 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
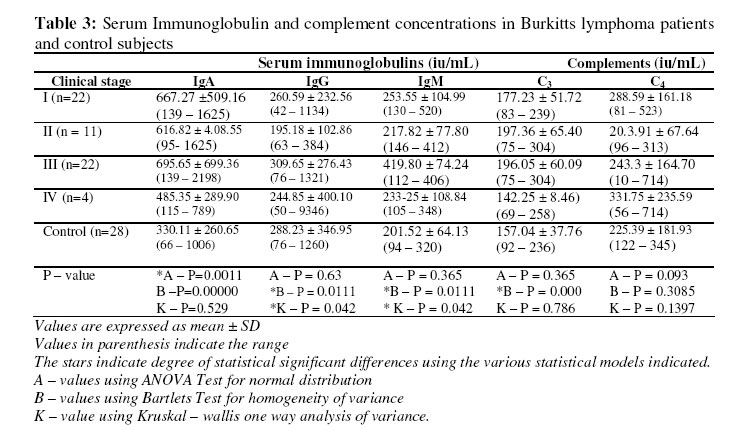
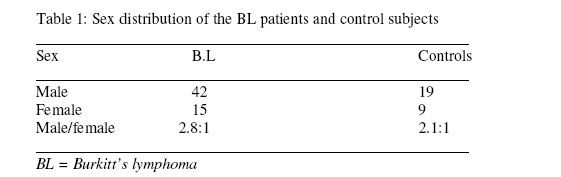
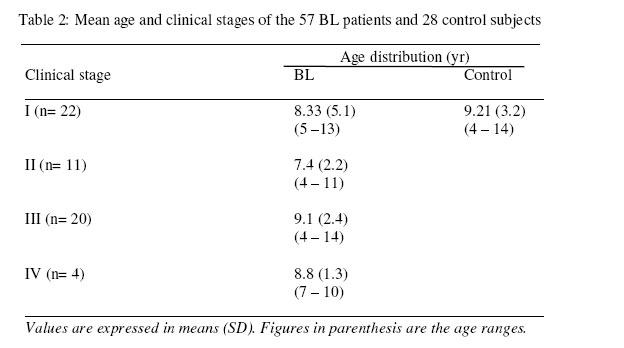
Biokemistri, Vol. 17, No. 2, Dec, 2005, pp. 193-197 Antibody and complement levels in patients with Burkitt’s lymphoma Godwin UMUKORO*a and Innocent ONYESOMb Departments of aMedical
Microbiology and bMedical Biochemistry, Faculty of Basic Medical
Sciences, College of Health Sciences, Delta State University, Abraka, Nigeria Received 6 August 2005 Code Number: bk05027 Abstract The concentration of immunoglobulins (IgA, IgG, and IgM) and complement (C3 and C4) were measured in fifty-seven (57) Nigerian children with Burkitt’s lymphoma (BL), and in twenty-eight (28) apparently healthy control subjects, using the single radial immunodiffusion (SRID) technique. The sera analyzed were obtained from the four clinical stages of BL. There were high titres of IgA (stage I: n=22; 667.27 ± 509.16; stage II:n=11; 616.82 ± 408.55; stage III: n=20; 695.65 ± 699.93 and stage IV: n=4, 485.75 ± 289.90); IgG (stage I: n=22, 260.59 ± 232.56; stage II:n=11 195.18 ± 102.86;stage III:n=20, 309.65 ± 276.43; stage IV:n=4, 244.85 ± 400.107). IgM (stage I:n=22, 253.55 ± 104.99, stage:II n=11, 217.82 ± 77.8; stage III:n=20, 419.20 ± 74.21, stage IV:n=4, 233.35 ± 108.84). These values are significantly higher (P<0.05) than the values for the control subjects (IgA, 330.11±260.55; IgG, 288.29 ± 346.95, IgM, 201.82 ± 64.132). Higher complement titres were also observed in the various clinical stages of BL C3 (stage:In=22, 177.25 ± 5172; stage II:n=11, 197.36 ± 65.40; stage III:n=20, 190.05 ± 60.91; stage IV:n = 4, 142.25 ± 81.40); C4 (stage I:n=22,288.68 ± 181.84, stage II:n=11, 207.91 ± 67.64; stage III:n=20,243.30 ± 164.70, stage IV:n=4, 331.75 ± 275.59). The complement values for control subjects were significantly lower than the BL patients; (C3:157.04± 37.76; C4 256.39 ± 181.93). These results show relative higher immnoglobulins and complement responses in Nigerian children with BL. Key words: Immunoglobulin, Burkitt’s lymphoma, Nigeria INTRODUCTION The etiology of Burkitt’s lymphoma (BL) has been reported by several authors 1,2,3,4. One of Burkitt’s early papers discussed the potential role of host immunity to BL. He reported cases of spontaneous remission, and those who transiently responded to serotherapy with sera from BL patients who had undergone complete remission5. Other investigators who pursued this initial documented idea observed evidence of serum cytotoxicity in-vitro. The development of hypersensitivity reactions to extracts of autologous tumour and impaired immune reactions associated with the presence of large tumours further support the potential role of immune failure in the pathogenesis of BL.6,7,8. Clinical trials of immunotherapy were started in the early 1970’s based on Burkitt’s hypothesis of immunosurveilance using sera from patients who had undergone complete tumour regression, and immunostimulators like Bacillus Calmette Guerin (BCG)9. Depressed host immunity measured by mitogen stimulation and delayed type hypersentivity in BL patients bear direct and indirect relationship to the tumour burden10,11. The immunology of BL is further complicated by the presence of Epstein Barr viral particles in the tumour cells which express a variety of virally determined antigens that provoke complementary antibody and cellular responses4. In addition, as a B-lymphocyte tumour, the cells may be subjected to immunoregulatory influences such as T-helper cells or T-suppressor cells and antidiotype antibody responses. The aim of this work is to measure the concentration of serum immunoglobulins IgA, IgG, IgM and complements (C3, C4), in the various clinical stages of BL, and to determine their relevance in BL pathogenesis in Nigerian children with BL. MATERIALS AND METHODS Patients’ Selection Fifty-seven (57) Burkitt’s lymphoma patients (4-14yrs)of age attending Paediatric clinic of Ahmadu Bello University Teaching Hospital (ABUTH) Zaria and Kaduna, Nigeria, between 1994 and 1996, were enlisted for the study. These cases were diagnosed clinically and histopathologically using the established WHO criteria12. Human experimentation conduct protocol was approved by the ABU-Hospital Ethical Committee (Ref. No. F-MED/com.19/16/6/95 and the project number was ESC/95/00075). Quantitation of serum Immunoglobulin and complement The single radial immunodiffusion technique13 was used. Serial dilution (nondil; 1:2, 1: 4, and 1:8) of standard serum (WHO recommended) were used to obtain a standard calibration curve. Samples were then assayed, and the immunoglobulin and complements were estimated using the calibration curve. Commercial test kits supplied by Sigma, Chemicals, United Kingdom were used for the assays. Statistical Analysis The data collected were subjected to statistical analysis using the E.P.I computer package. The various levels of significant differences were computed using analysis of variance (ANOVA), Bartlet test of homogeneity and Kruskal-Wallis one-way analysis of variance. RESULTS There was significant increase (P<0.05) in the concentration of IgA in all the clinical stages of BL when compared with control subjects. Table 3 shows significant different in AP, P<0.005. A relatively higher IgG titre is seen in Table 3 with significant difference in BP and KP with P<0.005. IgM has significantly higher titre in all the clinical stages when compared with the titres for the control subject. Table 3, also shows significant difference in BP and KP (P<0.05). The various concentrations of the serum complement (C3 and C4) in all the clinical stages were not significantly higher than the levels in the control subjects. Relative comparison of the various immunoglobulin show that IgA has the highest titre and the class III clinical stage had the highest concentration. DISCUSSION The central role of antibody mediated immune response in BL has not been clearly documented. Early studies using cultured cell-lines from BL biopsy were able to recognize, some BL specific antibodies like the cardio antigens and their specific antibodies (VCA), membrane antigens (MA) with their specific antibodies, and predictions were made based on these findings14,8. The presence of these antibodies in very high titres have been of prognostic importance;14,15. This in-vitro finding using human sera has been able to demonstrate a significantly high immunoglobulin response in BL patients which correlate with disease activity. For example, the highest concentration of IgA was noticed among patient with tumour in multiple sites (Table 3). This observation tends to agree with earlier suggestions14,15. This study shows that in BL patients the major Immunoglobulin response was IgA followed by IgM and IgG. Table 3, also shows significantly high level of the complement components, C3 and C4; C3 levels from stage I to III were relatively higher than control group and C4 levels from stage I to IV were all higher than control group but not to a statistically significant level (P>0.05). The actual role played by these high concentration of antibodies and complement components could be suggestive (from some clinical observations) of the tumour site. Clinically, the oral tumours are oedematous and bleed easily, indications of inflammatory activities, which may be due to complement activation. Usually the oral hygiene were poor with dental anarchy and offensive odour. These are suggestive of the role played by high complement (C3 and C4) titres in BL. High level of 1gA, IgM and IgG have also been reported in some tropical diseases like malaria, and in HIV infected patients 16,17. In these cases, it was observed that there was hypergammaglobulinaemia in Nigerian patients with HIV 17 and IgG subclass levels in malaria infected Nigerian16. Previously, the etiological correlation between malaria infestation and BL has been established, and hypergammaglobulinaemic condition may induce suppressions including immune suppression that might result in BL3. REFERENCES
The following images related to this document are available:Photo images[bk05027t2.jpg] [bk05027t3.jpg] [bk05027t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}