 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
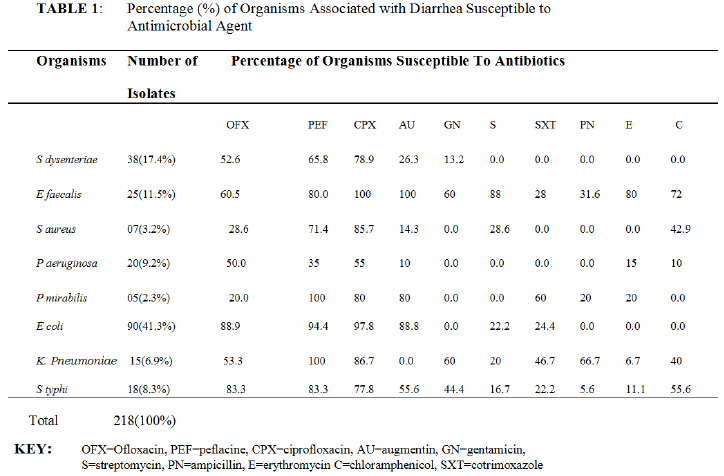
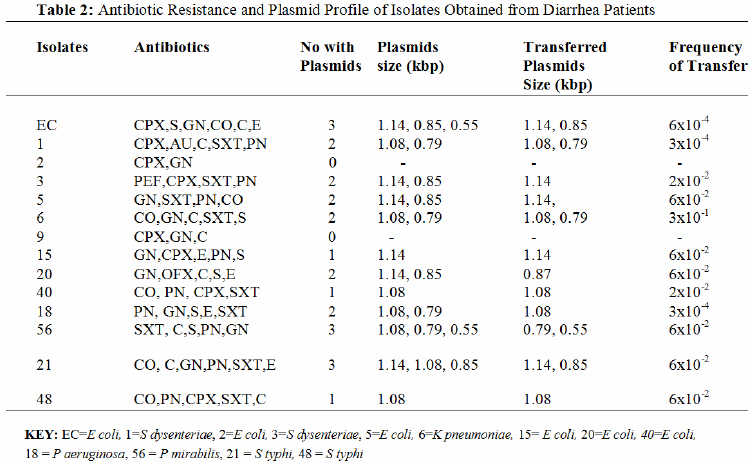
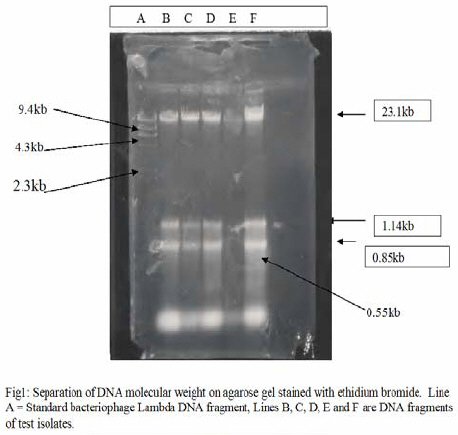
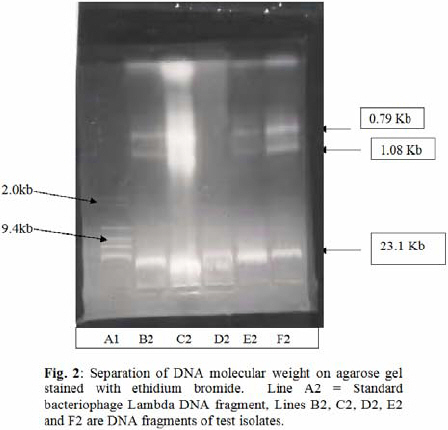
Biokemistri, Vol. 19, No. 1, June, 2007, pp. 35-42 Multi-antibiotics-resistance plasmid profile of enteric pathogens in pediatric patients from Nigeria Clarence Suh Yah1*, Helen U. Chineye2 and Nosakhare Odeh Eghafona1 1Department of Microbiology, Faculty of Life Sciences, University of Benin, Benin City, Nigeria Received 26 January 2007 Code Number: bk07006 Abstract A total of 938 faecal samples of diarrheal stool of pediatric patients attending Madonna University Teaching Hospital (MUTH) from June 2003 to June 2004 were examined. 218 of eight different bacterial strains namely Escherichia coli 90(41.3%), Shigella dysenteriae 38(17.4%), Pseudomonas aeruginosa 20(9.2%), Salmonella typhi 18(8.3%), Staphylococcus aureus 7(3.2%), Proteus mirabilis 5(2.3%), Enterococcus faecalis 25(11.5%) and Klebsiella pneumoniae 15(6.9%) were isolated. The susceptibility pattern of the isolates to the various antibiotics varied with Proteus mirabilis and Klebsiella pneumoniae 100% sensitive to peflacine and Enterococcus faecalis 100% sensitive to ciprofloxacin and augmentin.Most of the isolates were least sensitive tocotrimoxazole, ampicillin, erythromycin gentamicin, streptomycin and chloramphenicol. The resistance plasmids to the various isolates were very diverse and distributive among the isolates. They were also highly transferable with a high frequency range of 2x10-2 to 6x10-4. Some of the isolates had plasmids bands that ranged from ≤0.55kbp to ≥1.14kbp. This indicates that plasmids allow the movement of genetic materials, including antimicrobial resistance genes between bacterial species and strains. Keywords:Diarrheagenic pathogens, antibiotics resistance plasmids profile INTRODUCTION Intestinal diseases of microbial origin are marked principally by diarrhea and sometimes by ulcero-inflammatory changes in the small or large intestine13. It is usually a symptom of gastroenteritis and can be accompanied by severe abdominal pain, urgency, perianal discomfort, and incontinence13. Diarrhea posses a very serious problem in developing countries where it is the leading cause of morbidity and mortality among children and adult. It ranks second only to respiratory diseases and is a major cause of morbidity among notifiable diseases in some part of the world4. An estimate of about 5 million children (more than 13,600 a day) dies from diarrheal diseases in Asia, Africa and South America. In the U.S, estimates exceed 10,000 deaths per year from diarrhea and an average of 500 childhood deaths are reported per day22. Epidemiological studies have also shown that diarrhea is responsible for more than 3.1 million deaths each year among children less than 15 years of age, mostly in developing countries10. It is estimated that U.S adults each year experience 99 million episodes of acute diarrhea. Although mortality due to acute diarrhea in children has decreased both in developed and developing countries in recent years after the introduction of oral dehydration solution. Those associated with persistent diarrhea occur in malnourished children and is usually disproportionately high, accounting for up to 45% of diarrhea deaths in Brazil, Bangladesh and in several African countries9,22. In Nigeria, the incidence of acute watery diarrhea is approximately 4.9 episodes per year and there are approximately 200,000 diarrhea related deaths of children aged below five years with an average of 300 deaths per day8,10. Ogunsanya et al.19 found that 70-90% of children in Lagos from December 1989 to May 1990 were infected with enteropathogenic bacteria as compare to 28% of control group. According to Federal Ministry of Health,8 the risk factors include malnutrition, poor personal hygiene, unhygienic food preparation, improper sewage disposal, environmental sanitation problems, inadequate water supply, over crowding. Also, people who visit foreign countries are at risk for traveler’s diarrhea, caused by eating food or drinking water contaminated with bacteria, viruses or sometimes parasites7,25. Antimicrobial resistance on enteric pathogen is of great public health concerned in the developing world where the rate of diarrhea is highest. Researchers have also reported an increasingly widespread use of antibiotics in food and animals contributing to high dissemination of resistant enteric infections to humans. Most of these life-threatening enteric pathogens include Escherichia coli, Salmonella, Shigella, Yersinia, Vibrio, Campylobacter species Entamoeba histolytica, andGiardia lamblia in developing countries6,5,22. In the 1960’s Salmonella species resistant to ampicillin, chloramphenicol and trimethoprim – sulfamathoxazole have been reported with increasing frequency through out the world. Strains of Campylobacter jejuni have been reported as resistant to ampicillin, carbenicillin, clindomycin, gentamicin streptomycin and metronidazole24,26. The present study was aimed at assessing the level of antibiotic resistance from diarrheal stool of pediatric children age less than 5 years attending Madonna University Teaching Hospital (MUTH) Elele, River State, Nigeria and also to determine the plasmids transferability of the antibiotic resistance markers among the enteric bacteria population. Plasmids have been found to confer drug resistance to their host bacteria14,27. Other studies have shown that they can be transfer from one bacterium to another by conjugation, transformation and by phage – mediated transudation17,22,29,33. MATERIAL AND METHODS Samples were collected from 938 diarrheal stools of pediatric patients attending Madonna University Teaching Hospital (MUTH) Elele, River State, Nigeria age less than 5 years. The samples were kept in a clean, dry, disinfectant free container and were free from urine. The samples colleted were well labeled ready for analysis The samples obtained were inoculated aerobically on sterile blood agar, MacConkey agar, eosin methylene blue, Salmonella-Shigella agar,nutrient agar and nutrient broth at 370C for 24 hours. The colonies of each representative isolates were then characterized using standard bacteriological method according to Cowan and Steel3. Other tests included gram stain, pigment production, hemolysin production, motility indole, urea, citrate and hydrogen sulfide utilization, oxidase, and sugar fermentation were used to isolate the enteric gram negative bacteria. They were further sub culture on nutrient agar slants and stored at 40C for further analysis. Susceptibility Testing Susceptibility were determined both by overnight broth-micro-dilution and agar disk diffusion methods as recommended by Bauer et al.1 and National Committee for Clinical Laboratory Standard18 using Oxoid- Mueller Hinton agar (Difco Laboratories, Detroit, Mich). The following antibiotics were used to screen for the resistance of the isolates; ciprofloxacin- CPX (10µg), Peflacine- PEF (10µg), Ofloxacin- OFX (10µg), augumentin-AU (30µg), gentamicin- GN (10µg), streptomycin- S (30µg), chloramphenicol- C (10µg), ampicillin-PN (30µg) and cotrimoxazole- SXT (5µg) (Optun Laboratories Nig Ltd., Nigeria). The zones of inhibition were then measured and the results recorded as sensitive (s) or resistance (R) base on World Health Organization Drug Information28 and National Committee for Clinical Laboratory Standard18. Conjugation and Plasmids profiles Conjugation experiments were performed using E coli strains obtained from Nigerian Institute for Medical Research (NIMR) as recipient as previously described by Olukoya and Oni20, Yukata et al.29 and Wang et al.17. The donors and recipients-plasmid -free - rifampicin resistant strains were incubated both on broth culture (nutrient broth ‘E’-Antec Diagnostic Products, UK) and on Nutrient agar (nutrient agar-International Diagnostic Group UK) at 370C for 18 hours. The transconjugants were selected on nutrient agar medium supplemented with ampicillin 30µg/ml and rifampicin 200µg/ml to inhibit the growth of the donor and recipient respectively. The frequency of transfer of the plasmids was determined by dividing the number of transconjugants by the number of donor cells according to Wang et al.17 and Yukata et al.29. Curing experiments were carried out according to Miller16 and Olukoya & Oni20 The transconjugants were re-streaked onto fresh selective nutrient plates and their identities were re-confirmed on the basis of their biochemical methods and their antibiotics resistance confirmed. The Birnboim and Doly2 and Gummic11 methods were employed for screening plasmids (rapid alkaline extraction) of donors and transconjugants. The plasmids DNA were then electrophoresed on 0.8% agarose gel, stained with 14µl/g ethidium bromide. The DNA was then photographed with Polaroid camera and viewed using UV trans-illumination. The molecular weights and distances were then determined using standard methods according to Meyers et al.15 and Birnboim and Doly2 using standard DNA molecular weight marker II (0.12-23.1kbp) of bacteriophage lambda HindIII (Roche Diagnostic GmbH). RESULTS A total of 938 faecal samples of pediatric patients attending Madonna University Teaching Hospital (MUTH) from June 2003 to June 2004 were examined. Two hundred and eight (218) of eight different bacterial strains namely Escherichia coli 90(41.3%), Shigella dysenteriae 38(17.4%), Salmonella typhi 18(8.3%), Pseudomonas aeruginosa 20(9.2%), Staphylococcus aureus 7(3.2%), Proteus mirabilis 5(2.3%), Enterococcus faecalis 25(11.5%) and Klebsiella pneumoniae 15(6.9%) were isolated and identified as shown in Table 1. The susceptibility pattern of the isolate to the different antibiotics varied as shown in Table 2. Proteus mirabilis and Klebsiella pneumoniae were 100% sensitive to peflacine and Enterococcus faecalis was also 100% sensitive to ciprofloxacin and augumentin. Most of the isolates were least susceptible to cotrimoxazole; ampicillin, erythromycin, gentamicin, streptomycin and chloramphenicol. Pseudomonas aeruginosa were the most resistant strains of the pathogens to the various antibiotics with a resistant range of 0.0% to 55% as shown in Table 1. All the isolates were very sensitive to ofloxacin, pefloxacin and ciprofloxacin above 50% except Pseudomonas aeruginosa that had a percentage sensitivity of 35% to pefloxacin. The resistance plasmids to the various isolates were very diverse and distributive among the isolates as shown in Table 2. These plasmids were highly transferable with a high frequency range of 2x10-2 to 6x10-4. Some of the isolates had plasmids bands that ranged from ≤0.55kbp to ≥1.14kbp. Twenty-six percent of the isolates were plasmids mediated, 42% chromosome mediated while 32% of the pathogens were resistant to antibiotics could not be ascertained. E coli had the highest frequent plasmids distributive occurrence. The results indicate that the plasmids were able to move genetic antibiotics resistance materials among the various bacterial strains. Some of the isolates had plasmids bands that ranged from ≤0.55kbp to ≥1.14kbp ( Figures 1 and 2). DISCUSSION This report describes the high rate of antimicrobial resistance among diarrheal stools isolates and their plasmids profile obtained from MUTH pediatric patients. The result indicated that diarrhea posses a very serious problem in developing countries where it is the leading cause of morbidity and mortality among children19. The prevalence of Escherichia coli 90(41.3%), Shigella dysenteriae 38(17.4%), Salmonella typhi 18(8.3%) in this study were slightly higher to those obtained by Olukoya and Olasupo21 ten years ago. The prevalence of Shigella species isolated were also proportional to those obtained by Olukoya and Oni20 and Tjaniadi26. The increase in prevalence observed in this study is probably due to lack of education and public awareness on hygienic conditions. Diarrhea may be infective and non-infective but the fact remains that most of them are self-limiting and require adequate rehydration. In all doubtful cases, a stool examination should be done for ova; cyst, blood and hanging drop if cholera is suspected. Presence of leukocytes on blood- stains, usually suggests infection with Salmonella, Shigella, invasive E. coli, Yersinia, or E. histolytica. Use of antimicrobial therapy in diarrheal diseases would include patients with high fever, bloody diarrhea, severe dehydration, systemic toxicity, and immunosuppressed patients, and outbreak of food poisoning. From the result the susceptibility pattern of the isolate to the various antibiotics varied seriously with Proteus mirabilis and Klebsiella pneumoniae 100% sensitive to peflacine, Enterococcus faecalis 100% sensitive to ciprofloxacin and augmentin. Most of the isolates were least sensitive to cotrimoxazole, ampicillin, erythromycin gentamicin, streptomycin and chloramphenicol. The widespread resistance observed in the study could be due to the indiscriminate use and the over the counter availability of antibiotics as well as the higher exposure of people to enteric flora in places with poor hygienic conditions. The survey also demonstrated that isolates from diarrhea samples in MUTH especially strains of Escherichia coli, Shigella typhi, Pseudomonas aeruginosa, Proteus mirabilis and strains of Klebsiella pneumoniae harbored conjugative plasmids which may confer resistance to some of these antibiotics. Most of the plasmids screened were in agreement with those obtained by Olukoya and Olasupo21 who revealed that plasmid profiles differentiated specifically among Shigella isolates from Nigeria. The plasmids obtained in this work were smaller in sizes than those obtained by Olukoya and Olasupo21. These multiple copies of plasmid bands might have resulted from covalently close circular, open circular or linear forms of the same plasmid that might migrated at different rates on agarose gel electrophoresis. There was also a high degree of plasmids relatedness among the bacteria isolates from the various patients because of the presence of similar size plasmids especially 0.55, 0.79, 0.85, 1.08 and 1.14kbp. Traditionally, the role of antibiotics in antibiotic- induced antimicrobial resistance is to provide selective pressures to resistant clones. In 1990, Chakrabarty et al.13 re-ported the detection of nucleic acids in various antibiotics and the capacity of such nucleic acids to transform bacteria to drug resistance. Subsequently, Webb and Davies32 demonstrated that DNA encoding antibiotic resistance genes that are present in bacteria used in the production of antibiotics can be recovered in antibiotic preparations. It was proposed that anti-microbial resistance genes might be co-administered with antibiotics to humans or animals and taken up by bacteria in the hosts, contributing to the rapid development of antibiotic resistance30. The results also showed that conjugation was a very convenient method of transferring drug resistant genetic markers among intra and inter bacterial populations. This was shown by the high frequency of transfer among the isolates which was in accordance with the results of Wang et al.17 and Yukata et al.29. This wide spread transfer of antibiotics resistant markers has failed to eradicate microbial infections of diarrhea origin despite their benefits. Although there have been few previous reports focusing on diarrheal diseases, the high frequency with which antibiotics are used empirically to treat diarrheal diseases suggest that there might also be high rate of failure associated with enteric infections23. The use of antimicrobial agents in the treatment of diarrhea diseases has greatly improved the quality of life among residents and travelers in developing countries. However, the problems associated with microbial resistance in diarrhea patients still pose a challenge to public health works4,12. This challenge can be minimized if governments and associated public health providers can improve the hygienic condition. Also, a call to regulate the use of antimicrobial may be necessary to reduce the resistance to drugs. Government should also encourage the development of new vaccines to help reduce he incidence of emerging diarrheal diseases. Finally, the government and other health agencies should highlights the necessity of sanitary control system as well as monitor and regulate the use/distribution of antibiotics. These factors may help reducing childhood diarrheal infections of bacterial agents in developing countries, among diarrheal pathogens associated with decreased susceptibility to commonly prescribed antibiotics due to R-plasmids. Acknowledgements We are very grateful to the staff of Nigerian Institute of Medical Research (NIMR), Yaba Nigeria, especially Dr (Mrs.) S.I. Smith for her suggestion and contribution toward the realization of this work REFERENCES
The following images related to this document are available:Photo images[bk07006f2.jpg] [bk07006f1.jpg] [bk07006t1.jpg] [bk07006t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}