 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
ARTICULO ORIGINAL COMPLETO / FULL ORIGINAL PAPER
HUMORAL IMMUNOLOGICAL RESPONSE OF PATIENTS WITH EPIDEMIC NEUROPATHY AGAINST A VIRUS ISOLATED FROM THE CEREBROSPINAL FLUID OF A CLINICAL CASE Alexis Musacchio, Luis Herrera, Pilar Rodriguez, Reinaldo Alvarez, Martha Gonzalez-Griego, Eduardo Penton and Jose de la Fuente. Group for the Study of the Epidemic Neuropathy. Centro de Ingenieria Genetica y Biotecnologia. P.O. Box 6162, La Habana, Cuba.
Code Number: BA95051
Sizes of Files:
Text: 38K
Graphics: Photos (jpg) 344KRecibido en enero de 1995. Aprobado en julio de 1995. Keywords: coxsackie, epidemic neuropathy, immunology, virus.
SUMMARY Serum specimens from patients with epidemic neuropathy (EN) were tested in immunoblots for the presence of IgG, IgM and IgA antibodies against the structural proteins of: a virus isolated from the cerebrospinal fluid of a patient (isolate C-47), coxsackie B2 and poliovirus. Sera from blood bank donors, healthy workers from the CIGB and healthy children were used as controls. All the sera had IgG antibodies against the C-47 VP0 protein, but only sera from patients with EN had IgG and/or IgM/IgA antibodies against the C-47 VP1 protein. Immunological response to poliovirus was as expected for a vaccinated population. Practically all the sera recognized the viral VP1 structural protein, as the most important protein for protection against this virus. In the case of coxsackie virus B2 (CVB2), most of the sera recognized VP0, VP1 and VP2 structural proteins, thus indicating the previous circulation of this virus among the population. Antibodies against the C-47 isolate were detected in the CSF of the patients but not in healthy controls. The data obtained from the analysis of areas with low and high incidence of the disease showed that the virus associated with the EN circulated among the population. These results supported our hypothesis that the causal agent of the disease could be the virus in combination with nutritional deficiencies and stress that made the population more susceptible to the appearance of clinical symptoms because of the infection with the virus, although it could play the main role in the neurological damage.
RESUMEN Muestras de suero de pacientes con neuropatia epidemica (EN) se analizaron en inmunoblots para la presencia de anticuerpos tipo IgG, IgM e IgA contra las proteinas estructurales de un virus aislado del liquido cefalorraquideo (LCR) de un paciente (aislamiento C-47), virus coxsackie B2 (CVB2) y polio. Se emplearon como control sueros provenientes de donantes de sangre, trabajadores sanos del CIGB y ninos sanos. Todos los sueros mostraron reaccion frente a la proteina VP0 del C-47, pero solo los provenientes de pacientes con EN tenian IgG y/o IgM/IgA contra la proteina VP1. La respuesta inmunologica frente al virus polio fue la esperada para una poblacion vacunada. Practicamente todos los sueros reconocian la VP1 como la proteina mas importante para la proteccion frente al virus polio. Para el virus CVB2, la mayoria de los sueros reconocieron las proteinas VP0, VP1 y VP2, indicando la previa circulacion de este virus en la poblacion. Se detectaron anticuerpos tipo IgG contra el aislamiento C-47 en el LCR de pacientes y no en controles sanos. Los datos obtenidos de regiones con baja y alta incidencia de la enfermedad mostraron que el virus asociado a la EN circulo en la poblacion. Estos resultados apoyaron nuestra hipotesis de que el agente causal de la EN puede ser el virus en combinacion con deficiencias nutricionales y stress que hacen a la poblacion mas susceptible a la aparicion de sintomas clinicos producto de la infeccion con el virus, aunque este pueda jugar el papel fundamental en el dano neurologico.
INTRODUCTION An epidemic of neuropathy producing central and peripheral symptoms appeared in Cuba between 1991 and 1993. The clinical and epidemiological characterization of the disease has been published elsewhere (Llanos et al., 1993). The disease was termed epidemic neuropathy (EN) and three clinical forms were identified: purely ocular (optic neuropathy), peripheric neuropathy and mixed cases. About 50 000 cases were diagnosed until October 1993. Different hypothesis about the etiology of the disease were suggested.woxic-nutritional and biological factors were argued as being involved in the pathogenesis of the epidemic. The toxic-nutritional hypothesis was supported by laboratory evidences and may play a role as a background conditioning requirement for the disease. Two types of viral cytopathic effects (CPE) were observed when the cerebrospinal fluid (CSF) from patients was inoculated into a Vero cell monolayer. Most of the samples showed a weak, slowly progressing and delayed CPE (Rodriguez et al., 1994) and some other samples showed an enterovirus-like CPE that was characterized as Coxsackievirus A9 (CoxA9) by a neutralization test with the Limb-Beyesh-Melnick (LBM) pool of sera and by partial determination of the virus genome sequence (Mas et al., 1993; Roca et al., 1994; Riego et al., 1994). Coxsackievirus, which include 23 group A serotypes (CVA-1 to CVA- 22 and CVA-24) and six group B serotypes (CVB-1 to CVB-6), are common infectious agents that cause a wide spectrum of diseases, ranging from flu-like symptoms to severe infections of the central nervous system (More, 1982). They belong to the enterovirus genus of the Picornaviridae family. Like the other members of the family, the coxsackievirus are non enveloped icosahedral viruses of approximately 28 nm (300 A). Each virion contains one copy of a single-stranded messenger-sense RNA genome of approximately 7 500 nucleotides, enclosed in a roughly spherical capsid. A single polypeptide is post-translationally processed through two precursors (VP4 + VP2 = VP0 (~ 37.4 kDa) and VP1 + VP3) to originate the four coat protein subunits. The capsid is composed of 60 copies of each of the four coat protein subunits VP1 (~ 33 kDa), VP2 (~ 30 kDa), VP3 (~ 26 kDa), VP4 (~ 7.4 kDa). The development of the infection produced by the enteroviruses is characterized by a significant antibody response. During infection, antibodies to the denatured viral antigens appear before antibodies to the native antigens, and subsequently the levels of antibodies to the denatured antigens are the first to fall (Melnick, 1990). The immune response to enterovirus infection consists mainly in the production of neutralizing antibodies as demonstrated by the severity of these infections in agammaglobulinemic patients (MacKinney et al., 1987). The detection of serum antibodies to enterovirus is widely used for the diagnosis as a complement to virus isolation and more recently to virus detection by hybridization. Although most of the CSF samples from patients with EN showed a CPE not typical for enteroviruses, these isolates presented some similarities with this genus in the size and morphology of the virus particles (Rodriguez et al., 1994), in the crossreactivity of viral epitopes (Castro et al., 1994), and, at least for some of them, in the genome sequence as shown by PCR analysis (Alvarez et al., 1995). This fact suggested that we could be dealing with a mutant enterovirus or a new unidentified virus. However, due to the difficulties in growing these viruses and considering the existence of some degree of homology between these viruses and the coxsackievirus, the characterization of the immunological response of patients with EN was performed against a virus isolate classified as coxsackievirus A9 obtained from the CSF of a patient (isolate C-47/IPK). Here it was shown that patients with EN had a characteristic immunological response against C-47 viral proteins and that the virus circulated in the population. The relevance of these findings for the multicausal hypothesis of the etiology of the EN is discussed.
MATERIALS AND METHODS Virus preparation The C-47/IPK (C-47) isolate (classified as coxsackievirus A9) was obtained at the Tropical Medicine Institute "Pedro Kouri" (IPK) from the CSF of a female adult patient with EN showing essentially optical symptoms. The coxsackievirus B 2 (CVB2) and polio 1 virus strains were employed as references and were obtained from the IPK collection. Viruses were propagated twice in Vero cells prior to analysis. After propagation in Vero cells, virus were partially purified (Falcon et al., 1994). Samples of the CSF and sera from patients and controls Samples were aseptically collected from the hospitals and transported in ice to the CIGB. At the center, samples received a code number and were aliquoted and stored at -20 C until use. Characteristics of the individuals from whom the samples were collected are summarized in tables 1 and 2. Immunobloting SDS:polyacrylamide gel electrophoresis (SDS-PAGE) was performed according to the procedure described by Laemmli (1970). For electrophoresis, 400 ug of the virus preparation were diluted 1:2 in 2X electrophoresis sample buffer (1x: 0.0625 M Tris-HCl, pH 6.8, 2% SDS, 10% glycerol, 5% beta-mercaptoethanol, 0.01% bromophenol blue), placed in a boiling water bath for 20 min at 100øC and loaded into a 10 cm long slot. SDS-PAGE were run for 45-60 minutes with a 20 mA constant current at room temperature on a 0.75 mm thick 10% polyacrylamide gel (pH 8.8) with a 3% acrylamide concentration gel (pH 6.8). After electrophoresis, the antigens were transferred from the gel to 0.2 um pore size nitrocellulose filters (Schleicher & Schuell, Germany) in an electroblotting buffer containing 0.025 M Tris-HCl, 0.15 M glycine, 20% methanol, pH 8.3, for 1h at 40V. After blotting, the membrane was stained with Ponceau S-red to demonstrate successful transfer of proteins to the nitrocellulose membrane. The filters were washed 3 times for 10 min in PBS and incubated for 1h at 37 C in a blocking solution containing 5% skim milk (Oxoid, England) in PBS. Later, the membrane was cut in 3 mm wide strips. Serum samples were added (human serum 1:20) and the strips were incubated for 2h at room temperature with continuous shaking. The strips were washed 3 times, for 10 min each in PBS and horseradish-peroxidase-conjugated goat antihuman IgG, IgA or IgM antibodies were added in 5% milk in PBS. The incubation was for 1h at room temperature with shaking. The strips were then washed once for 10 min in PBS, once for 5 min in 0.02 % NP-40 in PBS and once for 5 min in PBS, and placed in a color developing solution (5 mL 4-Cl-I-naphtol dissolved in 1 mL methanol, 15 uL hydrogen peroxide and 25 mL PBS). The reaction was stopped after 15 min by dipping the blots in distilled water.
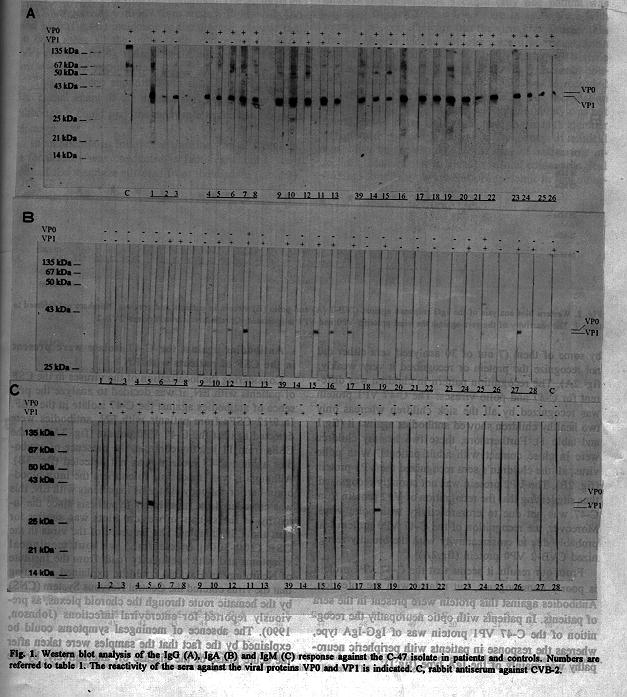
RESULTS AND DISCUSSION The C-47 virus isolate elicited a characteristic differential response in patients with EN In an attempt to find out if the immunological response against the C-47 isolate was masked by the presence in the sera of the population of antibodies against enteroviruses that have previously circulated in the country (P. Mas, personal communication) or by the response against the poliovirus vaccine, immunoblots were performed with the sera of patients and controls against C-47, CVB2 and polio viruses. As shown in figure 1A, all the sera examined had IgG against the C-47 VP0 protein because of the crossreactivity of this protein among the enteroviruses.
Table 1 Data from patients and controls included in these studies.
-------------------------------------------------------------
No. Patients and controls Specimen Sex Clinical Region
(Number of the diagnosis^b
clinical history)^a
-------------------------------------------------------------
1 4478, from a blood Serum M Healthy C. Habana
donor bank
2 4479, from a blood Serum F Healthy C. Habana
donor bank
3 4451, from a blood Serum M Healthy C. Habana
4 1-T, from CIGB Serum M Healthy C. Habana
5 2-T, from CIGB Serum F Healthy C. Habana
6 3-T, from CIGB Serum M Healthy C. Habana
7 7-T, from CIGB Serum M Healthy C. Habana
8 11-T, from CIGB Serum F Healthy C. Habana
9 Q1082 Serum M ON P. del Rio
10 Q1095 Serum M ON P. del Rio
11 Q1096 Serum F ON P. del Rio
12 54790 Serum M ON P. del Rio
13 Q1657 Serum M ON P. del Rio
14 90072 Serum M PN P. del Rio
15 Q1183 Serum M PN P. del Rio
16 Q1180 Serum F PN P. del Rio
17 4NP Serum NR PN Stgo. de Cuba
18 5NP Serum NR PN Stgo. de Cuba
19 6NP Serum NR PN Stgo. de Cuba
20 7NP Serum F PN Stgo. de Cuba
21 8NP Serum M PN Stgo. de Cuba
22 9NP Serum F PN Stgo. de Cuba
23 161-N, child Serum M Healthy C. Habana
24 O-1-B-N, child Serum F Healthy C. Habana
25 N-17-N, child Serum M Healthy C. Habana
26 OHB8-N, child Serum M Healthy C. Habana
27 E-1, child Serum F ON C. Habana
28 E-2, child Serum F ON C. Habana
29 Q1207 CFS and Serum M ON P. del Rio
30 Q1204 CFS and Serum F ON P. del Rio
31 51094 CFS and Serum F ON P. del Rio
32 N0131 CFS and Serum F ON P. del Rio
33 Q1216 CFS and Serum F ON P. del Rio
34 Q1222 CFS and Serum M ON P. del Rio
35 Q1044 CFS and Serum M ON P. del Rio
36 Q1178 CFS and Serum F PN P. del Rio
37 Q184 CFS and Serum F PN P. del Rio
38 Q1173 CFS and Serum M PN P. del Rio
39 Q1174 CFS and Serum M PN P. del Rio
40 N0143 CFS and Serum M ON P. del Rio
41 FP16 CFS and Serum F Healthy C. Habana
42 FP18 CFS and Serum M Healthy C. Habana
43 FP19 CFS and Serum F Healthy C. Habana
44 FP20 CFS and Serum F Healthy C. Habana
45 FP21 CFS and Serum F Healthy C. Habana
46 FP22 CFS and Serum M Healthy C. Habana
47 FP6 CFS and Serum F Healthy C. Habana
48 FP8 CFS and Serum F Healthy C. Habana
49 FP9 CFS and Serum M Healthy C. Habana
50 FP11 CFS and Serum M Healthy C. Habana
51 FP12 CFS and Serum M Healthy C. Habana
52 SJ1 Serum F Healthy San Juan
53 SJ2 Serum F Healthy San Juan
54 SJ3 Serum F Healthy San Juan
55 SJ4 Serum F Healthy San Juan
56 SJ5 Serum M Healthy San Juan
57 SJ6 Serum F Healthy San Juan
58 SJ7 Serum F Healthy San Juan
59 SJ8 Serum F Healthy San Juan
60 SJ9 Serum F Healthy San Juan
61 SJ10 Serum F Healthy San Juan
62 SJ11 Serum F Healthy San Juan
63 SJ12 Serum M Healthy San Juan
64 SJ13 Serum F Healthy San Juan
65 SJ14 Serum F Healthy San Juan
66 SJ15 Serum M Healthy San Juan
67 SJ16 Serum F Healthy San Juan
68 SJ17 Serum F Healthy San Juan
69 SJ18 Serum F Healthy San Juan
70 SJ19 Serum M Healthy San Juan
71 SJ20 Serum F Healthy San Juan
72 SJ21 Serum F Healthy San Juan
73 SJ22 Serum F Healthy San Juan
74 SJ23 Serum M Healthy San Juan
75 SJ24 Serum M Healthy San Juan
76 SJ-E-1 Serum F PN San Juan
77 SJ-E-2 Serum F PN-ON San Juan
78 SJ-E-3 Serum F ON San Juan
79 SJ-E-4 Serum F ON-PN San Juan
80 SJ-E-5 Serum M PN San Juan
81 SJ-E-6 Serum M PN San Juan
82 C-1 Serum M Healthy Candelaria
83 C-2 Serum F Healthy Candelaria
84 C-3 Serum M Healthy Candelaria
85 C-4 Serum F Healthy Candelaria
86 C-5 Serum F Healthy Candelaria
87 C-6 Serum F Healthy Candelaria
88 C-7 Serum F Healthy Candelaria
89 C-8 Serum M Healthy Candelaria
90 C-9 Serum F Healthy Candelaria
91 C-10 Serum M Healthy Candelaria
92 C-11 Serum F Healthy Candelaria
93 C-12 Serum F Healthy Candelaria
94 C-13 Serum M Healthy Candelaria
95 C-14 Serum F Healthy Candelaria
96 C-15 Serum F Healthy Candelaria
97 C-16 Serum F Healthy Candelaria
98 C-17 Serum F Healthy Candelaria
99 C-18 Serum F Healthy Candelaria
100 C-19 Serum M Healthy Candelaria
101 C-20 Serum M Healthy Candelaria
102 C-30 Serum M Healthy Candelaria
103 C-E-1 Serum M ON Candelaria
104 C-E-2 Serum F ON Candelaria
105 C-E-3 Serum F ON Candelaria
106 C-E-4 Serum F ON Candelaria
107 C-E-5 Serum F ON Candelaria
108 C-E-6 Serum F ON Candelaria
109 C-E-7 Serum F ON Candelaria
110 C-E-8 Serum M ON Candelaria
111 CI1 Serum NR Healthy Caimanera
112 CI2 Serum NR Healthy Caimanera
113 CI3 Serum NR Healthy Caimanera
114 CI4 Serum NR Healthy Caimanera
115 CI5 Serum NR Healthy Caimanera
116 CI6 Serum NR Healthy Caimanera
117 CI7 Serum NR Healthy Caimanera
118 CI8 Serum NR Healthy Caimanera
119 CI51 Serum NR Healthy Caimanera
120 IM299 Serum NR Healthy Imias
121 IM300 Serum NR Healthy Imias
122 IM301 Serum NR Healthy Imias
123 IM302 Serum NR Healthy Imias
124 IM303 Serum NR Healthy Imias
125 IM304 Serum NR Healthy Imias
126 IM305 Serum NR Healthy Imias
127 IM306 Serum NR Healthy Imias
128 IM307 Serum NR Healthy Imias
-------------------------------------------------------------
^aAdult individuals (> 20 years old) unless otherwise
stated. Individuals included in the focal studies are in Table
2.^bHealthy controls were obtained from blood donors, CIGB workers and surgical patients. Patients with EN were classified according to the predominant symptoms in optic neuropathy (ON) and peripheric neuropathy (PN). NR: not recorded.
Table 2 Data from individuals included in the focal studies
-------------------------------------------------------------
Focus No. Sex Age Living Relat- Suspected Diag- Observat-
together ionship by nosis ions
with the interview confirmed
a b c d
--------------------------------------------------------------
I 1 F 36 * Patient * * ON-PN
2 M 17 * Son NORMAL
3 F 9 * Daughter NORMAL
4 F 36 Neighbor NORMAL
5 F 29 Neighbor NORMAL
II 6 F 40 * Patient * * PN
7 F 71 * Mother NORMAL
8 F 14 * Daughter NORMAL
9 M 6 * Son NORMAL
10 M 47 Sexual NORMAL
11 F 20 Neighbor NORMAL
III 12 F 30 * Patient * * PN
13 M 30 * Husband NORMAL
IV 14 F 47 * Patient * * ON-PN
V 15 F 23 * Patient * * ON-PN
16 F NR * Mother Normal
17 M 59 * Father Normal
18 F 26 Friend * * ON-PN
19 F 47 Coworker PN
VI 20 M 73 * Patient * * PN
VII 21 M 35 * Patient * * ON
22 F 31 * Wife NORMAL
VIII 23 F 24 * Patient * * PN
24 F 46 * Mother PN
25 M 52 * Father * * PN
26 F 27 * Brother * Normal
27 M 20 BrotherON- PN
28 F 52 Neighbor * PN
29 F 22 Neighbor * PN
IX 30 M 11 * Patient * * ON-PN
31 F 2 * Brother Normal
32 F 30 * Mother * PN
32 M 36 * Father * * PN
X 34 F 13 * Patient * * ON-PN
35 F 12 * Patient * ON-PN
36 F 6 * Brother Normal
37 F 32 * Mother * ON-PN
38 M 63 Father * * PN
39 M 14 Brother Normal
------------------------------------------------------------
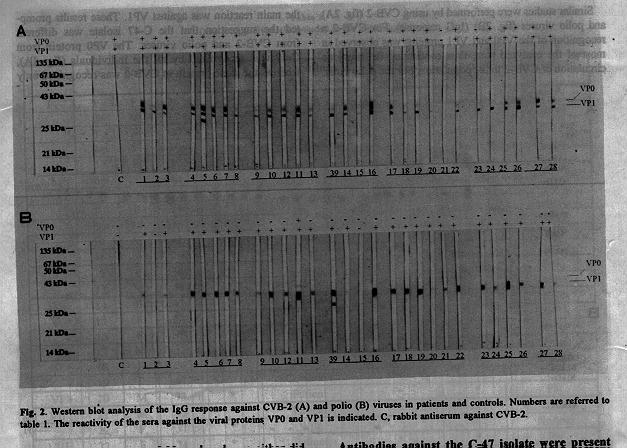
^aLiving in the same house.^bClinical symptoms of EN referred by the patient and observed during the focal study. ^cDiagnosis confirmed according to the clinical specifications of the disease. ^dPatients were classified according to the predominant symptoms in optic neuropathy (ON) and peripheric neuropathy (PN). However, the recognition of the C-47 VP1 protein was achieved only in the sera of patients or in that of people exposed to the virus (fig.1A and table 1). The IgA (fig.1B) and IgM (fig.1C) response against the C-47 isolate was also detected in the sera of adult patients and children, including two healthy children (fig.1A, C and table 1). Similar studies were performed by using CVB-2 (fig. 2A) and polio viruses (fig. 2B) (IgG response). For CVB-2 a recognition of the VP0 and VP1 proteins was observed in most of the analyzed sera, thus confirming the previous circulation of CVB-2 in the population. For the polio virus, the main reaction was against VP1. These results prompted the suggestion that the C-47 isolate was different from CVB-2 and polio viruses. The VP0 protein from C-47 was recognized by all the individuals (fig. 1A), whereas the same protein in CVB-2 was recognized only by some of them (7 out of 30 analyzed sera either did not recognize the protein or recognized it very weakly; fig .2A). The recognition pattern in children was different for C-47 and polio viruses. The C-47 VP1 protein was recognized by all the sick children whereas only two healthy children showed antibodies against it (fig.1 and table 1). Furthermore, these two healthy children were in close contact with adult patients. With polio virus, all the children's sera recognized the VP1 protein (fig. 2B). The VP2 protein was not strongly recognized, thus suggesting that the recognition of VP2 protein from C-47 was not due to crossreactivity with polio virus. Moreover, the recognition of the C-47 VP0 protein was probably due to crossreactivity with the broadly recognized CVB-2 VP0 protein (fig.2A).
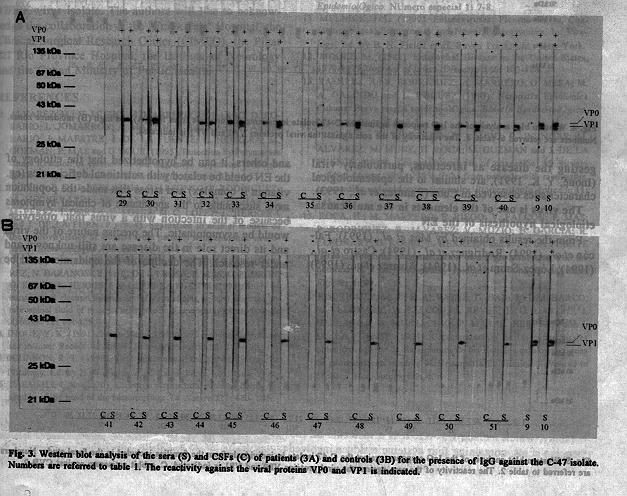
From our results it seems that the C-47 VP1 protein is poorly immunogenic, but related with the infection. Antibodies against this protein were present in the sera of patients. In patients with optic neuropathy the recognition of the C-47 VP1 protein was of IgG-IgA type, whereas the response in patients with peripheric neuropathy was mainly of the IgA type (fig.1). Antibodies against the C-47 isolate were present in the CSF of patients with EN Considering the localization of the viruses in the CSF of patients with EN, it was decided to analyze the presence of antibodies against the C-47 isolate in the CSF. In 9/12 CSFs from patients with EN, antibodies were detected against the C-47 VP0 protein (fig. 3A). In the CSFs from 11 healthy controls, the presence of antibodies against C-47 proteins was not detected (fig. 3B). Although it was impossible to confirm the intra-blood-brain-barrier antibody synthesis in patients with EN, this was considered the most likely hypothesis since the intensity of the signals in western blots was similar for sera and CSF samples. The presence of the virus in the CSF (200-300 particles/mL) without meningeal symptoms and with acellularity (data from the Institute of Neurology in Havana) could be explained assuming that the virus entered the Central Nervous System (CNS) by the hematic route through the choroid plexus, as previously reported for enteroviral infections (Johnson, 1990). The absence of meningeal symptoms could be explained by the fact that the samples were taken after the acute phase of the disease or, alternatively, by the absence of tropism of these viruses for the CNS. However, in an attempt to explain the role of the virus in the EN, this is one of the most contradictory facts.
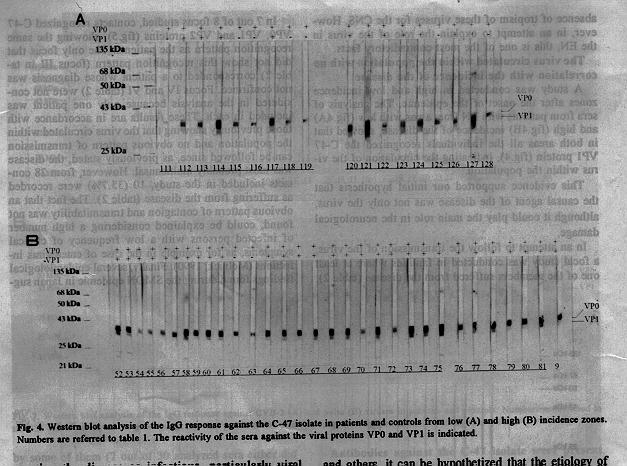
The virus circulated within the population with no correlation with the incidence of the disease A study was conducted in high and low incidence zones after the onset of the epidemic. The analysis of sera from patients with EN from areas with low (fig.4A) and high (fig.4B) incidence of the disease, showed that in both areas all the individuals recognized the C-47 VP1 protein (fig.4), indicating the circulation of the virus within the population.
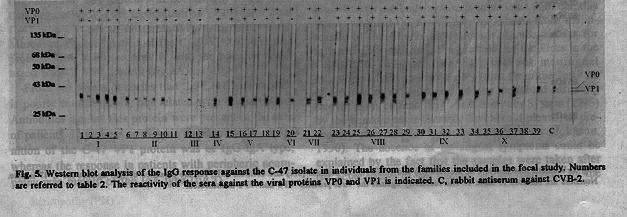
This evidence supported our initial hypothesis that the causal agent of the disease was not only the virus, although it could play the main role in the neurological damage. In an attempt to follow the transmission of the virus, a focal study was conducted in families where at least one of the members suffered from the disease (table 2). In 7 out of 8 focus studied, contacts recognized C-47 VP0, VP1 and VP2 proteins (fig.5), showing the same recognition pattern as the patients. The only focus that did not show this recognition pattern (focus III in table 2) corresponded to a patient whose diagnosis was not confirmed. Focus IV and VI (table 2) were not considered in the analysis because only one patient was included in each. These results are in accordance with those previously showing that the virus circulated within the population and no obvious pattern of transmission can be followed since, as previously stated, the disease was most probably multicausal. However, from 28 contacts included in the study, 10 (35.7%) were recorded as suffering from the disease (table 2). The fact that an obvious pattern of contagion and transmitability was not found, could be explained considering a high number of infected persons with a low frequency of clinical symptoms, as for example in the case of enterovirus infections (Melnick, 1990). Finally, several epidemiological findings found during the SMON epidemic in Japan suggesting the disease as infectious, particularly viral (Inoue, Y. K. 1991), are similar to the epidemiological characteristics observed in Cuba (Ramirez et al., 1993).
The virus is one of the elements in the multicausal etiological hypothesis of the EN From the results obtained by Mas et al., (1993); Falcon et al., (1994); Rodriguez et al., (1994); Castro et al., (1994); Lopez-Saura et al., (1994); Alvarez et al., (1995) and others, it can be hypothetized that the etiology of the EN could be related with nutritional deficiencies (eg. vitamin B complex) and stress that made the population more susceptible to the appearance of clinical symptoms because of the infection with a virus that, otherwise, would be asymptomatic. The precise nature of the virus and its direct role in the disease are still unknown and under research. The decline of the epidemic could be explained by the elimination of the predisposing element, by the elimination of susceptible persons in the population or by a combination of both factors. The vitamin administration to the population would prevent the appearance of the clinical symptoms but not spread of the virus. Thus, the seroconvertion in different groups and regions will not be related with the disease and should be essentially the same. The recombinant human interferon-alpha2b (HeberonR, Heber Biotec S.A., Havana, Cuba) therapy, that resulted useful for the treatment of the peripheral neuritis associated to the EN (Lopez-Saura et al., 1994), will act on the virus without eliminating the predisposing element. Furthermore, in some cases, people that eventually recover from the disease could relapse again with clinical symptoms. However, in a population with a good nutritional balance, the risk of the appearance of the disease should be low.
ACKNOWLEDGEMENTS We wish to thank Dr. P. Mas for providing the C-47/IPK virus isolate. The authors will like to acknowledge the collaboration of the "Frank Pais" Hospital, the Clinical-Surgical Research Center (CIMEQ), the Pinar del Rio Province Hospital, the Institute of Neurology and the Cuban Ministry of Public Health.
REFERENCES 1. ALVAREZ, M.; V. MUZIO; M. MARRERO; M. BARRO; D. ROSARIO; L. JOMARRON; A. MARTIN; C. SARIOL; M. CANDELARIO; J. MAESTRE; J. DE LA FUENTE; L. HERRERA; M. GUZMAN; P. MAS and G.KOURI (1995). Detection by Polymerase Chain Reaction of enterovirus-like sequences in patients with epidemic neuropathy in Cuba. BiotecnologIa Aplicada 12: 46-51. 2. CASTRO, F. O.; J. BERLANGA; C. ALFONSO; P. RODRIGUEZ; M. HECHEVARRIA; O. HAYES; R. PEREZ; D. PICHARDO; M. PEREZ; I. DORTA; E. LOPEZ; M. C. LOPEZ; L. HERRERA and J. DE LA FUENTE (1994). Evaluation in animal models of the neurovirulence of isolates from patients with epidemic neuropathy. BiotecnologIa Aplicada 11: 138-144. 3. FALCON, V.; J. REYES; O. ANCHETA; P. RODRIGUEZ; R. ALVAREZ; N. BARANOSKY; M. C. DE LA ROSA; P. MAS; G. PADRON; G. KOURI; L. HERRERA and J. DE LA FUENTE (1994). Study by transmission electron microscopy of virus strains isolated from the cerebrospinal fluid of patients with epidemic neuropathy. BiotecnologIa Aplicada 11: 151-159. 4. INOUE, Y. K. (1991). Inoue-Melnick virus and associationed diseases in man: Recent Advances. Prog. Med. Virol. 38: 167-179. 5. JOHNSON, R. T. (1990). Viral Infections of the Nerval System. In: Virology, Ed. by B. N. Fields et al. Raven Press, Ltd., New York. 6. LAEMMLI, U.K. (1970). Cleavage of structural proteins during assembly of the head of the bacteriophage T4. Nature 227: 680- 685. 7. LLANOS, G. C.; D. ASCHER and D. C. BROWN (1993). Epidemic neuropathy in Cuba. Epidemiological Bulletin PAHO 14: 1-4. 8. LOPEZ-SAURA, P.; F. HERNANDEZ; V. LABARTA and the Group for the Study of the Epidemic Neuropathy (1994). Interferon alpha-2b in Epidemic Neuropathy. J. of Interferon Res. 14 (Suppl.1): S120. 9. MACKINNEY, R. E.; S. L. KATZ and C. M. WILFERT (1987). Chronic enteroviral meningoencephalitis in agammaglobulinemic patients. Rev. Infect. Dis. 9: 334-354. 10. MAS, P.; M. P. RODRIGUEZ; M. G. GUZMAN; M. ALVAREZ; V. MUZIO; O. ANCHETA; A. GOYENECHEA; H. ROCA; L. MORIER; R. ALVAREZ; M. MARRERO; A. MUSACCHIO; A. CASTILLO; V. FALCON; J. L. PELEGRINO; L. LUACES; A. BALMASEDA; M. BARRO; L. RODRIGUEZ; D. GARCIA DEL BARCO; M. SOLER; B. GARCIA; M. A. RIVAS; R. LLEONART; S. RESIK; G. PADRON; L. JOMARRON; M. CANDELARIO; M. MUNE; A. MARTIN; D. ROSARIO; M. G. MORALES; J. LAFERTE; J. REYES; C. SARIOL; R. RICARDO; J. L. MAESTRE; A. RODRIGUEZ; N. BARANOSKY; M. GONZALEZ GRIEGO; P. LOPEZ; E. PENTON; M. LIMONTA; J. DE LA FUENTE; L. HERRERA; A. LLOP and G. KOURI (1993). Resultados preliminares de laboratorio virologico en estudios de casos de Neuropatia Epidemica Cubana. Boletin Epidemiologico. Numero especial 1: 7-8. 11. MELNICK, J. L. (1990). Enteroviruses: Picornaviruses, Coxsackieviruses, Echoviruses and Newer Enteroviruses. In: Virology, Ed. by B. N. Fields et al. Raven Press, Ltd., New York. 12. MOORE, M. (1982). Enteroviral Disease in the United States, 1970-1979. Journal of Infect. Diseases 146: 103-108. 13. RAMIREZ, A.; R. RODRIGUEZ; A. MARRERO; G. MESA; M. A. GALINDO and L. INIGUEZ (1993). Neropatia Epidemica Cubana: Breve resena epidemiologica. Boletin Epidemiologico Numero especial 1: 1-5. 14. RIEGO, E.; M. MARRERO; E. CALVO; R. BRINGAS; M. ALVAREZ; M. MUNE; H. ROCA; M. GUZMAN and J. DE LA FUENTE (1994). Sequence analysis of coxsackie A9 viruses isolated during 1990-1994 in Cuba from patients with meningitis, myocarditis and epidemic neuropathy. Biotecnologia Aplicada 11: 145-150. 15. ROCA, H.; M. MARRERO; E. RIEGO; V. FALCON; P. MAS; P. RODRIGUEZ; R. ALVAREZ; V. MUZIO; B. GARCIA; R. LLEONART; G. KOURI; L. HERRERA and J. DE LA FUENTE (1994). Molecular characterization of a virus associated with the outbreak of a polyneurophathy epidemic in Cuba. Miami Short Reports 4: 89. 16. RODRIGUEZ, M. P.; R. ALVAREZ; D. GARCIA DEL BARCO; R. LLEONART; V. FALCON; J. REYES; F. O. CASTRO; J. BERLANGA; A. MUSSACHIO; P. MAS; L. HERRERA and J. DE LA FUENTE (1994). Caracterizacion de las cepas virales obtenidas a partir de aislamientos de los liquidos cefalorraquideos de pacientes con cuadros de Neuropatia Epidemica. Advances in Modern Biotechnology 2: 4.
Copyright 1995 Sociedad Iberolatinamericana de Biotecnologia Aplicada a la Salud
The following images related to this document are available:Photo images[ba95051b.jpg] [ba95051c.jpg] [ba95051a.jpg] [ba95051e.jpg] [ba95051d.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}