 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
WOUND HEALING PROMOTION IN RATS TREATED WITH EGF IS DOSE DEPENDENT Jorge Berlanga,^1 Evelio Moreira,^2 Luis C Perez,^1 Eduardo Boix,^2 Tania Gonzalez^1 and Pedro Lopez-Saura^1
^1 Centro de Ingenieria Genetica y Biotecnologia. Apartado postal
6162, Ciudad de La Habana, Cuba.
Abstract The relationship between Epidermal Growth Factor (EGF) dose and healing activity, has not been established when EGF is formulated as a semisolid cream. In order to address this question, groups of 18 experimentaly wounded Sprague Dawley rats were assigned to: A - untreated or treated with B, B - hydrophilic vehicle only, C - 0.5 ug recombinant human EGF (rh-EGF)/g; D - 5 ug rh-EGF/g and E - 10 ug rh-EGF/g of hydrophilic vehicle using a full- thickness skin wound model. After seven days, re-epithelization, percent of animals per group with re-epithelized lesions to more than 90 %, non-epithelized space between edges, and wound contraction level were assayed. The relationship between doses, inflammatory infiltrate and the fibrovascular reaction were also evaluated. Re-epithelization was significantly enhanced in groups D and E compared to A, B and C. Fourty seven percent of animals in group E showed re-epitelization of lessions to more than 90 % compared to groups A, B and C (p < 0.05). With respect to wound contraction and the amounts of non-re- epithelized space between edges, groups D and E exhibited similar responses, which were significantly improved with respect to groups A, B or C. Inflammatory infiltrate was significantly reduced in groups D and E, and showed a highest fibrovascular reaction compared to groups A, B and C. Key words: re-epithelization, wound contraction
Resumen Actualmente no se dispone de elementos experimentales, que avalen la utilizacion de determinadas dosis de Factor de Crecimiento Epidermico (EGF) en formulaciones semisolidas topicas para estimular la cicatrizacion. Para realizar esto, se utilizaron grupos de 18 ratas hembras Sprague Dawley lesionadas experimentalmente, asignadas a: A - grupo no tratado o tratado con B, B - vehiculo hidrofilo, C - 0,5 ug de EGF humano recombinante (rh-EGF)/g; D - 5 ug rh-EGF/g y E - 10 ug rh-EGF/g de vehiculo. Al septimo tratamiento, las lesiones fueron resecadas y procesadas para evaluar los siguientes aspectos: reepitelizacion, porciento de animales por grupo con lesiones epitelizadas a mas de 90 %, espacio no epitelizado y nivel de contraccion de la herida. Tambien se estudio la relacion entre dosis, la intensidad del infiltrado inflamatorio y la respuesta fibrovascular en cada grupo. La reepitelizacion fue significativamente superior en los grupos D y E comparados con los grupos A, B y C. El 47 % de los animales en el grupo E mostro mas del 90 % de reepitelizacion comparado con los grupos A, B y C (p < 0,05). Los grupos D y E mostraron respuestas similares en cuanto a contraccion de herida y espacio reepitelizado entre los bordes. La respuesta inflamatoria en los grupos D y E fue significativamente menor y se constato una respuesta fibroplastica superior a los grupos A, B y C. Palabras claves: reepitelizacion, contraccion de herida Introduction Wound healing is a localized process which involves inflammation, wound cell migration and mitosis, neovascularization and regeneration of the extracellular matrix. Recent evidence suggests that these phenomena may be regulated by peptide growth factors through autocrine and paracrine mechanisms (1). Among these growth factors, the healing promoting effect of the Epidermal Growth Factor (EGF) has been reported (2). Earlier studies demonstrated its to induce epidermal cell maturation and enhanced mitosis (3). Other evidence suggests that this molecule may act as an epidermal migration factor rather than a simple mitogen in healing wounds (4). Direct application of EGF to different wound models in vivo has shown significantly enhanced rates of epithelial regeneration and increased wound tensile strength (5). Buckley, et al. (6) were the first to report that sustained and slow release of critical concentrations of EGF into the wound site, is an important prerequisite to achieve significant increases in wound granulation tissue. They also confirmed that the number of persistently occupied receptors depends upon specific ligand concentrations, which determines the degree of mitogenic stimulation. Formulation of EGF in cream vehicles has been claimed to promote this slow release of the factor to the damaged area (2). Despite the many observations in vitro, and the evidence derived from in vivo studies, the role played by growth factors during wound repair is not clear. This is in part the result of the limited knowledge regarding the effective concentrations which promote an optimal healing response, and the difficulty for delivering these growth factors and quantifying the responses to them in vivo (6, 7). To date, the healing effect exerted by different concentrations of rh-EGF, as a topical cream formulation has not been defined. In this paper we show that re-epithelization and dermal matrix reconstitution are independent events and responsive to EGF treatment in a concentration-dependent fashion. Materials and Methods Animals Ninety female Sprague Dawley rats, (CENPALAB, Cuba) with 250 g average weight were kept in metabolic cages (IFA-CREDO 0.82 - 426) under controlled environmental conditions with free access to water and food. EGF and Formulations Recombinant human EGF was produced in Saccharomyces cerevisiae at the Center for Genetic Engineering and Biotechnology, Havana. The product was obtained with more than 95 % purity (8). It was formulated at 10, 5, and 0.5 ug EGF per gram of hydrophilic cream. EGF biological activity was assessed by a receptor-binding assay (9). Concentrations for formulation were determined by an ELISA method (10). Wound Model Nine millimeters-diameter, full-thickness skin wounds were practiced on the external side of the right upper hind limb with a skin biotome (Acu Punch, Acuderm Inc, USA.) in aseptic conditions and under sufficient anesthetic degree induced with diethilether mask. Rats were distributed among five experimental groups of 18 animals each.
Group B: treated with hydrophilic cream only Group C: treated with hydrophilic cream containing EGF at 0.5 ug/g Group D: treated with hydrophilic cream containing EGF at 5 ug/g Group E: treated with hydrophilic cream containing EGF at 10 ug/g
Sample Processing Ulcer area and a portion of surrounding tissue were excised using surgical scissors and fixed in 10 % buffered formalin. Tissue samples were paraffin-embedded and sectioned at 5 um, before hematoxilin-eosin, PAS/Alcian Blue, and van Giesson stainings.
Samples were blindly evaluated by different pathologists (Department of Pathology, Pediatric Hospital "Juan M. Marquez") using a sham identification label. Samples consisted of a 3 mm- thick slice obtained from the center of the ulcer by a sagital cut. Wound Healing Criteria
Non-epithelized space between edges (SBE) was determined by measuring the non-epithelized area between the growing edges.
Wound contraction level (WCL) was calculated as:
- Percent of epithelized area (PEA), was calculated as: PEA = [1 - (SBE)^2 / 81] x 100.
Inflammatory infiltrate was classified according to its intensity using the following criteria:
- Intense: a large amount of thicker collagen fibers in horizontal arrangement, forming a woven meshwork of fiber bundles. Positivity to van Giesson was considered.
Non-parametric statistic tests were preferred in order to avoid assumptions on the normal distribution of the data. These were processed by Mann-Whit-ney U and chi-square tests. Statistical significance was established for p ó 0.05. Results Re-epithelization (Re) Animals from group E, treated with the highest dose level of EGF (10 ug/g) exhibited a significantly enhanced rate of re-epithelization with respect to groups A (p = 0.001), B (p = 0.05) and C (p = 0.011). The effect exerted by the second dose level (group D) was similar to that seen in group E. Epithelial responses registered for group D, showed a strong tendency to be significantly higher than the value observed in group C (p = 0.054). Its enhanced re- epithelization was also noticed when compared to values recorded in groups, A (p = 0.006) and B (p = 0.043). The 0.5 ug EGF dose did not stimulate re-epithelization. The responses exhibited by this treatment group did not differ to those of groups A and B, (Figure 2).
$ Statistical difference with groups A and B (p < 0.05). $$ Statistical difference with groups A, B and C (p < 0.05).
-----------------------------------------------------------------
Table 1. Animals with more than 90 % of epithelized area,
fibrovascular reaction and inflammatory infiltrate in the
different groups: untreated (A), hydrophilic vehicle (B) and
EGF at 0.5 ug/g (C), 5 ug/g (D) or 10 ug/g (E). One biopsy sample
from groups D and E was not useful for examination.
-----------------------------------------------------------------
Group Animals with >90%
epithelization Fibrovascular reaction
---------------- ---------------------------------------
N/total % Mild Intense % intense
-----------------------------------------------------------------
A 1/18 5.6 14 4 22.2
B 2/17 11.8 13 4 23.5
C 5/17 29.4 14 3 17.6
D 7/18 41.1* 5 12 70.6*
E 8/18 47.1* 5 12 70.6*
-----------------------------------------------------------------
Table 1 (Continued)
Group Inflammatory infiltrate
-------------------------------------------------
Mild Intense % intense
-----------------------------------------------------------------
A 0 18 100
B 2 15 88.2
C 2 15 88.2
D 14 3 17.6*
E 13 4 23.5*
* significant difference with groups A and B. For details and p
values see text. *(p < 0.05).
-----------------------------------------------------------------
Non-epithelized Space Between Edges (SBE) The results indicate that treatments of groups D and E elicited a similar effect on the animals. It is noticeable that group E showed a better result solely with respect to group A (p = 0.011). However group D expressed significantly smaller values of SBE with respect to those calculated for groups A p = 0.006), B (p = 0.008) and C (p = 0.038). No differences were noticed among groups A, B and C (Figure 3).
$ Statistical difference with groups A, B and C (p < 0.05). $$ Statistical difference with group A (p < 0.05).
The WCL calculated for groups D and E did not show significant differences. The former only differed from group A (p = 0.006), whereas the latter became significantly higher with respect to values of groups A (p = 0.001) and B (p = 0.05). Group C showed a significantly higher WCL with respect to group A (p = 0.017) (Figure 4).
$ Statistical difference with group A (p < 0.05). $$ Statistical difference with groups A and B (p < 0.05).
Granulation tissue maturation score was higher for EGF treated animals with concentrations of 5 and 10 ug/g (groups D and E), while it was mild for groups A, B and C. Statistical differences appeared in groups D and E with respect to groups A, B and C (p < 0.05) (Table 1).
Inflammatory infiltrate scored in groups D and E was predominantly classified as mild, and intense for groups A, B and C. Statistical differences were observed in groups D and E with respect to groups A, B and C (p < 0.05) (Table 1).
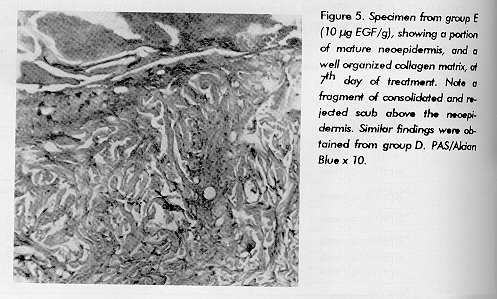
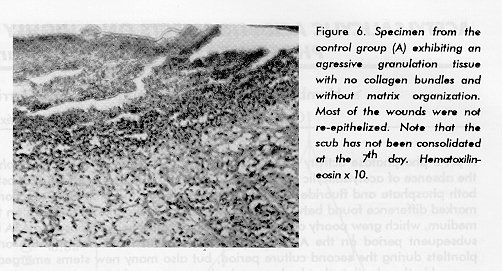
Conclusions drawn from the histological study of the specimens are consistent with the above described results. In most of the samples from groups D and E several fully resurfaced injuries were detected. These samples also exhibited an extense number of regenerated hair follicles. Another important feature was the histological presence of a marked increase in collagen deposition observed in those groups receiving higher doses of EGF (Figure 5), in comparison to control specimens from group A (Figure 6).
Figure 6. Specimen from the control group (A) exhibiting an agressive granulation tissue with no collagen bundles and without matrix organization. Most of the wounds were not re-epithelized. Note that the scub has not been consolidated at the 7th day. Hematoxilin-eosin x 10.
One of the first biological effects of EGF noticed by Cohen was the hypertrophy of the epidermis which occurred in mice after repeated injections with EGF (11). Barrandon and Green (4) suggested that EGF exerts an effect on the epidermis to speed up wound closure. Afterwards, several attempts were made to demonstrate an effect of EGF on healing skin wounds in vivo, but controversy still exists about the virtues of EGF in accelerating wound healing (12). One of the possible explanations for the ineffectiveness of EGF in in vivo trials, may be that optimal doses and application schedule have yet to be determined (7). Since wound healing is a process of overlapping biological events including inflammation and mesenchymal and epithelial cell migration, we assessed how different EGF concentrations in a topical formulation could influence on each of these processes. Re-epithelization of a wound begins within hours after injury by the migration of cells from the wound margin out across the defect (13). These cells exhibit a specific phenotype and express a large number of EGF/TGF-alpha receptors. EGF is a well-docu- mented agent in promoting epithelial-cell proliferation, keratinization and increasing the thickness of the epidermis (11). In this study, re-epithelization was significantly stimulated by EGF at concentrations of 10 and 5 ug/g, but not at 0.5 ug/g of vehicle. Although groups D and E did not show statistical difference, a trend is noticed showing an improved wound resurfacing with the highest dose level treatment. Others have also reported a dose-dependent re-epithelizing effect in the range of 100 ng-10 ug/mL, but in such experiment, a different vehicle for the formulation was used, therefore the in situ EGF bioavailability cannot be compared (14). Previous studies have shown that exogenous EGF might act, not only on the epidermal component of a cutaneous wound, but also enhancing collagen matrix synthesis and contraction which are associated to its mitogenic and chemotactic properties on normal dermal fibroblasts and for granulation tissue-derived fibroblasts (15, 16). EGF and TGF- alpha act also as angiogenic factors, stimulating blood vessel sprouting in granulation tissue (17).
Wound closure occurs from the margins of the wound and the acting contractile force derives mainly from a differentiated cell in the granulation tissue: the myofibroblast (18). As part of the dermal-mediated response, we evaluated the wound contraction level (WCL) on each experimental group. This parameter was influenced by each of the EGF treatments at 10, 5 and 0.5 ug EGF/g of vehicle. It is notorius that the largest relative response of WCL was observed in group D, and that groups E and C, were only different to A (untreated control). Previous studies have shown that EGF is capable of inducing collagen-lattice contraction in vitro (19) as well as in vivo (16). The reduction of the SBE might be due to wound contraction or to a larger epithelial outgrowth from the edges of the ulcers. Both phenomena have proved to be significantly stimulated by 5 and 10 ug/g EGF doses in this experiment. Nevertheless, it is interesting to observe that re-epithelization seemed more enhanced by the 10 ug/g dose rather than by the 5 ug/g EGF dose; the latter however, elicited a greater stimulating effect on the dermal-mediated response, such as collagenization and wound contraction. Albeit, the lowest EGF dose, did not show to exert any effect on the epidermal regeneration, it was capable of stimulating dermal contraction. This phenomenon of differential sensitivity to EGF, showed by keratinocytes and dermal fibroblasts, could be in relation to the number of constantly occupied receptors, which ultimately regulate a cellular response. In this context, dose-dependent increase in the cellularity and thickness of the neodermis has also been invoked as a mechanism of action of topical EGF formulations (20). Mustoe, et al. (21), showed that EGF concentrations higher or lower than an optimal dose may be less effective in achieving a clinically acceptable healing improvement. The environment of healing wounds is rich in growth factors, which coordinately stimulates several steps by virtue of a precisely regulated interplay among them. Experiments have demonstrated that imbalances in the concentration of one polypeptide growth factor may lead to down-regulation of critical functions of the exposed cells (14, 22, 23). In our trauma model of controlled infection, groups D and E, exhibited a better healing response and were less inflamed; whereas the other groups (A, B, C) were intensely infiltrated with round inflammatory cells. Despite that no direct effect on the wound inflammation intensity, neither on the infiltrating specific-cell stirpe, have been linked to EGF treatments (23); it is notorious that groups treated with larger doses are less inflamed. Although inflammatory cells do not express EGF-receptor (13), a modification on the local pulses of other cytokines, may arise as a consequence of the EGF topical treatment. The results presented here show that, re-epithelization, dermis reconstitution and wound contraction, are significantly stimulated by EGF- specific concentrations. On the other hand, it seemed that epidermis and dermis-mediated events exhibit particular sensitivity to a single EGF dose, which is capable of eliciting a more pronunced tissue response. Acknowledgements Authors are very grateful to Dr. Edward E. Tredget (Director of the Plastic Surgery Research Lab of the University of Alberta) for his critical advises, and to Jesus Seoane for his photographic assistance. References Referencias 1 Kovacs, JE. Fibrogenic Cytokines: The role of immune mediators in the development of scar tissue. Immunol Today 1991;12:17- 23. Schultz G, Rotatori D, Clark W. EGF and TGF alpha in wound healing and repair. J Cell Biochem 1991; 45:346-352. 2 Barrandon Y, Green H. Cell migration is essential for sustained growth of keratinocytes colonies: the roles of TGF alpha and EGF. Cell 1987; 50:1131-1137. 3 Kitazawa T, Kinoshita S, Fujita K, Araki K, Watanabe H, Ohashi Y, Manabe R. The mechanism of accelerated corneal epithelial healing by human epidermal growth factor. Invest Ophtalmol Vis Sci 1990;31:1773-1778. 4 Buckley A, Davidson M, Kamerath DC, Wolt TB, Woodward CS. Sustained release of EGF accelerates wound repair. Proc Natl Acad Sci USA 1985;82:7340-7344. 5 Okumura K, Kiyohara Y, Komada F, Iwakawa S, Hirai M, Fuwa T. Improvement of wound healing by EGF ointment. I. Effect of Nafamostat, Gabexate, or Gelatin on stabilization and efficacy of EGF. Pharmaceutical Res 1990;7:1289-1293. 6 Cinza AM, Quintana M, Lombardero J, Poutou R, Perez E, Perez.Tosar LC,. Castellanos L, Estrada R, Morales J. A batch process for production of human epidermal growth factor in yeast. Product characterization. Biotecnologia Aplicada 1991;8:166- 173. 7 Macias A, Perez R, Lage A. Estudios sobre el factor de crecimiento epidermico. II. Desarrollo de un radiorreceptor analisis para la determinacion de cantidades picomolares. Interferon y Biotecnologia 1985; 2:115-127. 8 Vazquez J, Freyre M, Duarte C, Ferra E, Lopez I, Perez E, Gavilondo J. Radio and enzyme immunoassay for Human Epidermal Growth Factor with Mouse Monoclonal Antibodies. Biotecnologia Aplicada 1990; 7:42-51. 9 Nial M, Ryan GB, O'Brien BM. The effect of Epidermal Growth Factor on wound healing in mice. J Surg Res 1982; 33:164-169. 10 Carpenter G, Cohen S. Epidermal Growth Factor. Annu Rev Biochem 1979; 8:193-216. 11 Buck RC. Cell migration in repair of mouse corneal epithelium. Invest Ophtalmol Vis Sci 1979;18:767-784. 12 Brown GL, Curstinger L, Brightwell JR, Ackerman DM, Tobin GR, Polk HC, George-Nascimento C, Valenzuela P, Schultz GS. Enhancement of epidermal regeneration by byosynthetic EGF. J Exp Med 1986;163:1319-1324. 13 Laato M, Kahari VM, Niinikoski J, Vuorio E. EGF increases collagen production in granulation tissue by stimulation of fibroblast proliferation and not by activation of procollagen genes. Biochem J 1987;247:385-388. 14 Martin P, Hopkinson-Woolley J, Mc Cluskey J. Growth factors and cutaneous wound repair. Progr in Growth Factors Res 1992;4:25-44. 15 Schreiber AB, Winkler ME, Derynk R. TGF-alpha. A more potent angiogenic factor than EGF. Science 1986; 32:1250-1253. 16 Rudolph R, Vande Berg J, Ehrlich HP. Wound contraction and scar contracture. In: Cohen IK, Diegelman RF, Lindbland WJ, eds. Wound healing. Biochemical and clinical aspects. Philadelphia: WB Saunders 1992;96-114. 17 Chen JK, Haines HB, Weiberg CB. Role of growth factors in the contraction and maintenance of collagen lattices made with arterial smooth muscle cells. J Cell Physiol 1991;146:110-116. 18 Nanney LB. Epidermal and dermal effects of EGF during wound repair. J Invest Dermatol 1990;94:624-629. 19 Mustoe TA, Pierce GF, Morshimia C, Deuel TF. Growth factor- induced acceleration of tissue repair through direct and inductive activities in a rabbit dermal ulcer model. J Clin Invest 1991;87:694-703. 20 Sporn M, Roberts AB, Shull JH, Smith MJ. Polypeptide TGF isolated from bovine sources and used for wound healing in vivo. Science 1983;219:4590-4593. 21 Heino J, Ignotz RA, Hemler ME, Crousse C, Massgue J. Regulation of cell adhesion receptors by Transforming Growth Factor-beta. J Biol Chem 1989; 264:380-388. 22 Jijon AJ, Gallup DG, Behzadian MA, Metheny WP. Assessment of EGF in the healing process of clean full-thickness skin wounds. Am J Obstet Gynecol 1989;161:1658-1662. Copyright 1996 Elfos Scientiae The following images related to this document are available:Photo images[ba96074e.jpg] [ba96074f.jpg]Line drawing images[ba96074c.gif] [ba96074b.gif] [ba96074a.gif] [ba96074d.gif] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}