 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Biokemistri, Vol. 21, No. 2, Dec, 2009, pp. 53-58 Serum Level of Antioxidant Vitamins (Vitamin A, C and E) in Plasmodium falciparum Malaria Infected Children in Owerri, Eastern Nigeria Raphael C. Ekeanyanwu1*, Nkem Achuka1 and Benjamin U. Akpoilih2 1Biochemistry Unit, Department of Chemical
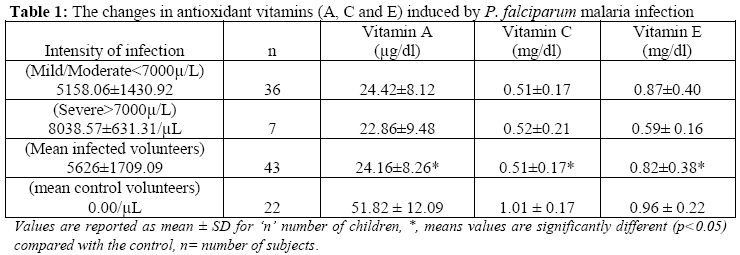
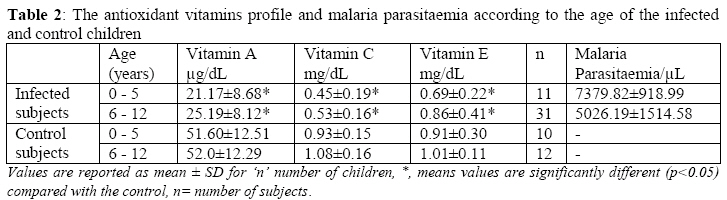
Sciences, Novena University, Ogume, Delta state Received September 11, 2009 Code Number: bk09007 Abstract The levels of antioxidant vitamins were estimated in Plasmodium falciparum malaria infected children. Forty-three children with P.falciparum infection were selected based on the clinical symptoms. Twenty-two apparently healthy children with no malaria parasitaemia were included as the control subjects. P.falciparum parasitaemia and serum levels of the antioxidant vitamins (vitamin A, C and E) were determined using standard procedures. It was observed that all parameters measured were significantly lower in malaria infected children when compared with the respective control values. The relationship between malaria parasitaemia and serum concentration of vitamin E were positively correlated (r= 0.42), but vitamin A (r= -0.05) and C (-0.06) were negatively correlated. Children within 0-5 years of age had higher malarial parasitaemia (7379.82 ± 918 99/µL) than those between 6-12 years of age (5026.19 ± 1514.58/µL), and these children had lower concentrations of vitamin A (21.27 ± 8.68 µg/dL), C (0.45 ± 0.19 mg/dl) and E (0.69 ± 0.22 mg/dL) when compared with children between 6-12 years (vitamin A = 25.19 ± 8.12 µg/dL, vitamin C = 0.53 ± 0.16 mg/ dL and vitamin E = 0.86 ± 0.41 mg/ dL). Results suggest that in Owerri, Eastern Nigeria, the degree of malaria parasitaemia in especially children between 0-5 years could comprise immunity (as judged by the correlation) and reduce serum antioxidant vitamin levels. Health care providers should recognize these effects in planning malarial treatment and control programs. Changes in serum antioxidant levels during post-treatment periods should be investigated and documented. Keywords:Vitamin A, Vitamin C, Vitamin E, Plasmodium falciparum, Children. INTRODUCTION Malaria is essentially a tropical disease occurring in regions between latitude 620 N and 400 S with an altitude of 1,500m. This region is formed mainly within the tropics and subtropics and this makes malaria endemic in this zone1. There are two epidemiological extremes of malaria known as stable and unstable malaria2. Epidemiological factors that make malaria endemic in the tropics include climatic factors (relative humidity, altitude, rainfall level, mean temperature between 18-190C) and socioeconomic factors, as all these have effects on the availability of vectors which maintain that transmission of malaria2. Malaria can be transmitted by three known ways; vector transmission3, blood transfusion4 and Congenital transmission5. Malaria is caused by the plasmodium species and is a major cause of morbidity and mortality in developing countries6. It affects 300 - 500 million people and kills 1.5 - 2.7 million people annually. The majority of these cases are children where the disease can exist in a severe form, often with devastating consequences7. The wide spectrum of malaria morbidity and mortality is dependent largely on the complex pathogenesis of this parasitic infection. Micronutrient statuses have been shown to influence resistance to several infectious diseases including measles and diarrheal and respiratory disease8,9. Micronutrients are known to influence the disease progression in man. For instance, a randomized trial has shown that periodic Vitamin A supplementation could reduce the incidence of febrile episodes and parasitaemia due to Plasmodium falciparum in Papua, New Guinea8. Vitamin A is essential for normal immune function and has been shown to influence both antibody responses and cell mediated immunity10. Strong antioxidants such as dietary carotenoids and Vitamin E have been shown to modulate immune functions in humans. Vitamin C concentrations correlated with white cell count, alpha-1- acid glycoprotein and IL-6, all of which are markers of inflammation11. Vitamin C can also rejuvenate Vitamin E, making it an indirect contributor to fighting free radical damage in membrane lipids12. These free radicals are products of oxidative stress that is aggravated in malarial infection to decrease the antioxidant defence system. One of the consequences of oxidative stress is the development of malarial anaemia13,14. Thus the overall antioxidant status will give more relevant biological information compared to that obtained by the measurements of individual components15. In Caucasians, a reference range of 1.30 – 1.78 mmol/L has been reported16. Akpotuzor et al.15 reported an Antioxidant range of 0.84 – 1.68 mmol/L in Nigerian subjects. It has been argued that vitamin E deficiency might be protective against malaria in mice17, but this relationship in humans is not well understood. It has been documented that antioxidants such as carotenoids and Vitamins C and E could provide protection against oxidative stress induced by malaria18. Despite the role of these antioxidants could play in malarial pathogenesis, there is limited information on the antioxidant profile among children with P. falciparum malaria in Nigeria and Owerri in particular. To gain insight into this, we investigated the antioxidant profile among Nigerian children diagnosed with P. falciparum malaria and studied the correlation between antioxidant concentrations and malarial parasitaemia. MATERIALS AND METHODS The study was conducted in Owerri, Imo State, Nigeria, between June 2009 and August 2009. Owerri town lies on latitude 5.485o N and longitude 7.035oE and is located in a rainforest belt of Imo State, endemic for Plasmodium falciparum malaria parasite which is transmitted by the female Anopheles mosquito. It has a rainy period from April to November which is when the bite of mosquitoes is more rampant. The rainforest belt where the state is located is also a very good site for mosquito habitat. Owerri has a population comprising workers in the private sector, civil servants, students, traders, self employment etc. The study subjects consist of sixty-five children between the ages of 1-12 years who attended the pediatric clinic of Federal Medical Centre, (FMC) Owerri, Nigeria. The study subjects were children (43) infected with Plasmodium falciparum malaria parasite, who reported ill with fever (axillary temperature >37.5oC), headache, vomiting, diarrhea, respiratory distress and other clinical signs and symptoms of malaria, as previously documented19 and also have not been placed on any anti-malaria drug. The children who did not meet these criteria were excluded from the study. Apparent healthy children, consisting of 22 subjects who were found to be negative for Plasmodium falciparum in their peripheral blood were used as controls. Both groups of subjects must have resided in the city of Owerri for at least one year before the study. The scope nature and objective of the investigation were thoroughly explained to the parents/guardian of the children for their consent, which was sought and obtained. Plasmodium falciparum parasitaemia was determined in peripheral blood smears stained by Giemsa stain. The thick and thin films were analysed for the number of parasites per 200 white blood cells. Slides were considered negative if no parasites were seen in 100 fields in the film. Serum Vitamin A assay was by the method of Olson et al.20, serum Vitamin E assay was by the method of Kaser and Stekol21, and serum Vitamin C assay was by the method of Roe and Kuether22. The data obtained in this investigation were subjected to statistical analysis. RESULTS The antioxidant profile and intensity of infection (malarial parasitaemia) of the volunteers are presented in Table 1. The control children had higher mean concentration of vitamin A (51.82±1209 µg/dl) and these differences were statistically significant at p < 0.05 when compared with the infected counterparts. The mean concentrations of vitamin C (1.01 ± 0.17 mg/dl) and vitamin E (0.96± 0.22mg/dl) in the control children were statistically significant (p<0.05) when compared with their infected counterparts. The relationship between malarial parasitaemia, vitamin A and the vitamin C were negatively correlated with r = - 0.05 and r = -0.06, respectively. The level of vitamin E strongly and positively correlated with the malarial parasitaemia (r = 0.42). The antioxidant vitamins profile and malaria parasitaemia according to the age of the infected and control children are presented in Table 2. Children between 0-5 years old had the highest Plasmodium falciparum load of 7379.82 ± 918.99 in their peripheral blood. Also, these children had a lower vitamins E concentration (0.69 ± 0.22 mg/dl) than those between 6 – 12 years of age (0.86± 0.41mg/dl). The vitamin A (21.27 ± 8.68µg/dl) and vitamin C (0.45 ±0.19mg/dl) were lower in younger children within 0-5 years but were higher in those children between 6 – 12 years when compared. However, there was significant difference (p<0.05) in the Vitamin A, C and E levels of the malaria infected children, 0-5years of age and 6-12 years of age compared with their control counterparts. DISCUSSION The antioxidant vitamin levels in malaria patients were lower than the levels for control. The lower values observed in antioxidant vitamin levels in malaria may be attributed to increased utilization of the host’s serum antioxidants by the malaria parasites to counteract oxidative damages15. It was observed that vitamin A concentration in P. falciparum infected children was significantly lower (p < 0.05) than in the control subjects (Table 1). This observation confirms earlier reports7,23. This study however, implicates vitamin A deficiency as an important component of P. falciparum in Owerri, Eastern Nigeria. This observation is considered valid considering the role of vitamin A as an essential micronutrient for normal immune function, which influences antibody responses and cell mediated immunity7,10. The lower concentrations of vitamin A and vitamin C observed among 0-5 years old children correlated with higher malarial parasitaemia. From present study, a lower concentration of vitamin E in the serum P. falciparum-infected children was observed than that of the control volunteers (Table 1). This agrees with the investigation of Nmorsi, et al.7 performed in Ekpoma, Edo state, Nigeria and Das et al.12 performed in India, where they documented that children with both severe and mild malaria had significant lower plasma vitamin E concentrations than the control children without malaria. The low concentration of antioxidant vitamin E and C in the infected children may be in part due to increased utilization of serum antioxidants or increased destruction during the malaria infection. Their transfer to red blood cell membrane to counteract the increase oxidative stress during acute phase of the disease by inhibiting membrane lipid peroxidation may be a contributing factor7. It was observed that the children within the first 5 years of age had lower concentrations of vitamin E than those between 6-12 years who had lower parasitaemia (Table 2). But previous investigation carried by Nmorsi et al.7 showed that the children within the first 5 years of age had higher concentrations of vitamin E than those 6–12 years of age who had lower parasitaemia. They concluded that these micronutrients, which increased with higher malarial parasitaemia, may have protective effects against malaria in their Ekpoma region. This lends support to an earlier hypothesis that antioxidants such as vitamin E may offer protection against the oxidative stress induced by malaria infection24. However, Metzger et al. 25 observed that low concentrations of vitamin E in serum were not associated with parasite clearance, which is not consistent with the hypothesis that low vitamin E status is protective against malaria17. Overall, the depressed antioxidant concentrations in the children who had malaria indicated the impact of P. falciparum infection on the antioxidant status of children in Owerri, Eastern Nigeria. This observation adds to the accumulating reports7,25,26,28. This observation can be further proved valid by the deduction of Akpotuzor et al15 and Nmorsi et al.7 who indicated that antioxidants are used to counteract the effects of free radicals generated in the presence of malaria. This also explained the negative correlation reported between the intensity of infection and the antioxidant concentrations among the infected children in our study area. This pattern of antioxidant status is a reflection of the malarial pathogenesis, which involves the invasion of human erythrocytes by the malaria parasite. This brings about metabolic changes in the host cell. The host cells may then become vulnerable to damage due to toxic metabolites derived from both host and parasites. Reactive oxygen species generated in the host-parasite interaction cause the lysis of erythrocytes and alteration of antioxidants7,27,29 thus leading to the development of malarial anemia7,13,14. From our observations in this study, the serum concentrations of antioxidant vitamins were reduced in malaria and reduction of these antioxidants in turn caused the reduction of the total antioxidant levels of malaria-infected children. It was also noted however that antioxidant levels in our controls were higher than values observed in infected subjects. However, lowered levels of antioxidants, especially of vitamin C in malaria infection also suggest lowered immunity of host which may be responsible for some of the complications of malaria infection. The reduction of these antioxidants in the stages of malaria infection may expose the children to free radical attack. To reverse this condition and reduce the morbidity due to Plasmodium falciparum, it is necessary to recommend antioxidant agents (particularly vitamin C) as a component of drugs for treatment of malaria infection. Foods rich in antioxidants such as vegetables, fruits (oranges, banana, apples, etc), red palm oil and so many more should also be part of diet recommended for the management of malaria and the outcome of such supplementation should be investigated and derived, documented for further advice. REFERENCES
© 2009 Nigerian Society for Experimental Biology. The following images related to this document are available:Photo images[bk09007t1.jpg] [bk09007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}