeletal changes induced by sublethal injury in proximal tubular epithelial cells. Am J Physiol 1994;266:F21–30. 32. Baud L, Ardaillou R. Involvement of reactive oxygen species in kidney damage. British Medical Bulletin 1993; 49:621–9. 33. Paller MS. The cell biology of reperfusion injury in the kidney. J Invest Med 1994;42:632–9. 34. Brezis M, Rosen S. Hypoxia of the renal medulla -its implications for disease. N Engl J Med 1995;332:647–5. 35. Saluja I, Song D, O’ Reagan MH, Phillis JW. Role of phospholipase A2 in the release of free fatty acids during ischemia-reperfusion in the rat cerebral cortex. Neurosci Lett 1997;233:97–100. 36. Price LT, Chen Y, Frank L. Epidermal growth factor increases antioxidant enzyme and surfactant system development during hyperoxia and protects fetal lungs in vitro from hyperoxic toxicity. Pediatric Res 1993;34:577–85. 37. Aricioglu A, Oz E, Erbas D, Gockora N. Effects of EGF and allopurinol on prostaglandin and lipid peroxide levels in mucosa of stomach in restrain cold stress. Prostaglandins Leukotrienes and Essential Fatty Acids 1996; 54:285–8. 38. Qin XQ, Sun XH, Lou ZQ, Guan CX, Zhang CQ. Cytoprotective effect of epidermal growth factor on cultured rabbit airway epithelial cells exposed to ozone. Acta Physiologica Sinica 1996;48:190–4. 39. Berlanga J, Caballero M, Ramírez D, Torres A, Valenzuela C, Lodos J, et al. Epidermal growth factor protects against carbon tetrachloride-induced hepatic injury. Clinical Science 1998; 94:219–23. 40. Yamada M, Enokido Y, Ikeuchi T, Hatanaka H. Epidermal growth factor prevents oxygen-triggered apoptosis and induces sustained signaling in cultured rat cerebral cortical neurons. European Journal of Neuroscience 1995;7(10):2130–8. 41. Peng H, Wen TC, Tanaka J, Maeda N, Matsuda S, Deskai J, et al. Epidermal growth factor protects neuronal cells in vivo and in vitro against transient forebrain ischemia-and free-radical induced injuries. J Cerebrovascular Blood Flow and Metabolism 1998; 18:349–60. 42. Lieberthal W, Triaca V, Brady E, Levine J. Apoptosis of renal epithelial cells: role of serum deprivation and oxidant injury. J Am Soc Nephrol 1994;5:902. Copyright Elfos Scientiae 2000 The following images related to this document are available:Photo images[ba00049a.jpg] |
| |||||||||

{kind=link}