 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Biokemistri, Vol. 21, No. 1, June, 2009, pp. 17-24 Nutritional status, prevalence of some metabolic risk factors for cardiovascular disease and BMI-metabolic-risk sub-phenotypes in an adult Nigerian population Chukwunonso E. C. C. Ejike*1,2, Chidiebere E. Ugwu,2,3 and Lawrence U. S. Ezeanyika2,3 1Department of Biochemistry, College of Natural and
Applied Sciences, Michael Okpara University of Agriculture, Umudike PMB 7267
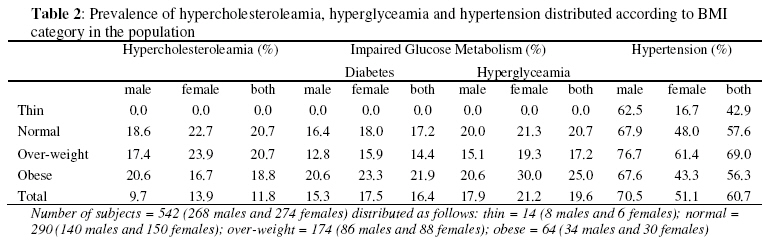
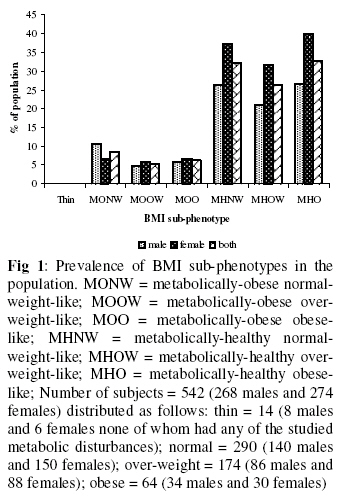
Umuahia Nigeria Received 21 April 2009 Code Number: bk09003 Abstract Studies have shown that metabolic risk factors associated with increased body mass index are the critical factors that confer risk for the chronic diseases associated with fat. The prevalence of these disorders is scarcely reported in Nigeria. We evaluated 542 adult Nigerians for nutritional status, serum total cholesterol, fasting blood glucose level and hypertension, using standard anthropometric and clinical methods. The results show that 32.1%, 11.8%, 19.6%, 11.8% and 60.7% of the population, irrespective of sex were over-weight, obese, hyperglycaemic, hypercholesterolemic and hypertensive respectively. Approximately 33% of the obese population were metabolically-healthy obese-like (MHO-like) while 8.6% of the normal BMI population were metabolically-obese normal-weight-like (MONW-like). Other sub-phenotypes were present at rates of 5 – 32% in the population. The results are discussed and compared to figures from other populations. Our data apparently supports the view that the assessment of metabolic risks for chronic diseases, irrespective of body mass index, may be more useful in identifying individuals or groups at risk of these disorders. Keywords: Body mass index, hypercholesteroleamia, hyperglyceamia, hypertension, prevalence INTRODUCTION Overweight and obesity are increasing at an alarming rate globally and developing countries appear to be the worst hit1 despite an increased awareness of the deleterious consequences of these conditions. Both disorders are often consequences of an imbalance in the energy intake and expenditure2,3 and are described by a body mass index (BMI) of 25-29.9 kg m-2 (over-weight) and more than 30 kg m-2 (obese). Obesity is a major risk factor for the development of chronic diseases and the associated mortality4,5. Visceral fat accumulation, which often accompany obesity, is associated with increased secretion of free fatty acids, hyperinsulinaemia, insulin resistance, hypertension, hyperglyceamia and dyslipidaemia6,7. Insulin resistance, which is an impaired biological response to insulin, is compensated for initially by the system, by an increased production of insulin such that with sustained insulin production and release, hyperinsulinaemia results. Since insulin stops the action of hormone sensitive lipase and lowers the level of carnithine in the liver, hyperinsulinaemia enhances the development of obesity8,9. This cyclic relationship may in part explain the difficulty observed in losing weight and sustaining such weight-loss in overweight and obese individuals, a phenomenon called weight cycling. Obesity is a complex disorder, involving the interaction of genetics with environmental factors to produce a heterogenous phenotype10. Studies have identified metabolically obese normal-weight (MONW) individuals who despite having a normal weight BMI, still have metabolic disturbances typical of obese individuals11-13. Other studies have described metabolically healthy obese (MHO) individuals, who, despite having BMI exceeding 30 kg m-2, still lack the metabolic abnormalities typical of obese individuals14-16. These phenotypes separate obesity from its usual metabolic consequences as seen in MONW individuals, or risks that are associated with obesity that are independent of adiposity as seen in MHO individuals. The prevalence of BMI-metabolic risk sub-phenotypes in community-based samples, especially in Africa, and Nigeria in particular is not known. The aim of this study is to provide data on: the nutritional status of adult Nigerians; the prevalence of hyperglyceamia and hypercholesterolemia in the population; and the prevalence of MONW-like and MHO-like individuals in the population. MATERIALS AND METHODS Adult Nigerian men and women (30-74 years of age) were studied. The participants were from Anyigba, Kogi State and Nsukka, Enugu State – both states are geographically contiguous with Kogi State bordering Enugu State to the North. The study was advertised locally in the two towns and those who gave informed verbal consent were allowed to participate in the study.The weights and heights of participants were taken, with subjects dressed in light clothing and the BMI calculated [weight (kg)/ height (m)2]. Subjects were grouped2,17 as thin (BMI<18.5), normal (18.5 ≤ BMI ≤ 24.9), overweight (25 ≤ BMI ≤ 29.9) and obese (BMI ≥ 30). Fasting blood samples (2ml) were drawn from each participant using a 4ml syringe, and transferred into clean sample containers. A drop of whole blood was removed from each container immediately and used for the measurement of whole blood glucose, by the glucose oxidase method18, using a glucometre (Accu-Chek Advantage, Roche Diagnostics, Mannheim, Germany). The glucometre was calibrated using standard test strips and solutions supplied by the manufacturer. Blood samples were allowed to stand at ambient temperature until clotting took place. The serum was separated completely by centrifugation for 5 minutes. From the serum, the total cholesterol concentration was measured by the method of Allain et al19. Subjects were grouped as being normo-cholesterolemic if they had cholesterol values of less than 5.17 mmol/L, and as being hyper-cholesterolemic20 if they had values ≥5.17 mmol/L. Subjects who had a fasting blood glucose level of >115 mg/dL were classified as having hyperglyceamia while those who had blood glucose levels ≤115 mg/dL were classified as having normal blood glucose levels. Those with hyperglyceamia were further divided into those with impaired fasting blood glucose levels (115 mg/dL to <125 mg/dL) and diabetic subjects (≥125 mg/dL)20. Age at last birthday as reported by each participant, was recorded. Blood pressure was measured using a digital blood pressure monitor (Omron model HEM-741 CINT, Omron Healthcare Inc., Illinois, USA). Three separate readings were taken (after a two minutes interval each) per individual (in a sitting position after an initial ten minutes rest) and the average of the second and third readings recorded. High blood pressure was defined as mean systolic blood pressure (SBP) ≥ 140mmHg and/or a mean diastolic blood pressure (DBP) ≥ 90 mmHg, or reported use of antihypertensive medication21. Subjects who had a cluster of hypercholesterolemia, hyperglycaemia and hypertension were described as metabolically-obese-like, while those who had normal values for the three parameters were described as metabolically-healthy-like. Based their BMI, subjects were then divided into: metabolically-obese normal-weight-like (MONW-like); metabolically-obese over-weight-like (MOOW-like); metabolically-obese obese-like (MOO-like); metabolically-healthy normal-weight-like (MHNW-like); metabolically-healthy over-weight-like (MHOW-like); and metabolically-healthy obese-like (MHO-like) sub-phenotypes.The study protocol was prepared in accordance with the Helsinki Declaration and was approved by the Human Experiments Review Board of the Department of Biochemistry, Kogi State University, Anyigba, Nigeria Statistical analysis Differences between means were checked for significance using the one way ANOVA and multiple comparison tests. Differences between means were significant at p<0.05. Analyses were performed using SPSS for windows version 11.0 (SPSS Inc, Chicago, IL). RESULTS A total of 542 subjects (268 males and 274 females) were studied. Of the 268 males, more than half (52.2%) had a normal BMI while approximately 13% were obese. The differences in the ages of the males (Table 1) who were thin, over-weight or obese, compared to those who had normal BMI were not statistically significant (p>0.05). For the females, approximately 32% were over-weight and about 11% were obese, while more than half of the population had normal BMI. As was with the males, the differences in ages of subjects in the different BMI groups compared (Table 1) to those with normal BMI were not significant (p > 0.05). A total of 11.8% (9.7% for males and 13.9% for females) of the entire population were hypercholesterolemic. None of the thin subjects (males and females alike) were affected by the disorder. Women were more affected than men (Table 2). The prevalence of hypercholesterolemia (disregarding the thin subjects) was highest among over-weight women (23.9%) and least among obese women (16.7%). For both males and females, obese subjects had the most impaired fasting blood glucose profile, followed by normal BMI subjects, over-weight subjects and thin subjects, in that order. In fact none of the thin subjects had an impaired blood glucose metabolismwhile one in four of the obese subjects had an impaired FBG. The same trend was noticed for the prevalence of diabetes mellitus in the population. In each BMI category (except in thin subjects), more females were affected by diabetes mellitus and/or impaired FBG than males (Table 2). From Table 2, it seen that hypertension was very prevalent in the population. Approximately 61% of the population (70.5% for males and 51.1% for females) was hypertensive. The prevalence of hypertension was least in thin subjects and highest in over-weight subjects, while normal BMI and obese subjects had similar prevalence rates. In all BMI groups, men were markedly more hypertensive than women. Approximately 33% of the obese population (26.5% for males and 40.0% for females) were metabolically-healthy obese-like (MHO-like). More over-weight females (31.8%) than males (20.9%) were metabolically-healthy over-weight-like (MHOW-like). The same was observed for metabolically-healthy normal-weight-like subjects in the normal BMI group (37.3% for females and 26.4% for males). On the other hand, more males (10.7%) than females (6.7%) having normal BMI, were metabolically-obese normal-weight-like (MONW-like). Only 5.2% of the over-weight population (4.7% for males and 5.7% for females) was metabolically-obese over-weight-like (MOOW-like). Also, only 6.3% of the obese population was metabolically-obese obese-like (Fig 1). DISCUSSION BMI is an acceptable index for estimating the nutritional status of a population2. Thinness is often as a result of chronic energy deficiency, except in cases of illness, while obesity is an indication of excessive energy intake without a commensurate level of physical activity. More than half of the population we studied had normal BMI, suggesting a balance between energy intake and expenditure. However, about 12% of the population was obese while as much as 32% were over-weight. This shows that as much as 44% of the population weighed more than was desirable. This is particularly high when compared to figures from the Nigeria demographic and health survey22 that reported 15% over-weight and 5% obesity in women. Our data also shows that the males have surpassed the 26% obesity prevalence projection of the WHO23 for the year 2010, while the women were slightly below the projected 36% prevalence in Nigeria. More females in our study were hypercholesterolemic compared to the males. The 9.7% and 13.9% for males and females respectively reported here are higher than figures reported elsewhere in rural Africa (0–2.8%) but lower than 26–50% reported in more developed African countries23-27. The 16.4% prevalence of suspected-diabetes reported in this study is very high. Reports from elsewhere in Africa show a prevalence of 1% in rural Africa, 5-7% in sub-Saharan Africa and between 8% and 13% in more developed areas like South Africa28,29. This is very worrisome especially in view of the association of diabetes with such macrovascular complications as coronary artery disease (CAD), cerebrovascular disease and peripheral vascular disease1. The prevalence of hyperglyceamia was naturally higher than that of suspected-diabetes since some individuals had more fasting blood glucose than is desirable but were not diabetic. The prevalence of hypertension in this study (60.7%), like suspected-diabetes, is also very high. Figures from other parts of Africa are lower [19–30%] in population based studies23,25,27 but slightly higher in hospital-based samples30,31. The role of hypertension in exacerbating cardiovascular diseases is well documented in epidemiologic literature. Its ability to result in morbidity and mortality make this high prevalence rate worrisome especially in a population that is battling with infectious diseases, like ours. Our data, more importantly, show that there are BMI-metabolic risk sub-phenotypes in Nigeria. This is important since it has been suggested that the metabolic consequences of elevated BMI are the critical factors that confer risk for the chronic diseases associated with fatness32. The prevalence of MONW-like phenotype is put at 3 – 28% depending on the definition of metabolic risk and the population source13,33-35]. Our figure of 8.6% is therefore one of the lowest reported. MHO-like phenotypes have been reported to occur in 11 – 28% of some populations14,33,36,37. The 32.8% prevalence of MHO-like phenotype in our study is higher than these. This is instructive since it implies that approximately 9% of those who had normal BMI were actually at high risk of cardiovascular disease (CVD) while as much as about 33% of the obese subjects were actually at low risk. Meigs and colleagues32 showed that normal-weight subjects with the metabolic syndrome but not obese subjects without the metabolic syndrome were at substantially elevated risk for CVD over 7-11 years of follow-up. Our data further highlights that though only 8.6% of the normal-weight group was metabolically obese-like, only 32.1% of the same group had a healthy profile (MHNW-like) with respect to the parameters measured. Furthermore, though only 5.2% of the over-weight group was metabolically obese-like, only 26.4% of the same population was MHOW-like. Again, though only 6.3% of the obese population was metabolically obese-like, only 32.8% of that group was MHO-like. The implication is that a vast majority of the population had one unfavourable metabolic index or the other, and may therefore have varying degrees of risk of CVD. It has been suggested that apparently healthy obese individuals may have sub-clinical vascular disease38. Our data therefore supports the view that metabolic factors associated with adiposity were more important than fatness with respect to the development of CVD and the associated morbidities. Caution must however be exercised in interpreting this data especially when extrapolating it for the general population. This is because our data is not cross-sectional and this may have introduced some bias as possibly those who knew they were hypertensive and needed help were more willing to participate in the study. This may explain the high prevalence of hypertension in the population. Furthermore, we could not assay for insulin resistance and all the components of the metabolic syndrome in the population. This may imply an under-estimation of the population at risk of these disorders. Our study is however fairly large and informative, especially as this population is rather under-studied. In conclusion, the prevalence of over-weight and obesity in the population is high (44%). Hyperglycaemia and hypercholesterolemia were significantly prevalent (19.6% and 11.8% respectively), while the prevalence of hypertension is very high (60.7%). Phenotypes of the BMI metabolic risk were present in the studied population. We found the MONW-like and MOOW-like phenotypes on the one hand and MHO-like and MHOW-like phenotypes on the other hand, at fairly high prevalence rates. We conclude that as with other populations where these phenotypes have been found, the assessment of metabolic risk, regardless of BMI, may be better for the identification of individuals and groups at risk of the development of cardiovascular disease and its co-morbid conditions. REFERENCES
© 2009 Nigerian Society for Experimental Biology. The following images related to this document are available:Photo images[bk09003t2.jpg] [bk09003t1.jpg] [bk09003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}