 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
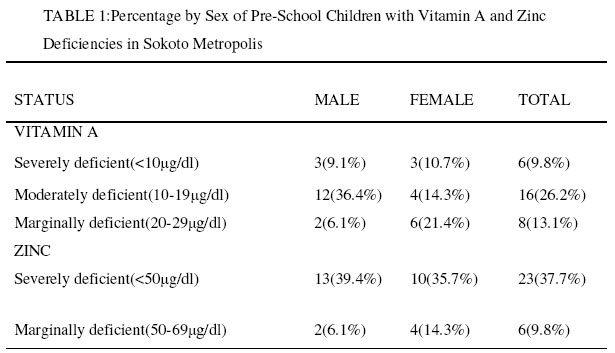
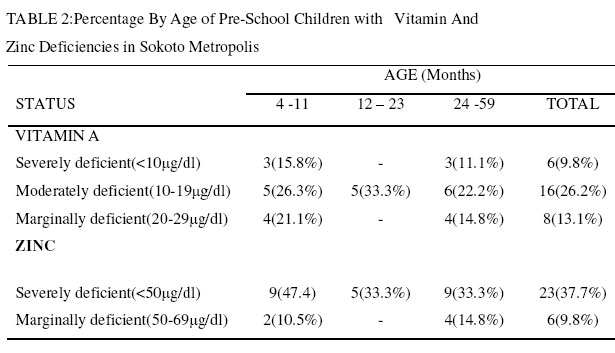
Serum Vitamin A and Zinc Levels of Some Preschool Children in Sokoto Metropolis of Nigeria L.S. Bilbis, Y. Saidu* and R.U. Aliyu Department of Biochemistry , UsmanuDanfodiyoUniversity,Sokoto, Nigeria. Received 5 September 2002 Code Number: bk03012 Abstract Serum levels of vitamin A (VA) and zinc of sixty-one randomly selected preschool children aged 4 to 60 months from Sokoto in the Northwestern Nigeria were investigated. The serum VA was assayed spectrophotometrically by ultraviolet irradiation method while Zn level was determined using atomic absorption spectrophotometer (AAS). The results obtained were analysed by correlation and regression method. The mean serum VA and Zn were 38.01 ± 18.70 and 73.24 ± 45.62 μg/dl respectively. 13% of the children had marginal VA deficiency. 26% and 9.8% of the children had moderate and severe VA deficiency (VAD) respectively. Of the 61 children studied, 37.7% had severe Zn deficiency (<50μg/dI) while 9.8% had serum Zn level of between 50 and 69 μg/dI. Analysis of the results indicated a significant (p<0.05) positive correlation(r=0.68) between serum VA and Zn levels of children with VAD. The result indicated that 66.7% of the children with VAD showed severe Zn deficiency. Only about 10% of the children with VAD were Zn adequate. The deficiencies of these micronutrients are common in both sexes and all age groups of preschool children of the study area. The results obtained indicated that the deficiencies of these micronutrients are public health problems in Sokoto, Northwestern Nigeria. Key words: Serum, Vitamin A, Zinc, preschool children, Sokoto-Nigeria INTRODUCTIONAn unsatisfactory vitamin A (VA) status is a major public health problem especially among preschool children of most developing countries of the world(1). Data from WHO micronutrients information system indicated that more than 90 countries of the world have VA deficiency (VAD) as a public health problem(2) including Nigeria (3). Worldwide, an estimated 3.1 million children have clinical VAD (2). About a million other children develop xerophthalmia annually, with 10% becoming permanently blind (4). VA is an essential nutrient, which is usually supplied in the diet as either preformed VA, carotenoid or a mixture of both (4). The recommended daily allowance (RDA) of VA for a given group depends on age and physiological status. FAO/WHO recommend that for infants and children age < 6 years, between 250 and 300 μg/day should be consumed (5). An excess amount of VA consumed above the daily requirement is stored mainly in the liver, which enables man to live for months consuming lower than his daily needs without developing clinical signs of the deficiency (4). Clinical manifestations of VAD include increased vulnerability to severe infection notably diarrhoea and measles (6) and xerophthalmia including night blindness, keratomalacia and irreversible blindness (1). Preschool children because of their rapid growth rate, typical nutritionally inadequate weaning foods and their aversion to green leafy vegetables are at higher risk of VAD(1). As the VA intake becomes poorer, the total body reserves become depleted, followed by reduction in the plasma concentration of retinol. This consequently leads to abnormalities of tissue functions (1). Effective absorption from the intestine, efficient transport and mobilization of VA from storage tissues have been documented (1). Therefore the total body reserve should be and is a good indicator of VA status of an individual (4). This may not be easy, however, to assess during a survey. Suitable and more practicable survey procedures have been developed over the years, which provide useful information on the VA status. This procedure includes those based on dietary, physiological, biochemical, cytological, and clinical assessments (1). VA status of an individual can be deficient, marginal, satisfactory, excessive or toxic. A very low plasma level of 10 μgdl-1 is associated with a deficient status, which may also be characterized by xerophthalmia. This could be as a result of deficient consumption of VA or its carotenoid precursors rich food over a span of time (1). PlasmaVA may, however, not serve as a useful indicator of VA status unless it is very low, since it is homoeostatically regulated and is subject to change as a result of other nutritional deficiencies, infections and parasitic infestations (1). It has long been established that the metabolism of micronutrients cannot be considered in isolation, since a wide range of nutritional and physiological factors can influence their uptake, transport, storage and metabolism. These interactions may enhance their susceptibility to deficiency or toxic state (4,7). In this regard, reduction in plasma VA concentration in Zn deficient animals despite diets adequate in VA has been reported (7). This may indicate a strong possible metabolic relationship between Zn and V A. This is more so, since Zn is a cofactor of alcohol dehydrogenase, which is known to reversibly dehydrogenate VA alcohol to its aldehydic form in isolated retinal rods(6). Additionally, the eye, which is an active site of VA metabolism, is one of the organs that contain the highest concentration of Zn in the body(7). More recently the role of Zn in the VA metabolites nuclear receptors have been established (8). It is also thought to be important in the synthesis of retinol binding protein (RBP) by the liver (7). Since it appeared that there is a dearth of reports on micronutrients status of preschool children in this part of the world, we report serum VA and Zn status in preschool children in Sokoto metropolis, Nigeria. MATERIALS AND METHODS Human Subjects: A total of 61 apparently healthy children, aged 4-60 months, who were on routine immunization visits to some selected hospitals within the metropolis were randomly selected for this work. The hospitals and clinics selected were: 1. UsmanuDanfodiyoUniversity Teaching Hospital, Sokoto. Blood Samples: Blood samples collected by venipunctures were carefully transferred into cleaned, dried, labelled and corked centrifuge tubes and immediately transported to the laboratory in a cold box for analysis. Serum was separated from blood sample by centrifuging at 3000rpm for 5min in a bench top centrifuge. The sera obtained were transferred into labelled, corked, aluminium foil screened plastic tubes of 1ml capacity and stored immediately at –20oC until required(9). Purposely to reduce the possible destruction of vitamin A and the associated erroneous results that will be obtained as a result of haemolysis and exposure to light(9).The samples were analysed for both VA and Zn within 72 hours of collection. Reagents and Equipment: All the reagents used in this work were of analytical-grade and were purchased from Sigma Chem. Co. USA. USP reference VA standard capsules used, were obtained from Accucaps Industries Limited, Canada. UV/visible spectrophotometer (Pharmacia LKB Biochrom 4060 model) was used for the analysis of VA. Zn estimation was carried out using atomic absorption spectrophotometer (AAS) (Buck Scientific model 210). Assay Method: VA was assayed by ultraviolet inactivation as reported by IVACG 8. Serum samples for Zn estimation were deproteinised using 10% (v/v) solution of 70% perchloric acid in distilled water. The sample was then centrifuged at 700g for 10 minutes. The absorbance of the clear supernatant was read from AAS using a Zn lamp. Acetylene – oxygen gas was used. The concentration of Zn in the samples was extrapolated from a standard curve constructed using ZnSO4 solution as the standard. The results obtained were analysed using correlation and regression. RESULTS AND DISCUSSIONThe mean serum VA and Zn levels of 61 preschool children aged 4 to 60 months in Sokoto Metropolis of northwestern Nigeria were 38.01+187μg/dl and 73.24+46.62μg/dl respectively (Not shown in the tables. Out of the 61 children recruited for this work,49.2% (table 1) had VA levels of less than 30 μg/dl (1.05 mol/L), the lowest acceptable level for young children (1). Hernando(10) reported a normal frequency distribution curve of serum VA levels in children, aged 2-6 years old, of deprived environments who were previously placed on a massive dose of VA with about 95% of the values greater than 30μg/dl. In the current work 13.1% of the children had marginal VA status (20-29μg/dl) while up to 9.8% of the children were severely deficient (<10 μg/dl)(1). Analysis of the results on the basis of gender indicated that 9.1% and 10.7% of the male and female children respectively had severe VAD (Table 1). Up to15.8% of the children aged 4-11 months had severe VAD with another 26.3% showing moderate deficiency (Table 2). The incidence of vitamin A deficiency in the current study is higher, compared to that reported (49.1% versus16.5%) in an earlier survey confined to Niger and Kaduna states of Northwestern Nigeria(11). Survey results from other geopolitical zones of Nigeria indicated lower incidence of VAD compared to the North West Zone (11) . As reported by other researchers(3,12), our report confirmed the fact that, hypovitaminosis A is a public health problem in many developing countries of the world including Nigeria. The most basic cause of VAD in this part of the world is a habitual intake of too little VA in relation to need(1) asa result of poverty and/or ignorance. Disease like diarrhoea is another risk factor of VAD in children(6). However, other factors like Zn status may significantly affect the VA status of individuals. The result of the current study indicates that about 48% of the children had low (<70μg/dl) serum Zn concentration. Up to about 39% and 36% of the male and female children respectively showed severe Zn deficiency (Table 1). About 47% of the under one children had severe Zn deficiency (Table 2). These children are being weaned on cereal gruels, which may be poor sources of these micronutrients The result indicated a significant (p< 0.05) positive correlation(r=0.68) between serum VA and Zn levels of children with VAD. In the current work, all the children with severe VAD also had severe deficiency of Zn. About 66.7% of children with VAD had Zn level of less than 50μg/dl (Table3). The association between the two is interesting. Significant correlation of Zn and VA deficiencies in children had been reported (7,13,14). It has also been reported that plasma VA increases as a result of Zn administration in rats(7). These observations underscore the importance of Zn in VA metabolism. Zn is an integral component and an important cofactor in the function of VA nuclear receptors(7). It is also important in the synthesis of retinol binding protein(7), and a component of more than 70 enzymes including DNA and RNA polymerases(15). Micronutrients deficiencies especially VA and Zn in children in the population have far reaching health and socio-economic implications. Chances of developing eyes related diseases including night blindness are increased. Some studies have indicated that preschool children enduring inadequate intake of VA and to a lesser degree, Zn are associated with stunted growth, less weight gain, lower than normal levels of haemoglobin concentrations, higher incidences of diarrhoea and measles, and erythrocyte abnormalities (6,13). All these tend to suggest that children with VA and Zn deficiencies are less likely to realize their full potential for growth and development and are more susceptible to diseases especially when they occur together. It could be concluded that VA and Zn deficiencies are significant public health problems in the study area, that demand the urgent attention of the government and non governmental organizations. Intervention methods through dietary supplementation or fortification need to be instituted and sustained. ACKNOWLEDGEMENTThe first and second authors wish to express their appreciation to the UsmanuDanfodiyoUniversity, Sokoto, Research and Publication Committee for providing them with the research grant used for this work. REFERENCES 16. IVACG (1993) A brief guide to current methods of assessing vitamin A status (B.A. Underwood and J.A. Olson eds). A report of the International Vitamin A Consultative Group (IVACG), Washington USA, 1-26. 17. Underwood, B.A. and McClatchey S. (1994) Global prevalence of vitamin A deficiency and its control. In: Report of the XVI IVACG Meeting: Two decades of progress, linking knowledge to action Chiang Rai, Thailand; 64. 18. Atinmo, T., Adeyemo A.A., Adeyefa I., Omatade O.O., Ajaiyeoba O., Olubajo O., Obagaiye O., and Salami L. (1997) The vitamin A status of Nigerian children: Prevalence and risk factors from the National Micronutrients Survey 1993. In the report of the XVIII IVACG Meeting Cairo, Egypt, 22-26. 19. Bauernfeind, J.C. (1980) The safe use of vitamin A; a report of IVACG; Nutrition Foundation; Washington; USA, 1-12. 20. FAO/WHO (1967) Requirement of Vitamin A, Thiamine, Riboflavin and Niacin, Report of a joint FAO/WHO Expert Group. World Health Organisation Technical Report series 362. FAO Nutrition Meeting Report Series 41. FAO, RomeItaly. 21. IVACG (1996) International Vitamin A Consultative Group (IVACG) policy statement on vitamin A, diarrhoea and measles; Washington, USA. 1 - 4 22. Smith, J.C. (1980) The vitamin A - zinc connection: A review. Annals of New YorkAcademy of Sciences: 62-75. 23. Blumhoff, R. (1997). Molecular mechanisms of vitamin A; In a report of the XVIII IVACG Meeting: sustainable control of vitamin A deficiency; CairoEgypt; 47-48. 24.IVACG (1982). Biochemical methodology for the assessment of vitamin A status; Nutrition Foundation, Washington, USA, 4-30. 25. Hernando, F. (1993); Frequency distribution of serum vitamin A levels in cross Sectional surveys and in surveys before and after vitamin A supplementation; In a brief guide to current methods of assessing vitamin A status: A report of IVACG; Nutrition foundation; Washington; USA; 9-11 26. FGN/UNICEF (1994) The Nutritional Status of Women and Children in Nigeria; Lagos; Nigeria.; Quoted in Curriculum for Institution Based Short-Term Nutrition Training in Nigeria For Field Programme Managers and Implementors; Food Basket Foundation International; Ibadan Nigeria: 13 27. Atinmo, T. (1994) Nigerian National Micronutrients Team, Magnitude and distribution of vitamin A deficiency in Nigeria; In the report of the XVI IVACG meeting: Two decades of progress; Linking knowledge to action; Chiang Rai, Thailand, 82. 28. Smith, J.C.; Makdani, D., Hagar, A., Rao, D. and Douglas L.W. (1999) Vitamin A and zinc supplementation of preschool children; Journal of American College of Nutrition; 18: 213-222. 29. Yuyama, L.K.O. and Cozzolino, S.M. F.(1999), Interaction of vitamin A and zinc in lactating rats: Experimental deficiency models, Archivos Latino Americanos De Nutrition; 45: 305-309. 30.Peggy, L.P. (1997). Nutrition in infancy and childhood; C.V. Mosby Company, USA. ; 40-76. © 2003 Nigerian Society for Experimental Biology. The following images related to this document are available:Photo images[bk03012t2.jpg] [bk03012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}