 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Biokemistri, Vol. 19, No. 1, June, 2007, pp. 29-34 Plasma vitamins C and E levels inversely correlate with the risk of ischaemic heart diseases in patients from Imo state, Nigeria Okey A. OJIAKO1* and Harrison U.NWANJO2 1Department
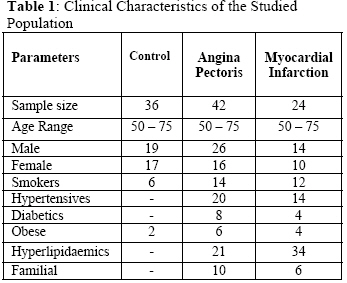
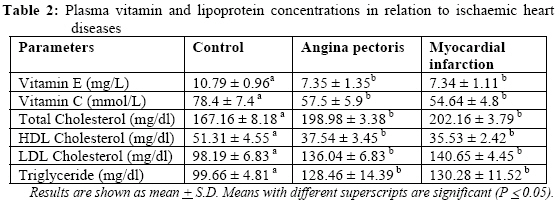
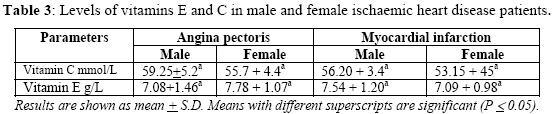
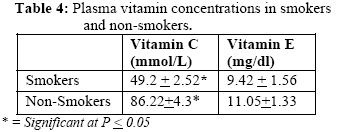
of Biochemistry, Federal University of Technology, Owerri, Nigeria Received 13 March 2007 Code Number: bk07005 Abstract Sixty-six Nigerian patients with ischaemic heart diseases age ranging between 50 -75 years were studied. The samples consisted of 42 cases with angina pectoris and 24 cases with myocardial infarction, which were proven to suffer from ischaemic heart disease by the presence of clinical symptoms, exercise electrocardiogram abnormalities and myocardial enzyme measurement. Controls were 36 subjects who did not show any abnormalities in the parameters used. Controls and patients were classified into groups based on the presence or absence of risk factors (smoking, hypertension, diabetes, hyperlipidaemia, obesity and family history). The mean plasma concentrations of vitamins C and E were significantly inversely related to the risks of ischaemic heart disease. Smoking was a compounding factor. These findings suggest that some populations with high incidence of ischaemic heart disease may benefit from eating diets rich in natural antioxidants, particularly vitamins E and C. Keywords:Vitamins C and E, ischaemic heart disease, angina pectoris, myocardial infarction INTRODUCTION Free radicals have been incriminated in the pathogenesis of myocardial damage during ischaemia as well as in the generation of atherosclerotic plaques. In both processes, membrane damage has been considered to play a pivotal role in initiating the cascade process leading to the ultimate cellular death of the affected tissues. A large body of evidence1 shows that free radicals are responsible for plasma membrane damage and that it is the fallouts of these peroxidation processes that eventuate in the diverse sequelae of various diseases like obesity, diabetes mellitus, arterial hypertension and other cardiovascular diseases, retinopathy, nephropathy etc2,3. In addition to lipids, free radicals attack proteins, enzymes and DNA to unleash an avalanche of pathological events4. The oxidative modification of low-density lipoprotein (LDL) particles in the arterial subendothelium results in structural changes, which are postulated to make them more atherogenic than native LDL. This then means that inhibition of oxidation or modification of LDL should retard or inhibit atherosclerosis and consequently decrease or prevent the clinical sequelae. This is why the use of dietary antioxidants to inhibit the oxidation or modification of LDL has received increasing attention in recent years and has in consequence popularized the use of antioxidant food supplements to improve life expectancy. The nutrients that have shown promise as protective antioxidants include lipid - soluble antioxidants in humans because of their association with membrane lipids as well as water-soluble vitamins like Vitamin C. Vitamin C serves directly as an antioxidant by scavenging aqueous peroxyl radicals and indirectly by regenerating reduced vitamin E. Vitamins C and E as well as uric acid, ubiquinol and β-carotene (among others) are chain-breaking antioxidants and could individually halt the chain of oxidative reactions that ultimately lead to pathology4. The use of these vitamins combined with moderate exercise have been shown to counteract oxidative stress and also lower the level of malondialdehyde, a critical marker of oxidative stress 3,5. Since these vitamins and other antioxidants are available in several food materials in our environment and the highest prevalence of cardiovascular disease risk factors is observed in adults of low socio-economic status6, the nutritional and health benefits of the current study to a predominantly poor population justify the effort. It is therefore, the purpose of this work to obtain an evidence from Imo State, Nigeria that low plasma concentrations of vitamins with antioxidant properties is related to the risk of ischaemic heart disease and then suggest the clinical significance of eating diets rich in natural antioxidants, the so-called functional foods, to this population. This is important especially as reports from different parts of the world seem to be contradictory7,8. MATERIALS AND METHODS Identification and Grouping of Subjects Successive patients presenting to General Hospital, Owerri and a reputable specialist private hospital in Owerri Nigeria between a period of eight (8) months were enlisted for the study. Sixty-six (66) newly diagnosed patients with ischaemic heart disease (32 males and 34 females) age ranging 50-75 years and 36 population-based controls (19 males and 17 females) of the same age brackets were used for this study. The samples consisted of 42 cases with angina pectoris, and 24 cases with myocardial infarction, which were proven to suffer from ischaemic heart disease by the presence of clinical symptoms, exercise electrocardiogram abnormalities and increased blood levels of myocardial enzyme (lactate dehydrogenase isoenzymes; LDH1 and LDH2). Controls were subjects who did not show any clinical evidence of ischaemic heart disease, and no E.C.G changes. The subjects were divided into groups based on various risk factors as follows: Smokers: Subjects who smoke regularly and at least one cigarette per day or its equivalent as tobacco or has just stopped smoking in the last three months prior to the study. Hypertensives: Subjects that had raised blood pressures interpreted as patients with an average of 2 diastolic BP measurements in the range of 95-130 mmHg in the sitting or supine positions. Diabetics: Subjects that had raised blood sugar levels and were placed on diet. Obese: Subjects that had body mass index (BMI) ≥ 30, BMI calculated as weight/height x height. Hyperlipidaemics: Subjects with LDL cholesterol levels > 140 mg/100ml or total cholesterol level > 200mg/100ml. Familial: Subjects with positive family history of one or both parents or bloodkin having had ischaemic heart disease or died suddenly before the age of 55. Individuals with abnormal liver and kidney function parameters or those with peripheral blood vessel disorders and acute infections were categorized as confounders and therefore excluded from the study9. All subjects were informed of the rationale for the study and their informed obtained prior to the study as required by WHO10. Blood Collection and Biochemical Assays Blood samples (5ml each) from the subjects were collected into tubes treated with the anticoagulant EDTA (1mg/dl) after an overnight fast of 10-12hrs. Blood was obtained from patients with acute myocardial infarction within 9-24 hrs after attack. Blood samples from healthy subjects who had normal cardiovascular function and were resident in Owerri metropolis were similarly collected and used as controls. The plasma samples obtained by centrifuging the whole blood in a Wisperfuge (model 684) centrifuge at 2500g for 10 min were used immediately11. Plasma vitamin C was assayed by the 2 – 4 nitrophenyl-hydrazine methods of Tietz 12 while plasma Vitamin E levels were determined based on the ability of vitamin E to cause a reduction of ferric to ferrous ion which them forms a red complex with α-α-dipyridyl as described by Tietz13. Plasma triglyceride level for each sample was determined by the method of Mendez et al14. Total cholesterol was measured by the method of Zak15 while high-density lipoprotein – cholesterol (HDL-C) was determined by the method of Lopez-Vitrella et al16. Low density lipoprotein – cholesterol (LDL-C) was then calculated by a modified Friedewald formula17 based on these measured parameters. Percentage plasma lactate dehydrogenase isoenzyme activity was determined using the polyacrylamide gel electrophoresis method of Ditz and Lubrano18. Statistical Analysis All results were analyzed by the Statistical Analysis System (SAS) program (SAS Institute, Inc. Cary, N. C.) and values were expressed as mean ± S.D. Duncan multiple range test was used to determine significant differences in the plasma concentrations of vitamins C and E, and the lipoproteins. Correlation was done using Spearman’s correlation statistical method. Results with differences at P ≤0.05 were considered significantly different. RESULTS AND DISCUSSION The clinical characteristics of the studied population are shown in Table 1. Levels of Vitamins C and E in the samples as well as the results of lipoprotein determinations are represented in Table 2. These results show that the mean plasma concentrations of vitamins C and E in angina pectoris patients were 57.5 ± 5.9 mmol/L and 7.35 ± 1.35mg/L respectively while the corresponding values in patients with myocardial infarction were 54.64 ±4.8mmol/L and 7.34 ±1.11mg/L respectively. These values are significantly (P< 0.05) lower than the control group values of 78.4 ± 7.9mmol/L and 10.79 ± 0.96mg/L for vitamin C and E respectively. There were no statistically significant gender-related differences between male and female patients with angina pectoris as well as between those with myocardial infarction is as shown in Table 3. The results of the lipid profile showed significantly (P ≤ 0.05) higher levels of total cholesterol, LDL – cholesterol and triglyceride in both angina pectoris and myocardial infarction patients relative to the corresponding values for the control group. Contrarily, the HDL – cholesterol levels in these disease conditions were significantly (P ≤ 0.05) lower than the value for the control group. These observations agree with our results in an earlier study on this population9. The findings are also in consonance with some other reports for Nigerians19 as well as for the report for Indians20. Table 4 shows the relative results of these measured parameters between smokers and non-smokers. Cigarette smokers had significantly (P ≤ 0.05) lower levels of vitamin C than subjects who had never smoked. There was however, no observed significant difference in vitamin E levels between smokers and non-smokers among the studied population. These observations do not agree completely with other reports. Cigarette smoke as well as various gaseous pollutants are known to induce oxidative stress which in turn depletes the levels of antioxidants including vitamins A, C and E. The non-significant increase in Vitamin E level observed in this study may be as a result of several factors. In addition to scavenging reactive oxygen and reactive nitrogen species, vitamin C is known to possess the ability to regenerate other antioxidants such as a-tocopherol (vitamin E), glutathione, urate and B-carotene from their respective radical species1. Vitamin C may therefore have had a regenerating or sparing effect on vitamin E, hence our current observations. This however needs to be further investigated. Furthermore, correlation analysis (not shown in the tables) show that plasma vitamin E concentrations were inversely related to total cholesterol (r = - 0.51; P < 0.05) and to triglycerides (r = - 0.45; P < 0.05) but positively related to HDL cholesterol (r = 0.47; P < 0.05). Similarly, plasma vitamin C concentrations were inversely related to total cholesterol (r = - 0.46; P < 0.05) but not to HDL-Cholesterol. Low levels of HDL-Cholesterol and high levels of triglycerides, total cholesterol and LDL-Cholesterol are known to be independent markers of the possibility of cardiovascular events22. Our findings therefore support this position. The relevance of our study on the possible correlation between vitamins C and E and ischaemic heart diseases in our locality is heightened when considered against the background that the evidence from laboratory and epidemiological studies linking low plasma vitamin antioxidants with ischaemic heart diseases (IHD) has been equivocal. In Europe, the study of healthy middle-aged men in Scotland, Finland and Italy showed no consistent correlation between plasma concentrations of carotene or vitamins A, C and E and the incidence of IHD among the population7. In Netherlands, a multicentre case-control study on alpha-tocopherol and beta-carotene concentrations in coronary heart diseases (CHD) showed that low alpha-tocopherol concentration was not associated with the risk of myocardial infarction8. These findings mean that vitamin levels can not explain the incidence of coronary heart disease among these studied populations. Other studies23 have however shown a clear inverse relationship between plasma vitamins C and E concentrations and CHD. In India, it was shown that the inverse relation between CAD and low plasma vitamin C concentration was substantially reduced after adjustment for smoking and diabetes while Vitamin E level remained independently and inversely related to the risk of IHD after adjustment for age, smoking, and diabetes. Having established that the levels of the antioxidant vitamins C and E inversely correlate with ischaemic heart diseases in our study area of Imo State, Nigeria and considering that due to a concert of socio-economic factors apparently healthy people may not seek medical attention until the late stage of ischaemic pathology, we recommend that serum levels of vitamins C and E among the population be used as a preliminary tool for diagnosing and managing ischaemic heart diseases in this area. REFERENCES
The following images related to this document are available:Photo images[bk07005t3.jpg] [bk07005t4.jpg] [bk07005t2.jpg] [bk07005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}