 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Biotecnología Aplicada, Volume 17, July-September 2000, pp. 183-186 Validation of an ELISA for the Quantitation of Diphtheria Antitoxin in Human Serum @ Juan C Martínez Rodríguez,
Rolando Ochoa Azze, Argentina Cruces Perón, DACTA, Instituto Finlay. Ave. 27, No. 19805. La Lisa, AP 16017,
CP 11600, Received in October, 1999. Accepted for publication in June, 2000. Code Number: BA00053 Abstract An indirect solid-phase enzyme-linked immunosorbent assay (ELISA) was developed for the quantitation of antidiphtheria antibodies in human sera on the basis of a calibrated antibody standard. Intra- and inter-assay imprecision was around 10%. This assay showed an excellent accuracy (97.06% average recovery). Parallelism deviations were below 10%, which were evaluated with dilutions covering the working range of the standard curve. The detection limit of 0.0044 international units per milliliter (IU/mL) was sufficient for determining the immunological protection against diphtheria. In a preliminary study, a good correlation was found between the ELISA and the neutralization test in guinea pigs (R2 = 0.992). A wide range of diphtheria antitoxin quantitation made possible to classify 81 adults prior and four weeks after revaccination against diphtheria as: unprotected subjects (£ 0.01 U/mL), relatively protected (> 0.01–0.1 IU/mL), satisfactorily protected (> 0.1–1.0 IU/mL), and long-lasting protected (>1.0 IU/mL). Keywords: diphtheria antitoxin, ELISA, validation Resumen Validación de un ELISA para la cuantificación de anticuerpos antitoxina diftérica en sueros humanos. Se desarrolló un ensayo inmunoenzimático en fase sólida (ELISA) de tipo indirecto para la cuantificación de antitoxina diftérica en sueros humanos, con el empleo de un estándar previamente calibrado. Las imprecisiones intra e interensayo fueron de alrededor de 10%. Este ensayo también mostró una excelente precisión (recobrado medio de 97,06%). Las desviaciones del paralelismo estuvieron por debajo de 10%, las cuales se evaluaron con el empleo de diluciones que cubrían el intervalo de trabajo de la curva estándar. El límite de detección de 0,0044 unidades internacionales por mililitro (UI/mL) fue suficiente para determinar el grado de protección inmunológica contra la difteria. En un estudio preliminar, el ensayo mostró una correlación adecuada con la prueba de neutralización en conejillos de Indias (R2 = 0,992). Este inmunoensayo ofrece, además, un amplio intervalo de cuantificación, lo que permitió la clasificación de 81 individuos adultos antes y cuatro semanas después de la revacunación como: desprotegidos (£ 0,01 UI/mL), relativamente protegidos (> 0,01-0,1 UI/mL), satisfactoriamente protegidos (> 0,1-1,0 UI/mL) y protegidos por largo tiempo (> 1,0 UI/mL). Palabras claves: antitoxina diftérica, ELISA, validación Introduction Diphtheria is caused by Corynebacterium diphtheriae. This infection has become rare in developed countries. This is mainly due to postnatal vaccination programs carried out according to expert recommendations [1]. Coverage of infants in developing countries with three doses of a diphtheria-pertussis-tetanus (DPT) combined vaccine rose slowly to 46% in 1985, and to 81% in 1995 [2]. Unexpectedly, since the mid-1980s, there has been a striking resurgence of diphtheria in regions of Eastern Europe. The epidemic began in the Newly Independent States (NIS) of the former Soviet Union and was spread to neighboring countries in Europe, the Middle East, and Asia. Many of the diphtheria cases reported in 1993–1994 were imported from the NIS into other European countries (Finland, Germany and Poland). An immunity gap in adults coupled with the presence of large numbers of susceptible children and adolescents, creates the potential for an extensive epidemic, which has led to an increased world-wide concern about the level of immunity [3]. Diphtheria antitoxin antibody measurements play an important role in serological surveillance in humans. Traditionally, biological activity has been measured through toxin neutralization assays in guinea pigs or rabbits. However, during the last decades, attempts have been made to replace, when possible, these labor-intensive assays with cheaper and faster in vitro methods to reduce the large number of laboratory animals required for obtaining statistically valid results [4]. These assays include hemagglutination assays, enzyme-linked immunosorbent assays (ELISA), the toxin-binding inhibition (ToBI) test, and also a Vero cell assay. The hemagglutination test with diphtheria toxin or toxoid using sensitized erythrocytes is easier to perform and low in cost; however, this assay is only semiquantitative. More precise results might be obtained with an ELISA that defines titers over a continuous range. A home-made ELISA for diphtheria antitoxin may be an alternative method largely used for the rapid estimation of antitoxin antibodies in diagnostic laboratories, as well as for epidemiological studies [4]. Commercial kits are not advisable for large studies. A home-made ELISA was developed to measure anti-diphtheria toxin IgG antibodies in human serum. Materials and Methods Antigen In all experiments, a highly-purified diphtheria toxoid from Finlay Institute, Cuba, was used. It was prepared by treating purified toxin with formaldehyde. Batch 003/97 of 500-limit flocculation units per milliliter (Lf/mL) was used. A coating concentration of 8 Lf/mL showed a high sensitivity and a low background and, therefore, was used as antigen concentration in all experiments. Antitoxin A human serum pool from 20 normal adults aged 24–53 years was prepared to be used as local reference sera and substandard in the ELISA test. Adults were bled one month after revaccination with a tetanus-diphtheria (Td) adsorbed vaccine for people of 7 years old and older (CONNAUGHT Lab., Ontario, Canada, batch 1056-12). The human serum pool was carefully tested against local reference serum (batch ADRN 1/95), using intradermal neutralization test on the depilated skin of guinea pigs [5]. This reference was calibrated against the international WHO standard for diphtheria antitoxin (hyperimmune horse anti-serum containing 10 IU/mL). The human serum pool was diluted to 0.32 IU/mL with 6% (w/v) human serum albumin. ELISA procedure Diphtheria antitoxin levels were measured by ELISA in flat-bottomed polystyrene plates (COSTARâ E.I.A./R.I.A., Cat.N°3590, Costar, USA). The plates were coated with 100 µL of diphtheria toxoid diluted in 0.05 M sodium carbonate buffer (pH 9.6) and left overnight at 4 ºC. All the plates were then washed four times with sodium phosphate-buffered saline containing Tween 20 (PBST, 0.15 M NaCl, 0.01 M phosphates [pH 7.2], 0.05% Tween 20), and drained over a filter paper. Six twofold serial dilutions of the 0.32 IU/mL local reference serum (substandard) against diphtheria toxoid were prepared in PBST with 3% skim milk powder (Merck, Germany, Cat. N° 1.15363) (starting dilution 1:20). One-hundred microliters of each substandard dilution and of unknown serum samples were added to the wells of the plates, incubated at 37 ºC for 60 min, and washed four times with PBST. Negative serum samples in PBST with 3% skim milk powder were used as zero-standard. One-hundred microliters of sheep anti-human IgG (g-chain-specific)-alkaline phosphatase conjugate (Sigma A0287, USA), diluted 1:2000 in PBST with 3% skim milk powder, were added to each well, followed by incubation at 37 ºC for 60 min and further washing. One-hundred microliters of the substrate solution (1 mg/mL p-nitrophenyl-phosphate disodium [SIGMA 104Ò, USA] in 0.92 M diethanolamine buffer [pH 9.8]) were added to each well and incubated for 30 min at room temperature. Absorbance was determined at 405 nm using an ELISA reader (Anthos Labtec Instruments, Austria). The absorbance values were transformed to IU/mL using a public-domain software developed at the Center for Disease Control, Atlanta [6]. The four-parameter log-logistic function was used for constructing the reference curve [7]. Validation, quantitation of diphtheria antitoxin and printout were done using the ELISA software package [6]. Precision Intra- and inter-assay studies were performed using four serum samples of high, medium, and low antitoxin levels. The coefficient of variation (CV) was used in order to express the variations. Intra- and inter-assay experiments were done in replicates of 10 and 3 runs, respectively. Accuracy (recovery) Accuracy was studied using a recovery test by the addition of various amounts of analyte to an analyte-free specimen. Five serum samples of high, medium, and low antitoxin levels were diluted 1:2 with negative serum sample. Therefore, the expected value was defined as the half value of the undiluted positive sample. Accuracy was expressed as the percentage error between the obtained value and the expected value ([obtained value/expected value] x 100%) [8]. Dilution test Parallelism was tested by dilution experiments. Five serum samples of high, medium, and low antitoxin levels were assayed at three dilutions, covering the working range of the standard curve. The CV between the observed value at three different dilutions was used to evaluate the precision. Detection limit Detection limit was calculated after the zero-standards were tested 76 times. The mean plus twice the standard deviation (SD) was taken as an estimate of the detection limit [8, 9]. Correspondence between the ELISA and the neutralization test To establish the correspondence between ELISA titers and antitoxin units, 20 serum samples were assayed in both tests [5]. Taking antitoxin units by neutralization test as reference (independent variable x), a linear regression equation was then adjusted by least squares. Technical application Eighty-one normal adults aged 20–58 years were bled prior (T0) and four weeks (T1) after revaccination with a Td adsorbed vaccine (CONNAUGHT Laboratories, Ontario, Canada, batch 1056-12). Sera were stored at –20 ºC until simultaneous processing. The samples were carefully tested by an ELISA previously described for the determination of diphtheria antitoxin levels. Statistical analysis The statistical parameters [8, 9] were obtained using descriptive methods and a linear regression analysis performed with a statistical software on an IBM-compatible computer [10]. Geometric mean and 95% confidence intervals were calculated for diphtheria antitoxin distribution in T0 and T1 in reimmunized adults. Results and Discussion The neutralization tests in guinea pigs or rabbits are standard methods for estimating the levels of diphtheria antitoxin [5]. These in vivo methods show the functional capacity of antibodies to neutralize the toxin. In contrast, some in vitro tests not only show the neutralization of the toxin by the antibodies present in the test serum, but also reactions between other antigen-antibody systems. Therefore, the in vivo neutralization test should be used to calibrate and verify the in vitro tests routinely used in the laboratory [11]. Appropriate calibration using a WHO standard preparation was an important step enabling the reproducibility of the results. In vivo methods and in vitro procedures such as passive hemagglutination and neutralization tests in tissue culture have the disadvantage of being complex to handle and standardize, as well as being time-consuming. However, an indirect ELISA method is suitable for routine laboratory practice [12]. Both small and large specimen numbers were readily measured. We developed an indirect ELISA procedure that uses the diphtheria toxoid as capture antigen. A human serum pool showed an antitoxin concentration of 8.829 IU/mL by the intradermal neutralization test and was adjusted to 0.32 IU/mL with 6% (w/v) human serum albumin to be used as substandard. Intra- and inter-assay variations reflecting the precision of the test are shown in Tables 1 and 2. The ELISA test was reproducible with coefficients of variation around 10% within (intra-assay) and between runs (inter-assay). Table 1. Intra-assay precision of the ELISA test for diphtheria antitoxin quantitation.
x, mean value; CV, coefficient of variation. Table 2. Inter-assay precision of the ELISA test for diphtheria antitoxin quantitation.
x, mean value; SD, standard deviation, CV, coefficient of variation. A recovery experiment performed to determine the ability of the assay to measure the expected value revealed an excellent accuracy (Table 3). Accuracy provides an estimate of systematic errors and acceptable results are based on specifications for the actual reference value [9]. Table 3. Accuracy of the ELISA test for diphtheria antitoxin quantitation.
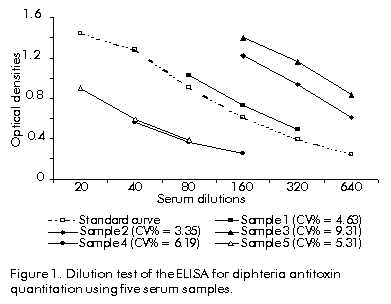
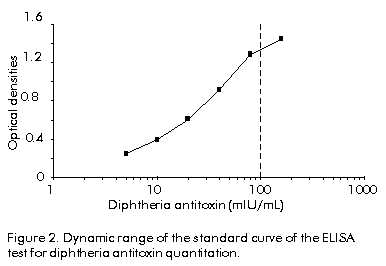
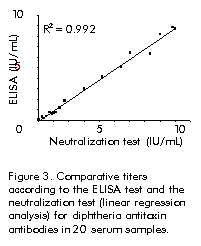
For the results of any analytical method to be valid, it is essential that the analyte in the calibration standard and in the tested samples shows the same behavior. For this reason, dilution of the samples with an appropriate diluent should normally have no effect on the calculated final result (dilution test). The samples assayed at three dilutions showed a small deviation in the observed value (CV < 10%) after correction for dilution (Figure 1). Figure 1. Dilution test of the ELISA for diphteria antitoxin quantitation using five serum samples. It has been shown that there is no a sharply defined level of antitoxin that provides a complete protection against diphtheria. A certain range of variation must be accepted; the same level of antitoxin may provide an unequal degree of protection in different individuals. Thus, antibody levels between 0.01 and 0.1 IU/mL may be regarded as giving basic immunity, whereas a higher antitoxin level might be required for achieving full protection. In some studies that used in vitro techniques, a level of 0.1 IU/mL was considered protective [12, 13]. The detection limit was 0.0044 IU/mL, and antitoxin levels ranging from 0.01 to 0.32 IU/mL (sample dilution of 1:20) or from 0.1 to 3.2 IU/mL (sample dilution of 1:200) could be measured (Figure 2). The assay covers a wide range of diphtheria antitoxin, which was found to be sufficient for routine test. Figure 2. Dynamic range of the standard curve of the ELISA test for diphtheria antitoxin quantitation. A good correlation between the ELISA and the neutralization test was found in this preliminary study (Figure 3). The determination coefficient (R2) was 0.992 for linear regression. The best-fit equation was, therefore, ELISA = 0.9849 neutralization test – 0.1039. However, antibodies detected by both techniques may not be the same. Perhaps, a better agreement between both assays could result from performing the ELISA with a toxoid antigenic fraction that might be more closely related to the protective antibodies. Figure 3. Comparative titers according to the ELISA test and the neutralization test (linear regression analysis) for diphtheria antitoxin antibodies in 20 serum samples. Table 4 shows an ELISA evaluation of diphtheria antitoxin levels prior (T0) and four weeks (T1) after diphtheria and tetanus revaccination. Sufficient diphtheria immunity, i.e. antitoxin titers > 0.1 IU/mL, was found in only 61.7% of the specimens prior revaccination. However, four weeks later, 95.0% of the subjects showed a sufficient anti-diphtheria immunity and 65.4% showed a long-lasting satisfactory immune protection (> 1.0 IU/mL). Table 4. Number (percentage) of subjects unprotected (£ 0.01 IU/mL), relatively protected (> 0.01–0.1 IU/mL), satisfactorily protected (> 0.1–1.0 IU/mL), and long-lasting protected (> 1.0 IU/mL), as determined by ELISA.
The ELISA test described in this paper for the quantitation of diphtheria antitoxin is a valuable tool for determining immunological protection against diphtheria and could be especially useful for population studies, since it is economical and practical for large-scale routine purposes. References 1. Expanded Programme on Immunization. Immunization Policy. Document WHO/EPI/GEN/95.3, World Health Organization, Geneva, Switzerland; 1995. 2. Galazka AM, Robertson SE. Immunization against diphtheria with special emphasis on immunization of adults. Vaccine 1996;14(9):845–57. 3. Hasselhorn HM, Nubling M, Tiller FW, Hofmann F. Factors influencing immunity against diphtheria in adults. Vaccine 1998;16:70–5. 4. Bonin E, Tiru M, Hallander H, Bredberg-Raden U. Evaluation of single- and dual antigen delayed fluorescence immunoassay in comparison to an ELISA and the in vivo toxin neutralisation test for detection of diphtheria toxin antibodies. J Immunol Methods 1999;230:131–40. 5. Glenny AT, Llewellyn-Jones M. The intracutaneous method of testing diphtheria toxin and antitoxin. J Path Bacteriol 1931;34:143–56. 6. Plikaytis BD, Holder PF, Carlone GM. Program ELISA for Windows. User’s manual. Center for Disease Control and Prevention, Atlanta, GA, USA; 1996. 7. Plikaytis BD, Turner SH, Gheesling LL, Carlone GM. Comparisons of standard curve-fitting methods to quantitate Neisseria meningitidis group A polysaccharide antibody levels by enzyme-linked immunosorbent assay. J Clin Microbiol 1991; 29:1439–46. 8. Chaloner-Larsson G, Anderson R, Egan A. A WHO guide to good manufacturing practice (GMP) requirements. Part 2: Validation. Validation of analytical assays. WHO Geneva; 1997. p.65–95. 9. Broughton PMG, Bergonzi C, Lindstedt G, Loeber IG, Malan PG, Mathieu M, et al. Guidelines for a user laboratory to evaluate and select a kit for its own use. Part 1. Quantitative tests. European Committee for Clinical Laboratory Standard 1986;3:3. 10. STATGRAPHICS Plus for Windows [computer program]. Version 1.0. Statistical Graphics Corp, USA; 1994. 11. Skoura L, Efstratiou A, Tsakris A, Pournaras S, George RC, Douboyas J. Study on the use of an enzyme-linked immunosorbent assay in determining human antibodies to diphtheria toxin as compared with a reference toxin neutralization assay. Comp Immunol Microbiol Infect Dis 1999;22:181–6. 12. Bergamini M, Comodo N, Gasparini R, Gabutti G, Fabrizi P, Severini R, et al. Prevalence of diphtheria toxin antibodies in human sera from a cross-section of the Italian population. Vaccine 1999;17:286–90. 13. Souliou E, Kyriazopoulou V, Diza E, Hatzistylianou M, Frantzidou F. Serological survey on the immunity to diphtheria of the northern Greek population. Eur J Epidemiol 1997;13:535–9. Copyright Elfos Scientiae 2000 The following images related to this document are available:Photo images[ba00053c.jpg] [ba00053b.jpg] [ba00053a.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}